
Abstract
Aims:
The aim of this study to determine the expression of MMP-28 in bladder urothelial carcinoma and to analyze the correlation between MMP-28 and the clinicopathological characteristics of human bladder carcinoma, and its relationship with patient prognosis.
Methods:
A total of 491 surgically resected bladder cancer samples and 80 normal tissue adjacent to the tumor were stained by immunohistochemistry. The expression of MMP-28 in these samples was quantitated, and the value of MMP-28 as a marker of bladder cancer and prognosis was assessed.
Results:
The expression of MMP-28 in urinary bladder carcinoma was higher than in normal bladder mucosa. The high level of MMP-28 was significantly correlated with tumor histology grade, lymphatic metastasis, lymph node infiltration, and distant metastasis (P < 0.05). The upregulation of MMP-28 was also closely related to the risk of cancer progression and the survival of patients. Further analysis documented that high expression of MMP-28 was associated with decreased overall survival in bladder cancer patients.
Conclusions:
The abnormal expression of MMP-28 may be related to the initiation and development of urothelial carcinoma. The upregulation of MMP-28 can be used as one of the effective indicators to diagnose bladder cancer and predict tumor progression.
Introduction
Bladder cancer is one of the most common malignant tumors of the urinary system. The incidence of bladder cancer increases continuously, and it ranks as the seventh most frequent tumor in men. 1 In its early stages, bladder urothelial carcinoma lacks clear clinical symptoms, and is highly metastatic in the late stages, resulting in a high mortality rate. 2,3 During the transition from early to late stages, bladder cancer undergoes a complex pathological process, which makes its treatment more difficult. At present, 4 types of bladder cancer therapy are being used: surgery, chemotherapy, radiation therapy, and combined immunotherapy. In particular, radical resection of bladder cancer has been widely used in clinical practice as a standard treatment for muscle-invasive bladder cancer. Unfortunately, nearly half of the patients develop metastases and die within 2 years after cystectomy. 4 -6 Although with the progress in surgical techniques and chemotherapy in the past few decades the mortality of bladder cancer has been declining, the overall 5-year survival rates did not improve significantly. 7 Therefore, the search for novel markers of bladder cancer and therapeutic targets remains the main goal of research in the field of bladder cancer treatment. 8
Matrix metalloproteinases (MMPs) is a family of zinc-dependent endopeptidases comprising 23 structurally related enzymes capable of degrading the extracellular matrix and regulating the activity of growth factors and cytokines. Moreover, MMPs have an important functional role in various physiological activities in the human body, such as growth and development, inflammation, wound healing, and angiogenesis. 9 -12 Several studies demonstrated that the upregulation of MMPs is related to tumorigenesis and can affect tumor progression.
MMP-28, also known as epilysin, belongs to the MMP19 subfamily of MMPs. Its structure includes the prototype domain of MMP and the furan activation sequence that is always stimulated in the secretory pathway. MMP-28 is localized on the plasma membrane of cells and is expressed in a variety of normal and tumor tissues. 13 -15 Among normal tissues, MMP-28 has been detected in rhesus monkey placenta during early pregnancy, human dermal keratinocytes at the edge of wounded skin and locations distant from the wound; its expression is upregulated in conditions of demyelination in vivo of human. 16 -18 At the same time, MMP-28 also plays an important role in the development of several types of cancer. 14,17 Its expression has been demonstrated in cells of colon, pancreatic, ovarian, prostate, and lung cancers. 17
Given the important physiological effects of MMP-28 on the development of embryos and tumors, we have raised the hypothesis that the expression of MMP-28 can predict tumor occurrence and cancer prognosis. To further understand the role of MMP-28 in the urinary system, the present study was designed to evaluate the activation and expression of MMP-28 in urothelial carcinoma and determine whether the MMP-28 gene is stably overexpressed in cells.
Materials and Methods
Patient Population and Samples
Tissue specimens were collected from 491 cases of bladder cancer (patients age: 35-79 years, median: 63.2 years) from January 1998 to December 2011 in the Zhejiang Provincial People’s Hospital. The samples included 102 cases of a single tumor and 389 cases of multiple tumors. According to the 2004 WHO pathological classification standard, 38 cases corresponded to a low-grade urothelial carcinoma and 453 cases to a high-grade urothelial carcinoma. The TNM staging following the 2009 method of the Union for International Cancer Control identified 67 cases of non-muscle-infiltrating bladder cancer and 424 cases of muscle-infiltrating bladder cancer. All patients had been followed up for more than 5 years from the time of surgery to December 2017 or death. The main causes of mortality were cancer metastasis and recurrence. Eighty control samples were collected from the tissues located more than 5 cm from the tumor edge. All specimens were fixed with formaldehyde and paraffin-embedded. A tissue microarray instrument to select the core tissue biopsy (2 mm diameter) of the most aggressive part of the target area of each tissue block in a paraffin block (tissue array block). The study was approved by the ethics committee of the Zhejiang People’s Hospital (IRB:2020QT218), and all patients signed the informed consent.
Immunohistochemistry and Analysis
The expression of MMP-28 was detected by immunohistochemistry. Briefly, from each tissue array block, a 4 µm thick continuous section was cut, slides with the sections were placed in an oven, baked at 60°C for 2 hours, deparaffinized in xylenes, rehydrated with an ethanol concentration gradient, microwaved in a 10 mM citric acid buffer for 15 minutes for antigen retrieval. Subsequently, the sections were blocked with 3% hydrogen peroxide for 10 minutes to inhibit endogenous peroxidase activity and with 1% bovine serum albumin to prevent nonspecific binding. Sections were then incubated with an anti-MMP28 (Santa Cruz Biotechnology Inc, Delaware Avenue, CA) mouse monoclonal antibody at 4°C for 16 hours, washed, and treated with the secondary antibody (Envision). Goat serum was used as a negative control. Finally, tissue sections were counterstained with hematoxylin, dehydrated, and a coverglass was mounted.
Immunostaining scores based on staining intensity and the fraction of stained cells were assigned independently by 2 individuals with no knowledge of the pathological and clinical data. In case of differences, the consistent score will be selected for evaluation. Staining intensity was graded according to the following standards: 0 points were assigned for the absence of staining, 1 point for weak or light yellow staining, 2 points for moderate or brownish-yellow staining, 3 points for strong or tan staining, staining of less than 5% of cells was assigned 0 points, staining of 6-26% of cells was assigned 1 point, staining of 26-50% of cells was assigned 2 points, and staining of more than 50% of cells was assigned 3 points. The final score was calculated by multiplying score for the fraction of positive cells by the staining intensity score: The expression level of MMP-28 was consider low if the score was 0-4 points and high if the score was 5-9.
Statistical Analysis
Application of SPSS V.16.0 statistical software to assess the correlation between MMP-28 expression and clinicopathologic characteristics of bladder cancer patients. The measurement data were analyzed using the Student’s t-test, and the categorical data processing were using the Fisher exact test or the Χ 2 test [2]. Survival curves were assessed by the Kaplan-Meier method, and logarithmic order validation was used to verify differences between the curves. Multiple survival analysis with the model and evaluation of the prognostic value of protein expression were performed using the Cox ratio. The associated coefficients were considered statistically significant at P < 0.05.
Results
Expression of MMP-28 in Bladder Cancer Tissues
The expression of MMP-28 was located predominantly in the cytoplasm of bladder cancer cells (Figure 1). Among the 80 control samples of the bladder mucosa, the MMP-28 protein was detected in 8 cases (10.0%), but the level of its expression was consistently low. Among the 491 tumor tissue samples, MMP-28 protein was detected in 333 cases (67.82%), a value significantly higher than in control samples of non-neoplastic bladder mucosa (P < 0.01). Figure 1 shows the plot of scores for MMP-28 immunostaining in the analyzed tissues.

Immunohistochemical staining for MMP-28 in urothelium tissue adjacent to the tumor and cancerous bladder tissue. A1-A3: Immunostaining of MMP-28 in urothelium tissue adjacent to the tumor. B1-B3: Strong staining (yellow-brown granules, mainly in the cytoplasm) in nonmuscle-invasive urinary bladder carcinoma. C1-C3: Strong staining in muscle-invasive urinary bladder carcinoma. Magnification: the original magnification ×40 (A1-C1), ×100 (A2-C2), and ×400 (A3-C3).
Relationship Between MMP-28 Expression and Bladder Cancer Clinicopathological Parameters
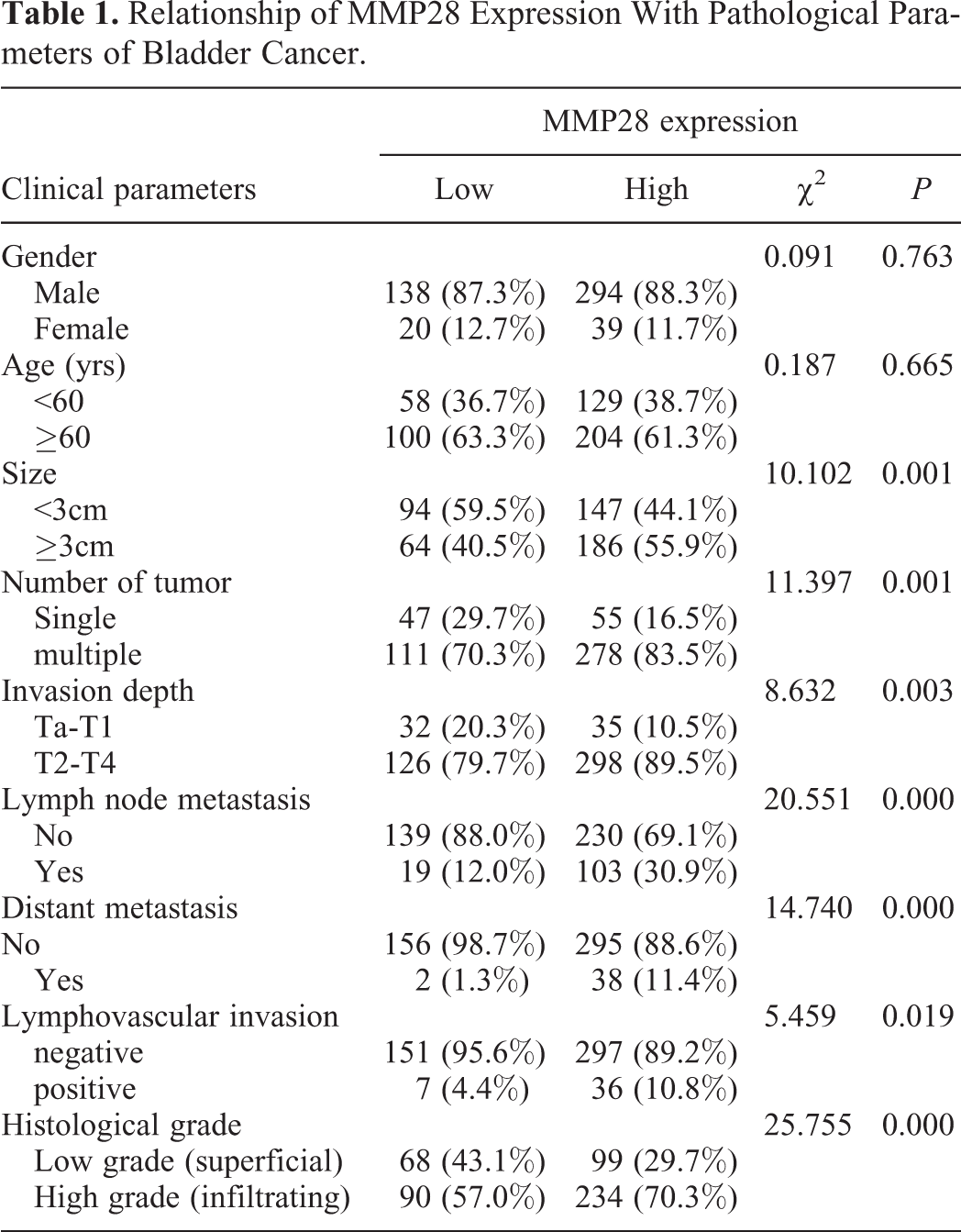
MMP-28 expression was correlated with tumor size, the number of tumors, histological grade, infiltration depth, lymph node metastasis, vascular invasion, and distant metastasis (P < 0.05). The age or gender of patients did not affect these correlations. The expression of MMP-28 was significantly upregulated in patients with the size of tumor was large, deep infiltration (stages T2-T4), multiple tumors, lymph node metastasis, distant metastasis, and advanced bladder cancer (Table 1). Spearman correlation coefficients of MMP-28 expression and the characteristics of bladder cancer were 0.143 for tumor size, 0.152 for the number of tumors, 0.133 for infiltration depth, 0.204 for lymph node metastasis, 0.162 for tumor histological grade, and 0.173 for distant metastasis (P < 0.05 in all cases).
Relationship of MMP28 Expression With Pathological Parameters of Bladder Cancer.
Survival Analysis
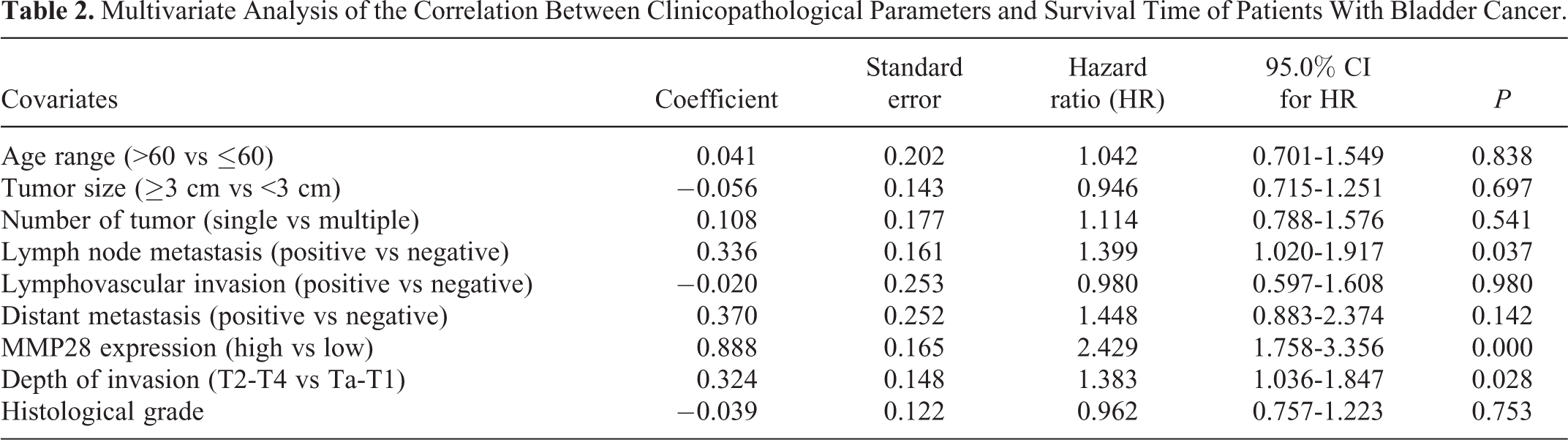
Patients with high MMP-28 expression had a significantly lower mean survival time (35.65 ± 1.47 months) than those with a low MMP28 level (56.36 ± 1.25 months, P < 0.001). Kaplan-Meier survival data showed that high MMP-28 expression (Positive) was associated with poor overall survival when compared to low expression (Negative) of MMP-28 (P < 0.001, Figure 2). The prognostic factors for the postoperative recurrence of bladder cancer were analyzed by the multivariate Cox proportional risk regression and documented that independent risk factors include infiltration depth (P = 0.028), lymph node metastasis (P = 0.037), and MMP-28 expression (P < 0.001). Conversely, patient age, tumor size, number of tumors, lymphatic vessel infiltration, distant metastasis, and histological classification lacked prognostic value (Table 2).

Kaplan-Meier survival curves of urinary bladder carcinoma patients with positive and negative MMP-28 expression.
Multivariate Analysis of the Correlation Between Clinicopathological Parameters and Survival Time of Patients With Bladder Cancer.
Discussion
Although some progress in the diagnosis and treatment of bladder cancer, one of the most common malignancies of the urinary system, has been made in recent years, the prognosis remains poor. Several markers such as NMP-22 and bladder cancer antigen (BTA) have been employed, but additional bladder cancer markers such as microsatellite analysis, telomerase, and survivin are still undergoing preclinical evaluation. 10,11,19 Increased expression of NMP-22 is widely used in the detection of benign or malignant tumors, including bladder cancer. However, other studies on NMP-22 have shown that its clinical application is limited due to the low overall sensitivity and specificity of detection. 20 Therefore, the search for better, more reliable, and noninvasive markers of bladder urothelial carcinoma that can be used for early diagnosis and postoperative monitoring of bladder cancer is an important research direction in urology.
MMPs are metal-dependent extracellular proteinases not commonly expressed in normal tissues. Their expression and activity increase after injury, and during inflammation and tumor development. 21 However, MMP-28 differs from many traditional MMPs in that it can be expressed in cells of normal tissues, such as keratinocytes, developing testicular germ cells, and basal layer cells of the lungs and skin. 14,17 Overexpression of MMP-28 can predict the survival of glioblastoma 22 and gastric cancer 23 patients. Although previous studies have demonstrated the potential of MMP-28 as a tumor marker, the correlation between its expression and clinicopathology of bladder cancer has not been reported.
At present, the depth of tumor infiltration, lymph node metastasis, and distant metastases are considered to be the factors influencing the prognosis of bladder cancer patients. The findings of the current investigation have shown that MMP-28 is an independent predictor of prognosis, and its overexpression in tumor tissues is closely related to the poor outcome in bladder cancer patients. Further analysis of the mean survival time revealed that the survival time of bladder cancer patients with an upregulated expression of MMP-28 was significantly shorter, suggesting that this protein may be used as an effective objective marker in the assessment of the invasion and progression of bladder cancer.
The present work analyzed the relationship between the expression of MMP-28 measure by immunohistochemistry and the clinicopathological features and prognosis in 491 cases of bladder cancer. Quantitation of immunostaining documented that the expression of MMP-28 in bladder cancer cells was significantly higher than in normal bladder tissue, suggesting the potential use of MMP-28 as a marker of bladder cancer. The analysis of the correlation between clinicopathological characteristics and MMP-28 staining indicated that the fraction of stained cells was higher in bladder cancer characterized by a large size, multiple tumors, and a high histological grade. This correlation indicates that the higher is the bladder cancer malignancy, the higher is the expression of MMP-28. In addition, the level of MM-28 is closely related to tumor metastasis. The collected data demonstrated also that MMP-28 expression correlates with the depth of tumor infiltration, lymph node metastasis, vascular infiltration, and distant metastases, but not with the age and gender of patients.
It has been shown that MMP-28 promotes the development of cancer by inducing epithelial cells to acquire a mesenchymal phenotype, which is characterized by TGF-β-dependent invasiveness. 24 Therefore, we analyzed the prognostic value of elevated expression of MMP-28 for overall survival in bladder cancer patients. Kaplan-Meier analysis revealed a statistically significant correlation between high expression of MMP-28 and poor overall survival, i.e. patients positive for MMP-28 had a higher risk of death than those negative staining. In addition, the total survival time of bladder cancer patients with upregulated MMP-28 expression was shorter in patients with low MMP-28 expression. Thus the expression of MMP-28 is an independent prognostic factor for bladder cancer.
In conclusion, the current investigation evaluated the expression of MMP-28 and the overall survival rate in patients with bladder cancer. The collected results indicate that MMP-28 can predict the prognosis of these patients, revealing an additional oncogene in the urinary system. Therefore, MMP-28 can be used as an important molecular marker of the onset and development of bladder cancer, and serve as an effective indicator of prognosis. Future research may further clarify its function in the malignant behavior of bladder urothelial carcinoma, and provide the basis for bladder cancer therapy.
Footnotes
Abbreviations
Authors’ Note
ZQ, YX and WHJ analyzed and interpreted the patient data regarding the bladder cancer. WJX, CXP and WHB performed the histological examination of the tissue. WH was a major contributor in writing the manuscript and ZDH, YX edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Grants from natural science foundation of Zhejiang province (GF19H160084) and Zhejiang traditional Chinese medicine administration (2017ZZ002).