
Abstract
Background
Endometrial carcinoma (EC) represents a unique clinical challenge. Fertility-sparing treatments rely on achieving complete response (CR) through progesterone-based therapy. We sought to investigate the prognostic value of molecular subtyping and immunohistochemical (IHC) markers in predicting three-month treatment outcomes and recurrence in EC patients undergoing fertility-sparing therapy.
Methods
A retrospective cohort of 68 patients diagnosed with early-stage EC received hysteroscopic surgery and conservative treatment whose paraffin-embedded tissue blocks preserved in our hospital between Jan. 2010 and Oct. 2022 was evaluated. Molecular subtyping based on TCGA classification identified low copy-number (CNL), microsatellite instability-high (MSI-H), and copy-number high (CNH) subtypes. IHC markers, including PTEN, PIK3CA, β-catenin, ARID1A, estrogen receptor (ER), and progesterone receptor (PR) were analyzed for their association with CR and recurrence. Transcriptome sequencing gene chips were used to study patients who achieved or did not achieve CR after three months, those who experienced recurrence within one year, and those who did not recur within two years. Differential genes were then mapped to KEGG pathways to explore the underlying mechanisms of progesterone therapy efficacy.
Results
Among the 68 patients classified through TCGA molecular typing, 65 cases (95.6%) were CNL subtype, two (2.9%) were MSI-H subtype, and one (1.5%) was CNH subtype. Following a three-month treatment, the CR rate for the CNL subtype was 75.4% (49/65), the MSI-H subtype was 50.0% (1/2), and the CNH subtype was 0% (0/1). In CNL subtype endometrial carcinoma, individuals with high PTEN and PR expression were more likely to achieve CR after three months (P < .05). Conversely, those with elevated CA199 levels and increased PIK3CA expression were more prone to recurrence after CR.
Conclusion
MSI-H and p53-mutant subtypes of endometrial carcinoma are not suitable for fertility preservation therapy. PTEN/PI3K-AKT-mTOR pathway activation contributes to reduced progesterone sensitivity, underscoring the need for targeted therapeutic strategies to improve patient outcomes.
Keywords
Introduction
Endometrial carcinoma represents the most prevalent gynecological malignancy, predominately affecting younger individuals. Approximately 12.7% of patients diagnosed with this cancer are under 45 years old. Fertility-sparing treatments are sought for patients with stage IA G1 to G2 endometrial carcinoma, particularly those under 45 years old and desiring childbirth. These treatments aim to reverse pathological changes in the endometrium, preserve the uterus, and preserve fertility. Evaluation of treatment efficacy involves regular endometrial biopsies during the treatment period, with hysteroscopic curettage conducted at three and six months. If a patient achieves CR after six months, the possibility of pregnancy can be considered.
However, challenges persist in fertility-sparing treatments for endometrial carcinoma. For instance, excessive hysteroscopic curettage and long-term progesterone treatment can lead to thinning of the endometrium, reduction in endometrial receptivity, and high rates of uterine cavity adhesions, potentially diminishing the success rate of pregnancy. Oral progesterone is the first-line treatment for early-stage endometrial cancer, because it can make the diseased endometrial undergo decidual-like changes without affecting the estrogen level in the body, and then transform into normal endometrial. ESGO/ESHRE/ESGE's recommended formulations for treatment of early EC are MA or medroxyprogesterone acetate (MPA) for 6-12 months, after which CR should be achieved, defined by two consecutive endometrial biopsies at least 3 months apart with no evidence of disease. 1 While domestic guidelines recommend waiting for CR at six months before considering pregnancy, 2 this results in extended medication and curettage periods. Some expert consensus and foreign guidelines propose the consideration of pregnancy after achieving CR at three months, wherein the damage to the endometrium caused by progesterone use and curettage will be reduced. Evidence suggests it is safe and reliable, with no difference in recurrence rate. Moreover, it also increases the likelihood of pregnancy. Therefore, three months of progesterone treatment can serve as a pivotal point for assessing the efficacy of conservative treatment. However, according to literature reports, the three-month treatment CR rate ranges from 60% to 90%, requiring a comprehensive exploration of influential factors. Currently, relevant research mainly analyzes the influencing factors of efficacy at six months and above. However, influencing factors of three-month CR may show variation. While the CR rate after six months of conservative treatment is significantly high (68% to 85%),3,4 recurrence post-CR remains substantial (30% to 40%) within a median period of approximately 15 months (4-66 months). 5 Previous studies propose factors such as obesity (body mass index (BMI) > 30 kg/m2), insulin resistance, polycystic ovary syndrome (PCOS), and post-CR progesterone maintenance therapy as potential contributors to recurrence,3–6 yet with inconclusive findings due to small sample sizes. Thus, further exploration is necessary to reduce the post-CR recurrence rate.
Exploration of the factors that affect the efficacy and prognosis of conservative treatment for endometrial carcinoma is limited, which could be attributed to small sample sizes in single institutions. Notably, previous research and clinical experience indicate that the clinical characteristics of patients with endometrial carcinoma might influence progesterone efficacy. Additionally, factors that affect the prognosis of endometrial carcinoma, such as molecular typing and immunohistochemical markers, such as PTEN, PIK3CA, CTNNB1, and ARID1A, are potential factors that may affect the efficacy of progesterone. 7 However, a lack of relevant research and conflicting results necessitate further in-depth exploration of these factors.This study aims to explore the influencing factors on the 3-month treatment efficacy and recurrence of endometrial carcinoma of fertility-sparing therapy.
Materials and Methods
Patient Collection
This study is a retrospective cohort study.130 patients with early-stage (FIGO stage I A) endometrial carcinoma treated conservatively with medication at our hospital from Jan. 2010 to Oct. 2022 were enrolled. Paraffin-embedded tissue blocks from the initial diagnosis retained at the hospital's pathology department were used for analysis. Patients were included if they met the following criteria: (1) age ≤ 45 years; (2) pathologically diagnosed with well-differentiated (G1) or moderately differentiated (G2) endometrioid carcinoma; (3) ultrasound or MRI indicating endometrial restriction without myometrial or cervical infiltration; (4) no suspicious metastatic lesions on imaging studies, with efficacy assessed through hysteroscopic curettage after three months of treatment. The reporting of this study conforms to STROBE guidelines. 8
Collection of Clinicopathological Information
A total of 130 patients were diagnosed, of which 68 had good paraffin section tissues for analysis. Clinical data from these 68 patients were collected, including age, BMI, menstruation, PCOS, diabetes status, obstetric history, endometrial thickness, carbohydrate antigen 125 (CA125), carbohydrate antigen 199 (CA199), and blood lipid level. Treatment mainly involved oral progesterone, such as megestrol acetate (MA), MPA, or intrauterine placement of LNG-IUD. Some patients also received subcutaneous injections of GnRH-a. CR was defined as the complete disappearance of cancer tissue, stromal decidual transformation, glandular atrophy, and a pathological examination confirming no abnormal proliferative changes in the endometrium.
Based on the TransPORTEC molecular typing method, TCGA molecular typing was performed on the 68 endometrial cancer tissues. The steps were as follows: (1) Sanger sequencing was used to detect mutations in POLE gene exons 9-14. If POLE mutations were observed, they were classified as POLE mutation subtypes; if not, next step was performed; (2) Immunohistochemical staining was used to detect mismatch repair (MMR) proteins MLH1, MSH2, MSH6, and PMS2. Patients with MMR protein deficiency underwent MSI testing. If they were MSI-H, they would be classified as MSI-H subtypes. If not, the next step was performed; (3) Immunohistochemical staining was used to detect p53 protein. If all tumor cells are negative or >70% of tumor cells are 3 + under the microscope, the TP53 gene was sequenced using next-generation sequencing technology. Mutations in the TP53 gene were classified as the HNL subtype. If p53 was scattered in 1+, it indicated the CNL subtype.
IHC Results
Immunohistochemistry (IHC) staining of PTEN, PIK3CA, β-Catenin, ARID1A, ER, and PR was performed on the CNL subtype. Five highly-magnified fields of view with tumor cells in each slide were selected randomly, with 500-1000 cells in each field. The scores were evaluated based on the ratio of positive cells in each field and the degree of staining. Positive cell count ratio scores were as follows: 0 point: ≤10%; 1 point: 11%-25%; 2 points: 26%-50%; 3 points: 51%-75%; 4 points: ≥75%. Staining intensity scores were as follows: 0 points: no staining; 1 point: the cell membrane, cytoplasm, and/or nucleus are light brown; 2 points: the cell membrane, cytoplasm, and/or nucleus are brown; 3 points: the cell membrane, cytoplasm, and/or nucleus are dark brown. IHC score adopts a semi-quantitative scoring method, where IHC score = positive cell count ratio score × staining intensity score, which is further graded based on the total score: negative (−): 0-1 points; weak positive (+): 2-4 points; positive (++): 5-8 points; strong positive (+++): 9-12 points. A score ≤4 points indicates low expression of IHC marker, while a score greater than 4 indicates high expression of IHC marker. 9 β-catenin protein is normally expressed on the membrane of endometrial glandular epithelial cells. When the CTNNB1 gene undergoes a missense mutation, β-catenin protein is expressed in the nucleus. We defined the expression of β-catenin in the cell membrane as low expression, and the expression of β-catenin in the nucleus as high expression.
The clinical characteristics and immunohistochemical markers of the 68 patients were analyzed to explore the factors influencing the achievement of 3-month CR and recurrence of conservative treatment for endometrial carcinoma.
MLH1 antibody, MSH2 antibody, MSH6 antibody, PMS2 antibody, p53 antibody, PTEN antibody, β catenin antibody, ER antibody, PR antibody were made in ZSGB-BIO. PIK3CA antibody was made in Bioss. ARID1A antibody was made in Abcam.
Statistical Analysis
Statistical analysis was conducted using SPSS 27.0 software. Measurement data were represented as mean ± standard deviation (x ± s) while counting data were presented as the number of cases and percentage. Univariate and multivariate logistic regression analyses were used for 3-month CR, and COX regression analyses were used for recurrence. Statistical significance was considered when P < .05.
Results
Clinical Characteristics & Prognosis of Patients
The clinical data of 68 patients are shown in Table 1. TCGA molecular typing was performed on 68 patients, revealing no pathogenic mutations in exons 9-14 of POLE, indicating the absence of POLE mutation subtypes. Among the patients, two individuals were classified as MSI-H subtype. Of these two patients, one, despite three months of treatment, did not achieve CR and subsequently underwent a hysterectomy. The other patient achieved CR after three months of treatment and remained recurrence-free during a 17-month follow-up. One patient was identified with a CNH subtype, and after three months of treatment without achieving CR, the patient chose to undergo a hysterectomy.
Clinical Characteristics of Included Cases.
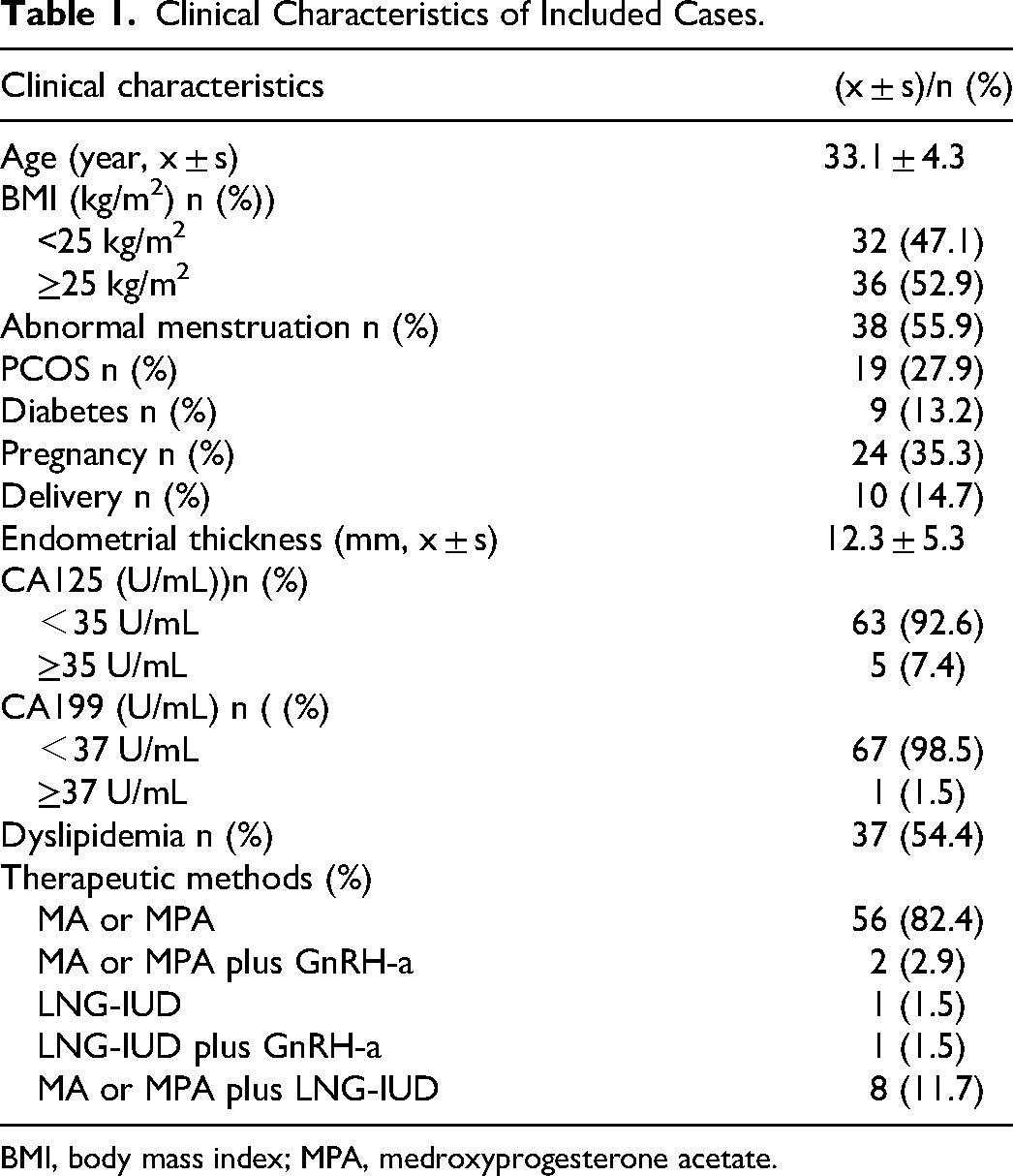
BMI, body mass index; MPA, medroxyprogesterone acetate.
Within the CNL subtype involving 65 patients, 49 patients achieved CR after three months, resulting in a three-month CR rate of 75.4% (49/65). Continued treatment up to six months revealed four cases without CR, raising the six-month CR rate to 93.8% (61/65). Among the 65 patients monitored for recurrence, 10 experienced recurrence over 3-42 months, with a median recurrence interval of 11 months, resulting in a recurrence rate of 15.6% (10/64).
Immunohistochemical Staining of the CNL Subtype Endometrial Carcinoma
The expressions of PTEN, PIK3CA, β-catenin, ARID1A, ER, and PR are shown in Figures 1-6. Among the 65 cases of CNL-subtype endometrial carcinoma, the expression of PTEN, PIK3CA, β-catenin, ARID1A, ER, and PR is shown in Table 2.

PTEN Expression (IHC Staining × 100).

PIK3CA Expression (IHC Staining × 100).

β-Catenin Expression (IHC Staining ×400).

ARID1A Expression (IHC Staining ×100).

ER Expression (IHC staining ×100).

The PR Expression (IHC Staining ×100).
The Expression of Immunohistochemical Markers in the CNL Subtype.

Analysis of Influencing Factors for 3-Month CR in CNL Subtype Endometrial Carcinoma
Age, BMI, PCOS, diabetes, endometrial thickness, CA125, CA199, blood lipids, PTEN, PIK3CA, CTNNB1, ARID1A, ER, and PR were considered as independent variables, and three-month CR was considered as dependent variable. Univariate logistic regression analysis between the independent and dependent variables revealed that those with high ER and PR expressions were more likely to achieve CR after 3 months of treatment compared to those with low expression, and the difference was statistically significant (P < .05), as shown in Table 3.
Univariate Logistic Regression Analysis of the Influencing Factors of 3-Month CR.

BMI, body mass index.
The independent variable with P value < .1 was included in the multivariate logistic regression analysis. The results indicated that patients with a high expression of PTEN, ER, and PR were more likely to achieve CR after 3 months of treatment, and the difference was statistically significant at P < .05 (Table 4).
Multivariate Logistic Regression Analysis of the Influencing Factors of 3-Month CR.

Analysis of Influencing Factors for Recurrence in CNL Subtype Endometrial Carcinoma
Age, BMI, PCOS, diabetes, endometrial thickness, CA125, CA199, blood lipids, three-month CR, pregnancy, PTEN, PIK3CA, CTNNB1, ARID1A, ER, and PR were considered as independent variables while recurrence was considered as a dependent variable. Univariate COX regression analysis of independent and dependent variables revealed that those with abnormally elevated levels of CA125 and CA199 were linked to a higher probability of recurrence. Additionally, those with a high expression of PIK3CA were more likely to recur after CR compared to those with low expression, and the difference was statistically significant (P < .05), as shown in Table 5.
Univariate COX Regression Analysis of the Influencing Factors of Recurrence.

BMI, body mass index.
The independent variable P value<.1 was included in the multivariate COX regression analysis to analyze CA125, CA199, and PIK3CA expression. The results revealed that patients with high PIK3CA expression had a higher probability of recurrence after achieving CR, while those with an abnormal elevation of CA199 before treatment were more likely to recur after reaching CR, with statistically significant differences (P < .05), as shown in Table 6.
Multivariate COX Regression Analysis of the Influencing Factors of Recurrence.

Preliminary Exploration of Transcriptomics Affecting the Efficacy of Progesterone Therapy
From the pool of patients who either reached or did not reach CR three months of treatment, a selection of paraffin blocks underwent gene transcriptome chip detection. Notably, six paraffin blocks were selected randomly from 16 patients without CR and six randomly selected blocks from 49 patients with CR. The heat map, scatter plot, and volcano map depicting the differentially expressed genes between the three-month CR and three-month non-CR groups are shown in Figure 7. To screen for differentially expressed genes, P value <.05 and Fold change >1.20 were selected as the criteria for defining significantly differentially expressed genes. The screened differentially expressed genes are presented in Table 7.

Differences in the Gene Expression Between Endometrial Carcinoma Tissues with and Without 3-Month CR.
Differential Genes Screened for 3-Month CR and 3-Month non-CR Groups.

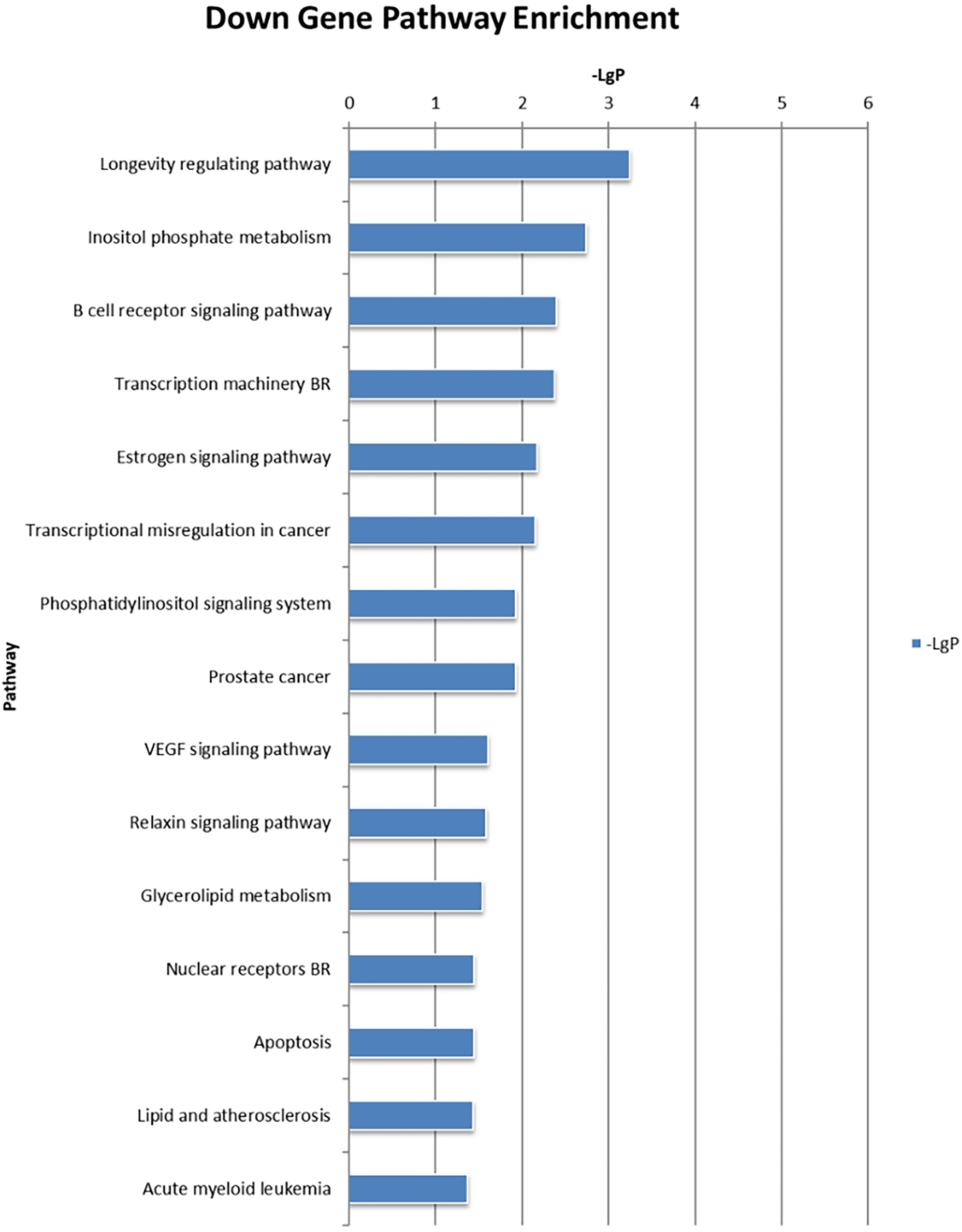
The differentially expressed genes between the three-month CR and non-CR groups were mapped into the KEGG pathways, wherein the adipocytokine signaling pathway, glucose metabolism, and focal adhesion, endocrine resistance were mainly upregulated, whereas cell apoptosis, colorectal cancer, and transcription machinery pathways were predominately downregulated (Figures 8 and 9).

Upregulation Pathway of Differential Gene Enrichment Between 3-Month CR and non-CR Groups.

The Downregulation Pathway of Differential Gene Enrichment Between the 3-Month CR and non-CR Groups.
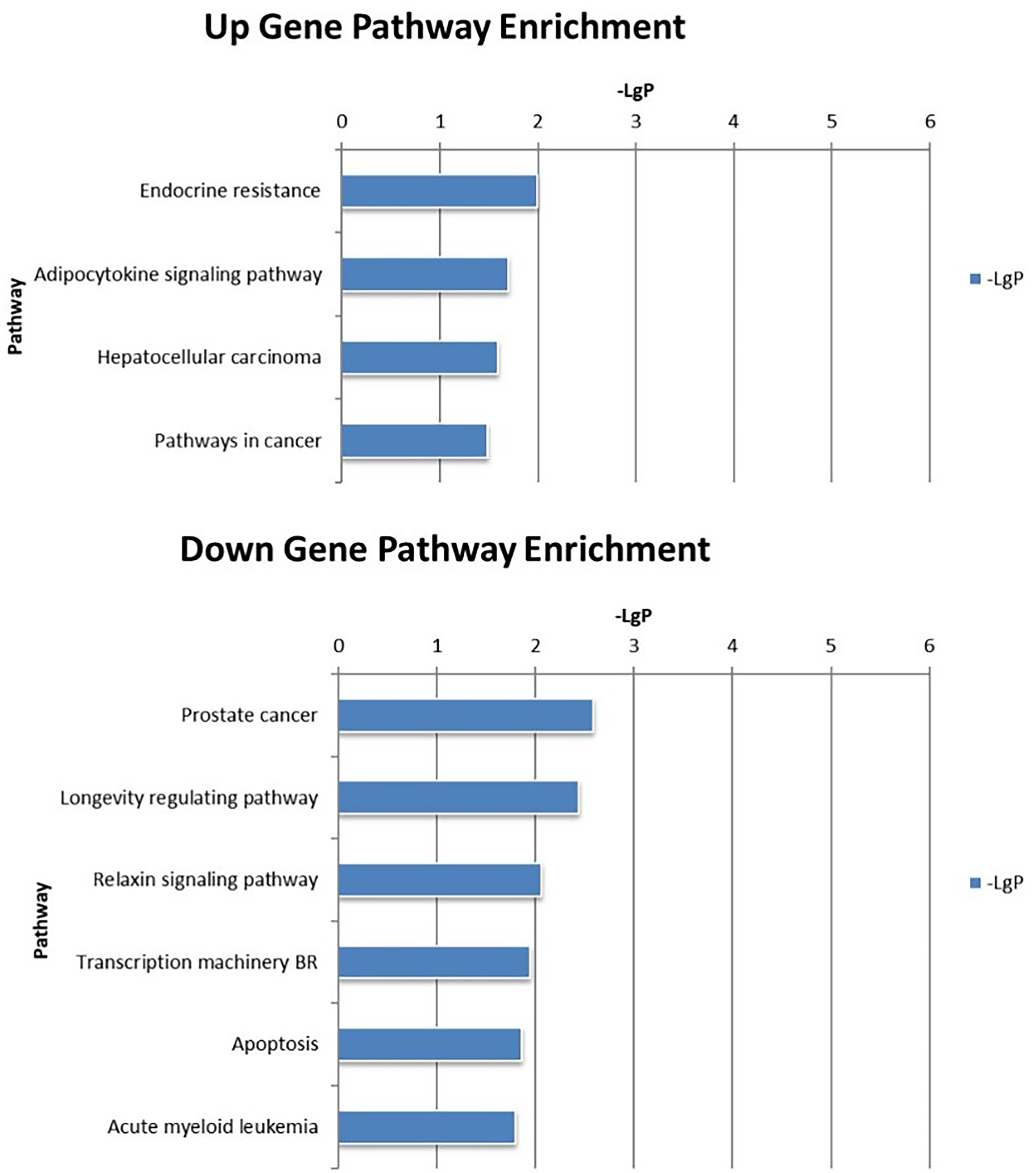
Among the 10 patients with recurrence within one year, six patients were selected randomly for gene transcriptome chip detection. A total of 22 cases did not recur for more than two years, six patients were selected randomly for gene transcriptome chip detection. The heat map, scatter plot, and volcano map depicting the differentially expressed genes between the recurrence and non-recurrence groups are presented in Figure 10. To screen for differentially expressed genes, P value <.05 and Fold change >1.20 were selected as the criteria for defining significantly differentially expressed genes. The screened differentially expressed genes are presented in Table 8. Meanwhile, differentially expressed genes between groups that recur within one year and those that have not recurred for more than two years were mapped into the KEGG pathway for enrichment analysis. Upregulated pathways were mainly related to endocrine resistance, colorectal cancer, and adipocytokine signaling pathway, whereas the downregulated pathways were mainly related to phosphoinositol metabolism, phosphatidylinositol signaling pathway, transcription disorders, and cell apoptosis (Figures 11 and 12).

Differences in the Gene Expression Between Endometrial Cancer Tissues that have Recurred Within 1 Year and Those that have not Recurred for >2 Years.

The Upregulation Pathway of Differential Gene Enrichments Between Recurrence and non-Recurrence Groups.
The Downregulation Pathway of Differential Gene Enrichment Between the Recurrence and non-Recurrence Groups.
Differential Genes Screened for the Recurrence and non-Recurrence Groups.

Intersecting the two sets of screened differentially expressed genes and identifying the upregulated and downregulated differentially expressed genes, as shown in Table 9.
Upregulation and Downregulation of the Differential Genes After the Intersection.

The upregulated and downregulated KEGG pathways of the above two groups were intersected, revealing the enrichment of the endocrine resistance and adipocytokine signaling pathways in these two groups. The downregulated pathway included the apoptosis pathway (Figure 13).
The KEGG Pathway After the Intersection Between the two Groups.
In the TNFα signaling pathway, mTOR inhibits tyrosine phosphorylation of the insulin receptor substrate (IRS1) by participating in serine phosphorylation, while AKT causes insulin resistance by influencing glucose uptake (Figure 14).While in the group with poor efficacy of progesterone treatment, ERα shows a downward trend. PI3K-AKT-mTOR is involved in this process (Figure 15).

Adipocytokine Signaling Pathway.

Endocrine Resistance Pathway.
Discussion
MRI should be used to evaluate the lesion involvement before hysteroscopic surgery. If there is no ovarian, cervical interstitial, and lymph node involvement, anti-mullerian hormone detection and antral follicle count should be performed to evaluate ovarian reserve function before fertility preservation in accordance with the above recommendations. In addition to the above examinations, blood clots should also be excluded by color ultrasound in both lower limbs. Endometrial carcinoma with fertility preservation was indicated as stage IA1 (endometrial infiltration) and histological grade was G1-G2. However, some studies have attempted to expand the evidence to include 2023 FIGO stages IA2 and IA3.After the disease reaches CR, pregnancy should be carried out as soon as possible. First of all, assisted reproductive technology is recommended to assist pregnancy. During the assisted pregnancy, LNG-IUS can be placed to locally secrete progesterone to protect the endometrial. If pregnancy is not successful after transplantation, oral short-acting contraceptive pills or intrauterine placement of LNG-IUS can be used to inhibit endometrial proliferation. Obstetric complications should be closely monitored during pregnancy, but it should be noted that endometrial cancer is not an indication of cesarean section. After the completion of fertility, if there is no family plan, you can choose to remove the uterus and decide whether to keep the ovaries according to the situation.
During conservative treatment with drugs, hysteroscopic curettage should be performed every 3 months to evaluate the endometrium, and if the disease does not reach CR after 9-12 months of continuous application, the uterus should be resected. If CR is reached, pregnancy should be prevented as soon as possible.Our research findings reveal a three-month CR rate of 75.4% and a six-month CR rate of 93.8%, surpassing reported CR rates following six months of conservative treatment, which typically ranges from 68.0% to 85.0%. 10 This suggests that it is safe for patients who wish to preserve their reproductive function to choose conservative drug therapy.
Currently, the recommended standard for the conservative treatment of endometrial carcinoma with drugs is that regardless of whether CR has been achieved by three months, medication needs to be administered until six months and pregnancy can be considered after achieving CR. Domestic guidelines suggest that achieving CR after three months for atypical endometrial hyperplasia can aid in pregnancy preparation, but patients with endometrial carcinoma need to achieve CR after six months for pregnancy preparation. Notably, prolonging the duration of medication may exacerbate endometrial glandular atrophy and stromal decidualization, and subsequent hysteroscopic curettage can cause trauma to the functional layer of the endometrium, increase endometrial adhesions, and thin the endometrium during ovulation, which is not conducive to fertilized egg implantation. The three-month CR rate in this study was 75.4% (49/65), and for this group of patients, it was proposed that medication could be stopped after three months of treatment to prepare for pregnancy. However, further exploration into the safety and recurrence rates post three months CR for these patients is necessary.
The rare occurrence of the POLE mutation subtype in endometrial carcinoma, absent in our study, aligns with its infrequency, accounting for approximately 7% to 12%. 11 The POLE mutation subtype of endometrial carcinoma has an advanced age of onset, with an average onset age of 55 years. Previous studies on the proportion of POLE mutation subtypes report an approximate rate of 5.1% to 6.9%, with a CR rate of approximately 66.7% (2/3) and a six-month CR rate of approximately 33.3% (1/3).12–14 However, due to the limited number of samples included, determining the efficacy of POLE mutation subtype endometrial cancer in preserving fertility proved challenging.
The MSI-H subtype accounts for approximately 19% of young endometrial carcinoma cases. Previous fertility-sparing studies of endometrial carcinoma have reported that the MSI-H subtype accounts for approximately 6.8% to 15.8%, with a CR rate of 46.2% (12/26), a six-month CR rate of 6.3% (1/16), and a recurrence rate of 42.9% (3/7).12–15 However, only two cases (2.8%) of MSI-H subtypes were detected in this study, with a three-month CR rate of 50.0% (1/2). Moreover, MSI-H subtype endometrial carcinoma is mostly diagnosed late in clinical practice, exhibiting strong invasion and metastasis ability. Without immunotherapy, the prognosis is poor. The current and previous studies suggest that the MSI-H subtype has a low CR rate and a high recurrence rate, and treatment that preserves reproductive function should be treated with caution. However, further research is needed to determine whether progesterone can be combined with other drugs to improve the efficacy of the MSI-H subtype.
The p53 mutant subtype, constituting 4% of young endometrial carcinoma cases, has shown modest efficacy in fertility preservation, accounting for 4.3% to 6.9% in previous fertility-sparing studies, a CR rate of approximately 55.6% (5/9), and a recurrence rate of 66.7% (2/3).12–14 The p53 mutant subtype is more common in type II and serous endometrial carcinoma. In this study, one case of p53 mutant with a medium-to-well differentiated endometrioid carcinoma was identified; however, the efficacy of fertility preservation was poor. After three months without achieving CR, the uterus was excised. Thus, the fertility-sparing treatment of the p53 mutant subtype demands careful evaluation. An analysis of the influencing factors of three-month CR was conducted on 65 patients using IHC. The results of the multivariate analysis suggest that individuals with high PTEN expression were more likely to achieve CR after three months of treatment than low expression, indicating that PTEN gene inactivation is an unfavorable factor, which is consistent with previous studies. Additionally, in the conservative treatment of endometrial carcinoma, PTEN gene inactivation may lead to a longer duration to achieve CR, and an increased progesterone dosage or the addition of related drugs can be administered at the initial stage of treatment to shorten the treatment duration and improve treatment efficacy. Notably, PTEN mutations or abnormal PTEN expressions have been associated with poor prognosis in endometrial carcinoma. Some studies demonstrated that the loss of PTEN expression is a predictive indicator for the progression of endometrial atypical hyperplasia to endometrial carcinoma. Meanwhile, the loss of PTEN expression in endometrial atypical hyperplasia also indicates the possibility of coexisting endometrial carcinoma. PTEN promoter methylation and functional loss are also related to the poor prognosis of endometrial carcinoma. Fyles et al 16 used PTEN+/- heterozygous mice to construct a PTEN-deficient endometrial carcinoma model. After ovariectomy or castration surgery, progesterone therapy was administered, which led to the conclusion that the occurrence of endometrial tumors in PTEN+/- mice and the activation of the PI3K pathway was not influenced by the disappearance of endogenous hormone or the use of progesterone therapy. The absence of PTEN leads to the activation of proteins such as PKB/AKT, FKHR, and mTOR, many of which are associated with components of malignant transformation, including proliferation, invasion, and anti-apoptosis. An absence of PTEN expression is common in the development of human endometrial carcinoma, which may make the lesion resistant to hormone treatment and lead to treatment failure. However, controversy remains over the relationship between PTEN gene inactivation and progesterone therapy efficacy. A meta-analysis by Travaglino et al 17 in 2018 suggests that PTEN deficiency indicates a better response to progesterone treatment (RR =0.89), with no statistically significant difference (P = .83). However, they did not study the efficacy of progesterone at three months of treatment. In another meta-analysis, Travaglino et al 18 reported that PTEN deficiency combined with low phosphorylated AKT expression had poor therapeutic effects on progesterone, but the difference was not statistically significant.
Univariate and multivariate analysis further suggests that PR expression is an independent risk factor affecting three-month CR. Patients with high PR expression are more likely to achieve CR after three months of treatment, as the combination of progesterone and PR causes endometrial glandular epithelial tumor cells to atrophy, induces stromal decidualization, and consequently leads to lesion regression. This result is consistent with the mechanism of progesterone's effect on the human body. In this study, the three-month CR rate of PR low-expression individuals was 57.9%, while that of PR negative-expression individuals was 44.4%; The CR rate of PR high expression individuals was 82.6%, which is significantly higher than that of negative and low expression individuals. Notably, for some PR negative and weakly positive patients, the use of high-efficiency progesterone therapy can still be effective, albeit low, which is worth paying attention to in a clinical setting.
This study could not identify a relationship between BMI, PCOS history, diabetes status, and three-month CR, but previous studies demonstrated that the higher the BMI and presence of PCOS history, the lower the remission rate after treatment.19–22 Moreover, this mechanism could also be associated with PCOS and insulin resistance in obese individuals, wherein an increase in serum androgens can be converted into estrogen, leading to an increase in serum estrogen concentration and antagonizing the effect of exogenous progesterone in the endometrium, resulting in progesterone resistance. 23 However, some studies suggest that there is no significant correlation between BMI and CR.24,25 The correlation between obesity, PCOS, and diabetes and the three-month efficacy still needs further study using a larger sample size.
Univariate and multivariate analyses suggest that patients with abnormally high pre-treatment CA199 levels are more likely to undergo recurrence after achieving CR. The high recurrence rate could be related to the abundance of endometrial tumor tissue, high gland density, abundant tumor cells, and active proliferation. This suggests that for those with endometrial thickness exceeding 1 cm before treatment and those with an abnormal elevation of CA199, the medication duration should be appropriately extended. Similarly, for women who have failed to conceive or have completed childbirth, long-term oral contraceptives should be taken to delay disease recurrence.
Additionally, high PIK3CA expression was linked to recurrence, with a recurrence rate of 26.1% (6/23) in high PIK3CA-expressing individuals and 9.8% (4/41) in low-expressing individuals. Abnormal changes in the PI3K-AKT-mTOR pathway are a common pathogenesis of endometrial carcinoma, which is regulated by class I PI3K kinases. PIK3CA encodes the PI3K catalytic subunit p110 α (tumor suppressive catalytic subunit), which is normally inhibited by the tyrosine kinase receptor (RTK), and when activated, p110 α phosphorylates PIP2 on cells and generates PIP3, which can bind to and phosphorylate AKT, thereby triggering tumorigenesis. The high expression of PIK3CA indicates its abnormal activation state, which can be due to mutations in its inhibitory factor PTEN gene or mutations in the coding gene PIK3CA. This study used phosphorylated PIK3CA antibody to perform IHC on endometrial carcinoma sections. COX regression demonstrated that individuals with high PIK3CA expression were more likely to recur, with statistically significant differences. This suggests that individuals with abnormal PIK3CA activation before treatment are more likely to undergo recurrence post-CR, which is consistent with the prognostic factors of endometrial carcinoma. In our study, 23 patients displayed a high expression of PIK3CA, which suggests that such patients should be carefully monitored for recurrence after CR and ensured of the effective measures to prevent recurrence. Notably, the conservative treatment effect of progesterone can be improved by regulating the expression of related genes in the PTEN/PI3K-AKT-mTOR pathway.
Previous studies hypothesize a positive correlation between obesity and disease recurrence,18,26 and the mechanism may be related to overweightness, which leads to endometrial hyperplasia through excessive estrogen secretion and high insulin. 23 However, other studies suggest that BMI is not correlated with disease recurrence.23–25 Studies have also shown that insulin resistance and PCOS history do not influence disease recurrence.23,27 Nevertheless, BMI, PCOS history, and diabetes status were not found to be associated with disease recurrence in this study. Apart from the clinical factors mentioned above, no correlation between three-month CR and recurrence was observed, which could be attributed to the continued medication consolidation treatment post-three-month CR. Furthermore, disease recurrence is a complex process wherein clinical factors cannot explain the mechanism of recurrence to the full extent, warranting the combined analysis of molecular typing and IHC.
Transcriptomic analysis revealed differentially expressed genes linked to various pathways that were upregulated, such as steroid hormone synthesis and metabolism, lipid droplet synthesis, and cholesterol synthesis, along with diseases such as colorectal cancer, gastric cancer, esophageal cancer, pleural mesothelioma, intracranial aneurysm, osteogenic imperfecta, congenital myasthenia syndrome, and Alzheimer's disease. The downregulated genes were mainly related to DNA double-stranded damage repair, RNA transcription, and cell cycle. Enriching the differentially expressed genes from the above two groups into the KEGG pathway revealed two upregulated and downregulated KEGG pathways. After intersecting the pathways of these groups, the upregulated pathways were identified as endocrine resistance, adipocytokine signaling pathway, liver cancer pathway, and malignant tumor pathway, while the downregulated pathways included cell apoptosis pathway and transcription pathway. The PI3K-AKT-mTOR signaling pathway is also associated with lipid metabolism and endocrine resistance pathways, indicating that the PI3K-AKT-mTOR pathway is associated with progesterone efficacy and recurrence. Liu et al proposed that long-term progesterone therapy may lead to progesterone resistance through the activation of the PI3K/AKT/mTOR signaling pathway. 28 The activation of PI3K/AKT/mTOR leads to reduced sensitivity to progesterone therapy by promoting tumor cell proliferation and inhibiting tumor cell autophagy. 29
Limitations
However, there are some limitations to our study. The total sample size included in the statistical analysis was limited, only 65 cases, and the statistical efficacy was limited. In addition, patients with the MSI-H subtype of endometrial cancer refused to undergo germline gene mutation testing for personal reasons, so it is not possible to determine whether they are patients with Lynch syndrome. The number of cases included in this study was limited. In the future, a larger sample size will be needed to further validate the reliability of our findings.In addition, further exploration of genes and pathways related to the efficacy of conservative treatment for endometrial cancer based on transcriptomics sequencing results will be needed in the future. This includes studying corresponding targeted drugs and the combination of progesterone to enhance therapeutic effects.
Conclusion
In conclusion, molecular typing serves as a valuable tool in determining patient populations suitable for fertility-preserving therapy for endometrial carcinoma. Conservative treatment for certain subtypes, such as MSI-H subtype and CNH subtype, exhibits poor prognosis, necessitating careful consideration before commencing treatment. Further research is needed to expand the sample size for analyzing the treatment efficacy of patients with the POLE mutation subtype. In patients with the CNH subtype, those with high PTEN and PR expressions are more likely to achieve CR after three months of treatment, while those with abnormal CA199 elevation and high PIK3CA expression are more likely to recur after CR. Therefore, the activation of the PTEN/PI3K-AKT-mTOR pathway is associated with reduced sensitivity to progesterone therapy.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and approved by the Ethics Committee of Peking University Third Hospital with the approval ID No. 2021-193-02 (7 September 2021). The submitted study is a sub-project under this approved protocol. Due to the retrospective nature of the study, participant informed consent was waived, and the study design was approved by the appropriate ethics review board.
Footnotes
Abbreviation
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013) and approved by the Ethics Committee of Peking University Third Hospital (No. 2021-193-02). The submitted study is a sub-project under this approved protocol. Due to the retrospective nature of the study, participant informed consent was waived, and the study design was approved by the appropriate ethics review board.
Authors’ Contributions
Y L and HY G conceived the project, Y L and YF N performed data collection. Y L and YF N performed data analysis. Y L wrote the manuscript and all other authors edited the manuscript.
Data Availability Statement
The datasets used and/or analysed during the current study available from the corresponding author (Hongyan Guo,Department of Obstetrics and Gynecology, Peking University Third Hospital, Huayuan Street, Haidian District, Beijing,100191, China, Email: bysyghy@163.com)
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.