
Abstract
Objective
This study analyzed the dosimetric impact of residual errors (rotational and deformation errors) in left-sided breast cancer radiotherapy after cone-beam CT (CBCT)-based translational errors correction.
Methods
Twenty patients treated with intensity-modulated radiotherapy (IMRT) were retrospectively analyzed. Virtual CT images were generated by deforming and registering CBCT images with planning CT images. The accumulated dose was calculated to assess residual errors effects on target and organs at risk (OARs). A phantom test was conducted to evaluate rotational errors impacts.
Results
Results showed significant dose differences: for 4005 cGy, D98 and D95 of the breast (PTVb) decreased, and mean dose, V30, and V20 of the left lung reduced; for 5000 cGy, D98 of the supraclavicular lymph nodes (PTVsc) and PTVb, D95 of PTVb, and mean dose and V20 of the heart differed significantly. Phantom simulations revealed that pitch angles ≤−1.8° and roll/yaw angles >2° caused overdosing in the left lung and heart, with maximum dose differences of 31.89% (heart) and 19.19% (lung) for 4005 cGy, and 26.32% (heart) and 20.92% (PTVsc) for 5000 cGy.
Conclusion
Residual errors significantly affect dose distribution despite CBCT-based translational correction. Improved immobilization techniques or 6DOF couch correction are recommended to mitigate rotational errors.
Introduction
Breast cancer is one of the most common malignancies among women globally. 1 Radiotherapy has been proven effective for early-stage breast cancer.2-4 During breast cancer radiotherapy, setup errors, respiratory motions, and relative target displacement can lead to underdosing of the target and overdose of the OARs. 5 The setup errors in breast cancer radiotherapy patients consist of translational, rotational, and deformation errors. 6 CBCT has been employed to reduce the translational errors.7-10 A six-degree-of-freedom (6DOF) couch has been utilized to correct rotational errors.11-14 Many studies15-17 have applied surface-guided radiotherapy (SGRT) to monitor deformation variations in patients, yet failed to quantify the dosimetric effects of these variations.
Currently, most hospitals use a conventional four-degree-of-freedom (4DOF) couch, which can only correct translational errors. As a result, it is difficult to comprehend the impact of residual errors (including rotational errors and deformation errors) following the correction of translational errors. Few studies have analyzed the residual errors. Among them, only Gang Cai et al 18 investigateed the residual and intrafractional errors. They found that a long treatment time and couch rotation may affect the accuracy of treatment delivery.
However, deformable image registration (DIR) techniques are commonly used to align CBCT images with planning CT images and map the dose, obtaining a more accurate accumulated dose.19,20 This helps evaluate the dose differences caused by the deformation of the target and OARs throughout the entire radiotherapy process. Rajko Topolnjak et al 21 quantified the differences in heart dose for left-sided breast cancer patients during different respiratory phases using four – dimensional (4D) CBCT and calculated the accumulated dose.
Therefore, In this study, we utilized CBCT images and employed a hybrid grayscale and structure-based DIR to calculate the accumulated dose to the target and OARs. Our aim was to analyze the dosimetric differences caused by residual errors after translational errors were corrected. Additionally, CBCT images were acquired using a female phantom to simulate rotational errors for dosimetric analysis. The goal was to study the impact of rotational errors among residual errors and provide a reference for clinical image – guidance and correction strategies.
Materials and Methods
Patient Informations
A retrospective analysis was performed on 20 patients with Stage T1N0M0 or Stage T2N1M0 left – sided breast – conserving cancer. These patients were collected randomly and were treated with a Synergy accelerator (Elekta, Stockholm, Sweden) in our hospital from October 2023 to August 2024. Among these 20 patients, 10 patients received whole – breast irradiation with a prescription dose of 4005 cGy delivered in 267 cGy per fraction. The remaining 10 patients received irradiation for the whole breast and supraclavicular lymph nodes, with a prescription dose of 5000 cGy delivered in 200 cGy per fraction. This study was approved by the Ethics Committee of West China School of Medicine, Sichuan University (approval number: No.2025227).
All patients were immobilized in the supine position on a 15° wedge plate using a breast vacuum bag (Klarity Medical, Shenzhen, China). Then, they were simulated in free – breathing with a GE Revolution CT (GE Medical Systems, Milwaukee, WI). The CT scan ranged from the chin to the lower edge of the liver with a slice thickness of 3 mm. The scanned images were transferred to the treatment planning system (TPS) (version4.7.5; RaySearch Laboratories AB, Stockholm, Sweden) for contouring and treatment planning. Clinical target volume (CTV) was delineated on the images by radiation oncologists in accordance with the ESTRO guideline. 22 The planning target volume (PTV) was generated by adding a 5-mm margin to CTV.
Treatment Planning
All plans were generated by experienced medical physicists and approved by oncologists before treatment. 6 MV photon beams were used. Dose calculation was performed with a collapsed cone algorithm. Six – field irradiations were employed with a prescription dose of 5000 cGy, with angles of 312°, 325°, 340°, 119°, 132°, and 160°. Four – field irradiations were used with a prescription dose of 4005 cGy, with angles of 296°, 310°, 110°, and 125°. All plans utilised a flash margin, was achieved by extending the fields into the air by 2 cm.23,24
Planning Based on Virtual CT
Daily CBCT images, which were acquired by the Elekta X – ray Volumetric Image (XVI) system for each patient and corrected only for translational errors, were transferred to Raysearch (RaySearch Laboratories, Stockholm, Sweden). The DIR process follows the method described by Rafael García-Molla et al. 25 First, a rigid registration was performed between the planning CT images and CBCT images. Second, the DIR was carried out, enabling the mapping of the target and OARs in the two registered images to generate virtual CT images. Finally, the same beam geometry (including gantry angle, collimator angle, etc) from the original plan was mapped onto the virtual CT images to create a new plan.
Calculation of the Accumulated Dose
In this study, the Raysearch employed a hybrid gray-scale and structure-based deformable image registration to deform the dose distribution. The planning CT images were defined as the floating images, and the virtual CT images were defined as the reference images. Subsequently, the deformed dose from each treatment fraction were superimposed to calculate the accumulated dose that the patient received at each anatomical position throughout the entire treatment process.
Phantom Scanning
To demonstrate the effect of rotational errors among residual errors, we employed a female phantom (Model: Chengdu Bionic Phantom) to artificially introduce rotation to simulate the rotation scenarios that could occur during patients’ clinical treatment. As shown in Figure 1, the female phantom was immobilized and simulated in the same way as that used for clinical patients. The target was contoured, and two treatment plans were designed with prescribed doses of 4005 cGy and 5000 cGy. CBCT was carried out on the phantom using the XVI system. Seventy CBCT images were acquired, which were used to generate the virtual CT imags. Subsequently, the plan was calculated based on those virtual CT images.
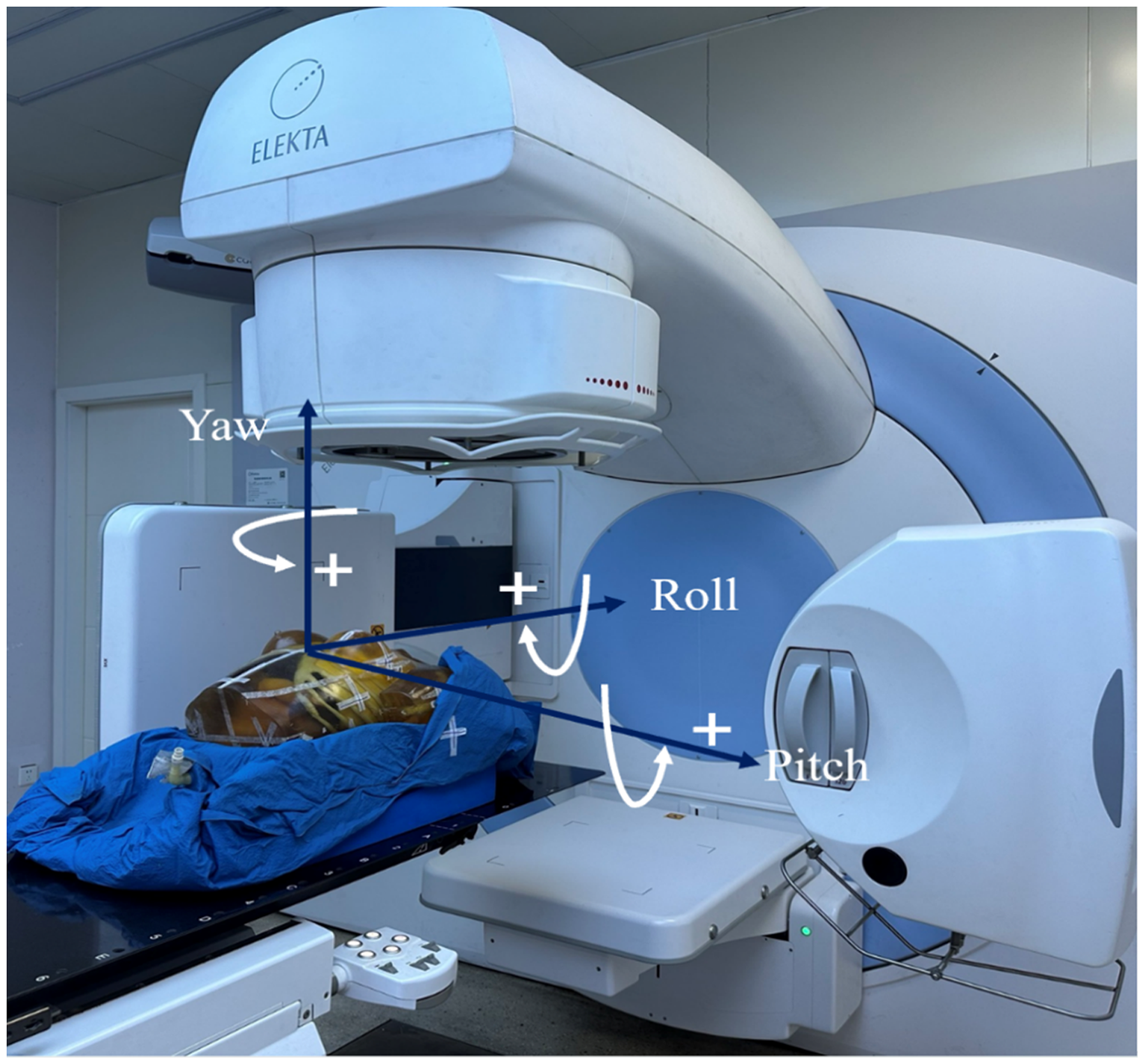
The Phantom Placed on the Couch of the Radiotherapy System was Marked with Rotational Axes.
Statistical Analysis
A paired sample test was conducted via SPSS 27 statistical software. All data were presented as the mean ± standard deviation (minimum-maximum), with a P-value of <.05 considered statistically significant.
Results
Clinical Dosimetric Evaluation
Dosimetric Evaluation in the Prescription of 4005 cGy
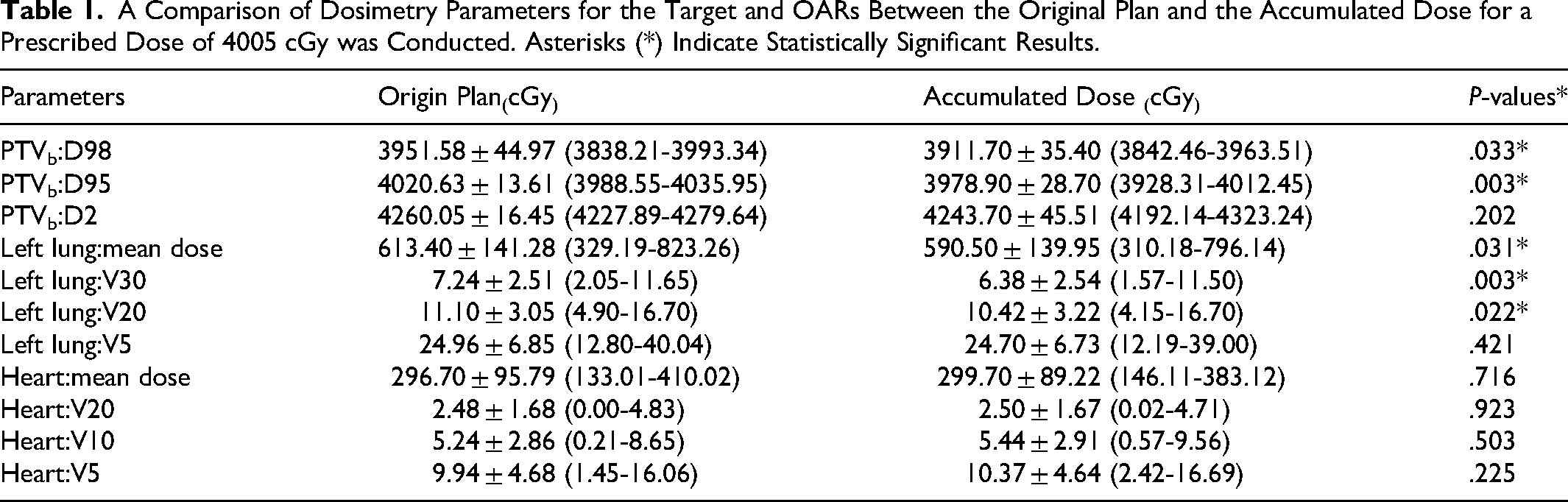
Table 1 presented a comparison of the dose to the target and OARs between the original plan and the accumulated dose for a prescribed dose of 4005 cGy. The D95 and D98 of PTVb, the mean dose, V30, and V20 of the left lung showed significant differences. In contrast, the D2 of PTVb, the V5 of the left lung, and the mean dose, V20, V10, and V5 of the heart did not show significant differences.
A Comparison of Dosimetry Parameters for the Target and OARs Between the Original Plan and the Accumulated Dose for a Prescribed Dose of 4005 cGy was Conducted. Asterisks (*) Indicate Statistically Significant Results.
Dosimetric Evaluation in the Prescription of 5000 cGy
Table 2 illustrated that there were statistically significant differences in the D98 of PTVsc and PTVb, and the D95 of PTVb, as well as the mean dose and V20 of the heart for patients with a prescribed dose of 5000 cGy. In contrast, there were no statistically significant differences in the D95 and D2 of PTVsc, the D2 of PTVb, the mean dose, V30, V20, and V5 of the left lung, and the V10 and V5 of the heart.
A Comparison of Dosimetry Parameters for the Target and OARs Between the Original Plan and the Accumulated Dose for a Prescribed Dose of 5000 cGy was Conducted. Asterisks (*) Indicate Statistically Significant Results.
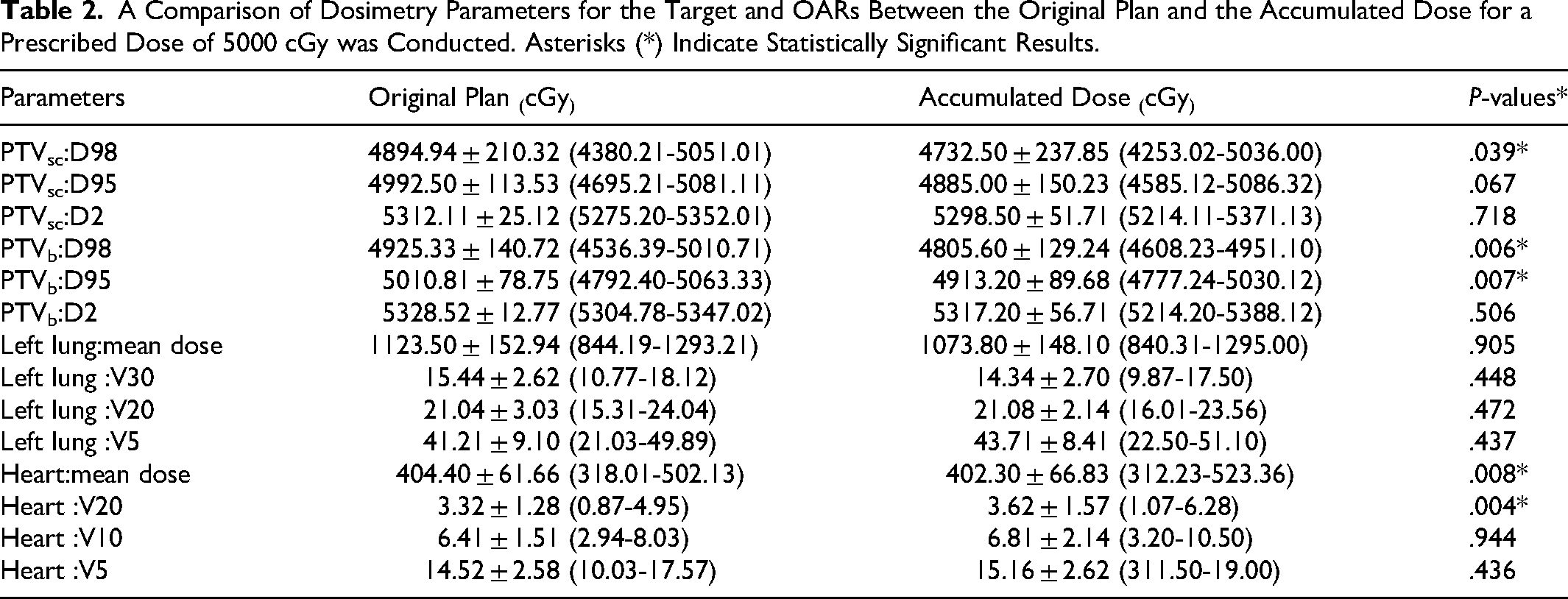
Figure 2 showed the dose distribution and dose – volume histogram (DVH) for a prescription dose of 4005 cGy (patient No. 4 in this cohort) and 5000 cGy (patient No. 9 in this cohort) between the original plan and the accumulated dose.

Dose Distribution and DVH of the Prescription Dose of 4005 cGy (Above) and 5000 cGy (Below).
Phantom Analysis
Rotational Distribution
Figure 3 showed the differences on mean dose to heart and lung, D95 of PTVsc and PTVb between the prescribed dose of 4005 cGy and 5000 cGy under the effects of pitch, roll, and yaw rotations. The color intensity represented the degree of influence of rotational errors, where redder colors denoted a greater magnitude of difference. The dose to the heart was influenced when the pitch angle was negative, the roll angle was positive, and the yaw angle was positive, as shown by the red areas in the Figure 3. In contrast, for the prescription dose of 5000 cGy, PTVsc demonstrated insufficient coverage when the pitch angle was negative and the yaw angle was positive, as depicted by the blue areas in the Figure 3. However, the PTVb was much less affected at both the prescription dose of 4005 cGy and 5000 cGy. Furthermore, the results suggested that pitch and yaw were the primary contributors to dose deviation.
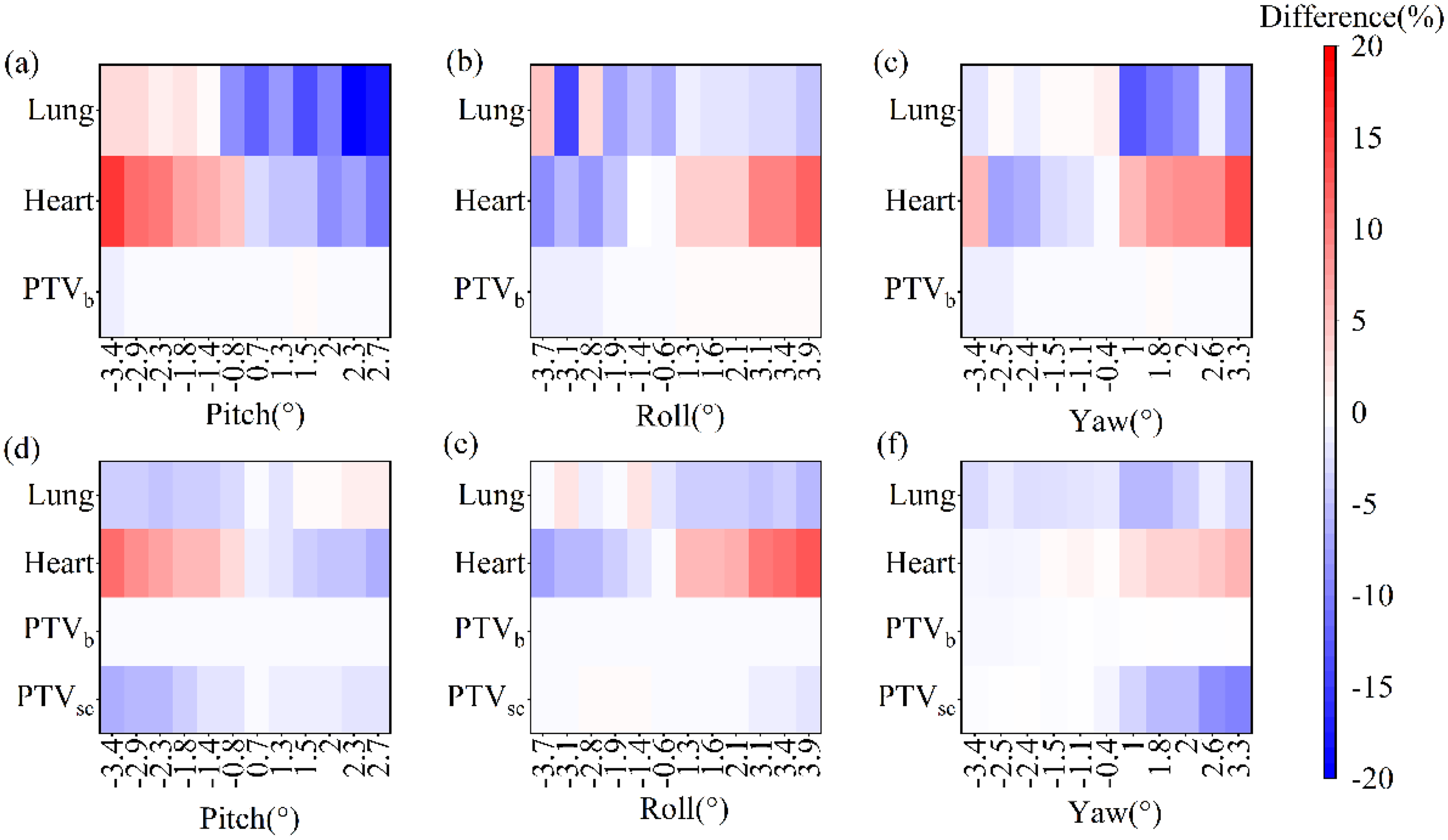
Rotational Distributions of the 4005 cGy Prescribed Dose (Above) and 5000 cGy Prescribed Dose (Below).
Differences Caused by Rotational Errors
Figure 4a and b illustrated the differences in target and OARs between the original plan and the plan calculated in the phantom for prescription dose of 4005 cGy and 5000 cGy, respectively. The more impact of rotational errors on the prescribed dose of 4005 cGy was observed mainly in the heart and lung, with maximum differences of 31.89% and 19.19%, respectively. For the prescribed dose of 5000 cGy, the more pronounced impacts were mainly observed in the heart and PTVsc, with maximum differences of 26.32% and 20.92%, respectively.

The Differences in Target and OARs Between the Original Plan and Plan Calculated in the Phantom for the Prescription Dose of 4005 cGy (Left) and 5000 cGy (Right).
Discussion
Although several studies18,26 have analyzed the dose deviation due to residual errors and deformation, they employed the different image matching methods. In this study, we first analyzed the impact of residual errors on the total delivered dose throughout the entire treatment processs in DIR. We found that the presence of residual errors might contribute to the total dose deviation. Additionally, we used a female phantom to artificially introduce rotations to simulate the rotation scenarios that could occur during patients’ clinical treatment. We found that the rotational errors could cause the discrepancies in target and OARs, especially when the pitch angle was negative, the roll angle was positive, and the yaw angle was positive.
Several studies have investigated dose calculations based on image-guided CBCT images using various methods, including dose calibration on CBCT images,27,28 deformable registration of planning CT with daily acquired CBCT,29,30 and deep learning. 31 In this study, we emplyed the method proposed by R.S. Thing et al 32 to generate virtual CT images after deforming the planning CT image with CBCT images. We then mapped the target and OARs from the original plan to these virtual CT images for dose calculation, ultimately obtaining the accumulated dose. Our findings indicated that for left-sided breast-conserving patients, there was no significant difference between original plan and accumulated dose, except for D95 of PTVb, which showed a statistically significant difference. The accumulated dose was 41.73 cGy and 97.61 cGy lower than the dose of the original plan, respectively. This is because, although image guidance can eliminate translation errors throughout the entire treatment process, it remains susceptible to rotational errors and target deformation. 33 At the same time, we found that the dose to the lung and heart was lower than those in the original plan, probably because rotational errors led to a smaller irradiated volume of the lung and heart. However, the direction of rotational error is not the focus of this study for clinical patients. Instead, it was investigated in the phantom study.
This study investigated the impact of residual errors on the final accumulated dose using daily CBCT images. We found that although CBCT was used to correct translational errors, residual errors can still affect the total delivered dose to the target and OARs. Anand Swaminath et al 20 demonstrated that the accumulated dose in stereotactic radiotherapy for liver cancer more accurately predict the time to local tumor progression. Sadegh Alam et al 34 used weekly magnetic resonance images to calculate the accumulated dose to the esophagus, which was statistically significant compared with the original plan. In contrast, Vickie C Kong et al 35 calculated the accumulated dose to the rectum by comparing bone matching and prostate alignment, suggesting a greater difference on the basis of bone matching. In conclusion, the utilization of daily CBCT images to assess the accumulated dose to the target and OARs can aid in predicting local tumor progression and the dose delivered to patients at different stages of radiotherapy. This enables physicians to adjust treatment plans and develop adaptive radiotherapy.
To demonstrate the effect of rotational errors among residual errors, this study utilized XVI system to acquire CBCT images of a female phantom. As illustrated in Figure 3, dose bias are more prone to occur when the pitch angle is negative and both roll angle and yaw angle are positive, This finding is consistent with the results reported by Min Fu et al. 36 They simulated the pitch, roll, and yaw rotations by adjusting the angles of the breast brackets, gantry, and couch. They reported that when the pitch was −2.5° and both roll and yaw were 3°, the V50 of the PTV decreased by 20.07% compared with the original value, whereas the V5 of the heart and mean heart dose increased by 7.49% and 165.76 cGy, respectively. In this study, after introducing rotational errors, the effects on the prescribed dose of 4005 cGy was mainly observed in the heart and the left lung, with maximum differences of 31.89% and 19.19%, respectively. For the prescribed dose of 5000 cGy, more pronounced effects were mainly observed in the heart and the supraclavicular lymph nodes, with maximum differences of 26.32% and 20.92%, respectively. The increase in the dose to the heart is attributed to rotational errors with a negative pitch angle, a positive roll angle, and a positive yaw angle. These rotational errors lead to a greater portion of the heart being included in the target. 37 The smaller effect on PTVb is attributed to the approximately oval shape of the breast. Previous studies37,38 have indicated that rotational errors have a limited effect on target with a circular shape. In a study conducted by Tsujii K et al 39 on cervical cancer, rotational errors in the pitch direction were moderately correlated with CTV coverage and highly correlated with OARs, such as the bladder and rectum. In this study, the differences between the prescription dose of 4005 cGy and 5000 cGy are the magnitude of the prescribed dose and the shape of the target. The target shape for the 5000 cGy prescribed dose is more complex, which makes a difference in the results. Previous studies40,41 have reported the impact of rotational errors in multiple brain metastatases. They found that smaller target sizes may still exhibitincreased sensitivity to rotational errors. Georgia Prentou et al 42 found that rotational errors was not significant on dosimetric prostate coverage due to the almost spherical shape of the prostate,but it did the seminal vesicles coverage. Annele Heikkilä et al 6 compared the VMAT and tangential field-in-field (FiF) in left-sided breast cancer, found that the dose distribution of the heart and left anterior descending artery was more stable with respect to rotations in VMAT plans compared with FiF plans.
Although R.S. Thing et al 32 concluded that dose calculations based on virtual CT images generated after deformable image registration can be utilized for clinical assessment, these calculations are still influenced by the quality of the CBCT images 43 as well as the accuracy of the deformable registration process. This highlights one of the shortcomings of this study: the poor image quality of CBCT images. Another limitation of this study is that the phantom is rigid and fails to effectively simulate the actual deformations of the patient's body surface, such as contraction or swelling. Consequently, this paper focuses only on the effect of rotational errors among residual errors on the dosimetry of the target area and OARs in phantom study. In future studies, we will systematically quantify the dose differences caused by deformation errors.
Conclusion
Despite the use of CBCT to correct translational errors, residual errors can still affect the total delivered dose to the target and OARs. Preventing large magnitude residual errors is of crucial importance. The simulated rotation study showed that when the pitch angle is ≤−1.8° and both the roll angle and yaw angle exceed 2°, a greater dose impact occurs on the heart and supraclavicular lymph nodes. Therefore, it is recommended to improve the immobilization technique to reduce rotational errors or to use a 6DOF couch for correction.
Footnotes
Abbreviations
Acknowledgments
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ya Wang, Denghong Liu and Renming Zhong. The first draft of the manuscript was written by Ya Wang and all authors commented on previous versions of the manuscript. Renming Zhong read and approved the final manuscript.
Ethical Consideratiions
This study was approved by the Ethics Committee of West China School of Medicine, Sichuan University (No.2025227).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funds from Science and Technology Department of Sichuan Province of China (grant no.2024YFFK0147).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.