
Abstract
Pancreatic cancer has the highest mortality rate of all major cancers, with a 5-year survival rate of about 10%. Early warning signs and symptoms of pancreatic cancer are vague or nonexistent, and most patients are diagnosed in Stage IV, when surgery is not an option for about 80%–85% of patients. For patients with inoperable pancreatic cancer, current conventional treatment modalities such as chemotherapy and radiotherapy (RT) have suboptimal efficacy. Tumor progression is closely associated with the tumor microenvironment, which includes peripheral blood vessels, bone marrow-derived inflammatory cells, fibroblasts, immune cells, signaling molecules, and extracellular matrix. Tumor cells affect the microenvironment by releasing extracellular signaling molecules, inducing peripheral immune tolerance, and promoting tumor angiogenesis. In turn, the immune cells of the tumor affect the survival and proliferation of cancer cells. Myeloid-derived suppressor cells are key cellular components in the tumor microenvironment and exert immunosuppressive functions by producing cytokines, recognizing other immune cells, and promoting tumor growth and metastasis. Myeloid-derived suppressor cells are the main regulator of the tumor immune response and a key target for tumor treatments. Since the combination of RT and immunotherapy is the main strategy for the treatment of pancreatic cancer, it is very important to understand the immune mechanisms which lead to MDSCs generation and the failure of current therapies in order to develop new target-based therapies. This review summarizes the research advances on the role of Myeloid-derived suppressor cells in the progression of pancreatic cancer and its treatment application in recent years.
Keywords
Introduction
Pancreatic cancer is currently the fourth leading cause of cancer-related death in the world, 1 though its incidence rate and mortality rate are increasing. It is predicted that by 2030, pancreatic cancer will be the second most common of all cancers. 2 Pancreatic cancer is one of the most lethal malignancies with extremely poor prognosis and few successful treatment schemes. 3 The 5-year overall survival (OS) rate of pancreatic cancer patients is abysmal at less than 5%. 4 Surgical resection is the only curable method for localized pancreatic cancer, but because of the lack of early symptoms and aggressive property of pancreatic cancer, fewer than 20% of tumors can be removed at the time of diagnosis.5,6 Most patients relapse after operation, even though conventional adjuvant therapy is systematically applied. 7 Neoadjuvant therapy improves the operative rate, but even in patients with local and resectable tumors, the 5-year OS rate is only about 27%. 8
Myeloid-derived suppressor cells (MDSCs) comprise a heterogeneous population of bone marrow cells having an immunosuppressive phenotype and serving as a key component of the immunosuppressive niche in cancer. The presence of MDSCs in cancer patients is associated with poor survival and tumor recurrence. MDSCs can significantly inhibit the T cell response and regulate the fate of multiple cells in the innate immune system. MDSCs-mediated immunosuppression is mainly due to the up regulation of inducible nitric oxide synthase (iNOS) and arginase 1 (Arg1), and the release of reactive oxygen species (ROS). Recently, a variety of inhibitory mechanisms of MDSCs have been identified, including antigen presentation to Tregs and secretion of cytokines such as IL-10 and TGF-β. 9 In fact, MDSCs play a central role in controlling and maintaining an inhibitory tumor microenvironment (TME) in solid tumors. 10 Increasing evidence supports that the number of circulating and intratumor MDSCs is related to cancer stage, progression, and resistance to chemotherapy and radiotherapy (RT). 11 Therefore, understanding the biological characteristics of MDSCs is an essential step to improve antitumor immunity. Here, we will review the important biological aspects of MDSCs, including their characteristics, development, activation, expansion, and inhibitory mechanisms that support cancer growth and progression. In addition, we will highlight important attempts to target or manipulate MDSCs biology to obtain treatment efficacy. Finally, we will discuss the latest trends and future directions of the studies on MDSCs to target pancreatic cancer.
Epidemiology and Current Treatment of Pancreatic Cancer
The various causes of pancreatic cancer remain largely unknown, but several common risk factors have been found. Age is one of the most important risk factors, and most pancreatic cancer patients are over the age of 50. 12 Smokers are two to three times more likely to develop pancreatic cancer than non-smokers. 13 Chronic pancreatitis, type 1 diabetes, and obesity are other notable risk factors. 14 Only about 10% of pancreatic cancer patients have a positive family history. 15 Most pancreatic cancers are a subtype of pancreatic ductal adenocarcinoma (PDAC). 16 Like other cancers, PDAC is generally believed to originate from precursor lesions known as pancreatic intraepithelial neoplasia. The lesion is formed by the initial mutation of Kras, TP53, CDKN2A, SMAD4, RNF43, ARID1A, TGFβR2, GNAS, RREB1, PBRM1, and other genes. 17 Kras wild-type tumors contain alterations in other oncogenic drivers including GNAS, BRAF, CTNNB1, and other RAS pathway genes. 18 With the subsequent acquisition of additional mutations, the lesion becomes more and more dysplastic and invades through the basement membrane, leading to invasive PDAC. 19
In the past 2 decades, the immune system has been shown to play a vital role in the development and progression of various types of cancers. Immune evasion is considered as a new sign of cancer. 20 To survive, tumor cells must be able to escape the immune destruction by innate and adaptive immune cells. Although inflammation usually promotes the clearance of bacteria and foreign debris, and contributes to the repair of damaged tissues, its role in tumor evasion is much more complex. 21 In the early stages of cancer, the host immune system detects incompatible tumor cells and eliminates them through the action of natural killer cells and CD8+ T cells. However, as the cancer develops, this normal monitoring eventually becomes ineffective in curbing tumors. 22 Therefore, enhancing the body's own humoral immunity or the positive role of cellular immune pathways to heighten the surveillance role of body immunity to achieve the goal of killing tumor cells is the focus of research on immunotherapy. Because of its potential as a targeted therapy, the mechanism of immunosuppression in the TME has become an important research topic. 23 Several therapeutic drugs have been explored with or without combination with the standard treatment of gemcitabine, 5-fluorouracil (5FU), oxaliplatin, nab-paclitaxel, or FOLFIRINOX, that have slightly lengthened the survival time of PDAC.24,25 Although these therapies are commonly used for pancreatic cancer treatment, their efficacy may be hampered by cell resistance and interference resulting from the contradictory promotion of the immunosuppressive environment of the whole body and the TME. 26
Classification of MDSCs
Studies in the early 1900s revealed that cancer is often accompanied by extra-medullary hematopoiesis (EMH) and neutrophilia, these immature leukocytes are characterized by their suppressive activity and are called myeloid-derived suppressor cells (MSCs), this term was further changed to MDSCs. 27 MDSCs are an immature population of myeloid cells found mainly in patients and in mice with cancer, and they have also been found in non-human primates such as macaques. 28 GR-1 and CD11b are major markers for the typing of murine MDSCs, and GR-1, in turn, consists of a marker molecule representing macrophages (Ly6C) and a marker representing neutrophils (ly6G). Mouse MDSCs were divided into monocytic MDSCs (M-MDSCs) subsets according to the above markers, with surface markers CD11b+ Ly6Chigh Ly6Glow/−, and granulocytic MDSCs (G-MDSCs) /polymorphonuclear (PMN-MDSCs) subsets, with surface markers CD11b+ ly6Clow/− ly6G+. Human MDSCs do not express GR-1 thus their classification characteristics are more complex, usually, the phenotype of MDSCs in human peripheral blood mononuclear cells (PBMCs) is CD33+, CD11b+, and HLA-DR low/−, and human MDSCs are classified as G-MDSCs and M-MDSCs based on the presence of CD15 and CD14 marker. 29 Another human MDSCs subpopulation is early MDSCs (e-MDSCs) that still do not acquire a granulocytic or monocytic phenotype, which is characterized phenotypically by (CD3, CD20, CD56) −, CD33+, CD11b+, and HLA-DR−.30,31 Additional markers of human MDSCs found by flow cytometry, such as CD16, CD38, and LOX-1, may provide a reference for subsequent typing. 32 Several studies have shown that CD56, NKG2a, and NKp46 are important markers for differentiating human and macaque MDSCs, but in fact, the phenotype, function, and distribution of the two MDSCs are not so different. 30
All MDSCs subsets have the ability to suppress immune responses, but different subsets of MDSCs have different mechanisms of suppression. G-MDSCs suppress immune responses by producing arginase-1 (Arg-1), reactive oxygen species (ROS), prostaglandin E2 (PGE2), and peroxynitrite. M-MDSCs respond to growth factors by using regulatory molecules such as PD-L1, TGFβ, IL10, and generates nitric oxide (NO) to exert their immunosuppressive effects.33,34
Multiple Cytokines Are Involved in Activating the Immunosuppressive Properties of MDSCs
Several different growth factors are involved in the tumor growth, but GM-CSF is the most known one. GM-CSF preferentially increases M-MDSCs. 35 GM-CSF is usually produced in response to infection to enhance the innate immune response, but studies have suggested that malignant pancreatic epithelial cells also produce a large amount of GM-CSF. 36 Influenced by the increase in GM-CSF, myeloid progenitor cells in bone marrow differentiate into MDSCs, migrate to systemic circulation, and aggregate in the spleen and tumor. 37 When antibodies were used to block the increase of GM-CSF, the number of GR1+ CD11b+ cells recruited by the tumor decreased and the tumor progression was impaired. 38 In addition, the latest research shows that this upregulation in mice depends on carcinogenic KrasG12D, which is significant because the Kras mutation is very common in human pancreatic cancer. 39 The use of gemcitabine and fluorouracil chemotherapy upregulates GM-CSF in the absence of aseptic inflammation and tumor cell death, which may contribute to the low response of pancreatic cancers to chemotherapy. 40 In renal cell carcinoma, chemotherapy decreases the number of MDSCs in the spleen but fails to decrease the number of MDSCs in the TME. 41 Perhaps this differential reduction is due to the increased level of GM-CSF caused by chemotherapy itself. 42 G-CSF is another factor that induces the proliferation of MDSCs, but this factor primarily increases the number of PMN-MDSCs, which are less immunosuppressive. 43
Other factors, such as IL-6, IL-1β, CXCL1, and VEGF-A, have also been shown to affect the proliferation of MDSCs in a variety of tumor types. 44 Studies45,46 have shown that serum IL-6 can promote MDSCs proliferation and all subsets of MDSCs are associated with immunosuppression in pancreatic cancer patients, with M-MDSCs and G-MDSCs exhibiting immunosuppression mainly through increased expression of ARG-1, PD-L1, and ROS activity. IL-1β, a tumor-associated factor that leads to the proliferation and migration of MDSCs, is regulated by the IL-1 RI/NF-κB pathway, and studies have confirmed that increased serum IL-1β levels correlate with the frequencies of M-MDSCs and Tregs. IL-1β can trigger a transition from non-alcoholic fatty liver disease to severe fibrosis, which in turn leads to liver cancer. In addition, IL-1β can also increase cyclooxygenase-2 (COX-2) expression, which in turn activates tissue endothelial cells to produce vascular endothelial growth factor and other angiogenic factors to induce endothelial cell proliferation and vascularization within tumor tissues. 47 Additionally, study of Wang et al. 48 confirmed that VEGF-A secreted by primary tumor cells stimulated CXCL1 production by tumor-associated macrophages, which recruited CXCR2 positive MDSCs to form a pre-metastatic niche to promote liver metastasis.
Epithelial–mesenchymal transition (EMT) is a reversible cellular program that transiently places epithelial cells into quasi-mesenchymal cell states, EMT enables tumor cells to have greater invasion and metastasis potential and generates greater therapeutic resistance. 49 CCR4+ M-MDSCs increased EMT in pancreatic cancer patients by modulating the CCL2-CCR4 axis and then increasing the expression of mesenchymal transition markers N-Cadherin, Snail, and ZEB1. 50 Recent studies51,52 have shown that MDSCs play a role in the induction of EMT and that they can promote the generation of cancer stem-like cells and do so by secreting TGFβ and activation of the COX2, EGF, and HGF pathways to promote cancer cell spread. Cancer-associated fibroblasts (CAFs) and their extracellular matrix (ECM) enhance immunosuppression by promoting angiogenesis, ECM remodeling, and secretion of tumor-promoting and immunosuppressive cytokines, chemokines, and growth factors such as EGF, HGF, CCL2, TGFβ1, and VEGF. 53 And in recent years there has been a study 54 showing that the CCL5-CCR5 axis is involved in MDSC recruitment and their immunosuppressive effects, and can promote tissue fibrosis. Collectively, the above cytokines may play a role in promoting fibrosis, EMT, and invasive immunosuppression by activating the immunosuppressive properties of MDSCs.55,56
Role of MDSCs in Pancreatic Cancer
MDSCs mobilized into systemic circulation and spleen and are eventually absorbed into the TME. 57 MDSCs play critical roles in immunosuppression and tumor promotion in the TME through a variety of mechanisms: blocking lymphocyte homing, inducing immunosuppressive cells, producing reactive oxygen species and nitrogen, consuming metabolites vital to T cell function, expression of external enzymes regulating adenosine metabolism, and expression of negative immune checkpoint molecules. 58
Myeloid cells constitute the main body of the innate immune system, performing a plethora of functions ranging from engulfment to processing antigens and delivering antigens to more specialized immune cells. 59 Recent studies60,61 suggest that crosstalk with MDSCs may play a role in the functional regulation of these cells, which in turn create a suppressive microenvironment that supports tumor growth. MDSCs may affect macrophage polarization, function, and activation status through crosstalk with macrophages. The crosstalk of MDSCs can promote the polarization of macrophages to the M2 phenotype by producing interleukin-10 (IL-10). Crosstalk with MDSCs may also lead to reduced expression of macrophage MHC II, which in turn reduces the antigen-presenting capacity of macrophages, further causing immunosuppression.62,63 Crosstalk between MDSCs and dendritic cell (DC) also results in impaired antigen uptake, presentation, and migration by DC, which ultimately skews DC toward an anti-inflammatory component, leading to decreased interferonγ production by T cells. 64 The tumor-promoting activity of tumor-associated neutrophils (TANs) is closely associated with PMN-MDSCs, and crosstalk between them would polarize neutrophils in the tumor microenvironment toward an N2 type biased immunosuppressive effect. 65 At the same time, MDSCs can also interact with unconventional and innate type lymphoid lineage cells (eg, NK T cells, γδ T cells, and NK cells) crosstalk to exert immunosuppressive effects.66,67 In PDAC patients, the number of MDSCs in the systemic circulation has been shown to be associated with the stage of the disease. 68 Pancreatic stellate cells secrete chemokines in vitro and induce peripheral blood myeloid cells to differentiate into MDSCs through a STAT3-dependent mechanism. 69 There is evidence that some of these factors depend on specific microRNAs to cause proliferation. In the myeloid cells surrounding pancreatic cancer, the level of miRNA-21 has been found to increase, whereas blocking miRNA-21 and miRNA-155 is related to a decrease in MDSCs levels. 70
The Significance of MDSCs in Pancreatic Cancer and Therapy in Preclinical Studies
Several studies have demonstrated the role of MDSCs in masking the antineoplastic immune response in pancreatic cancer models. Our study shows that some factors such as interferon regulatory factor 4 (IRF4), antibodies against the PDA-associated antigena-enolase-1 (ENO1), Src Homology-2 (SH2) domain-containing inositol 5’-phosphatase-1 (SHIP-1), and CXCR2 inhibition can exert positive antitumor effects by inhibiting MDSCs, and some factors such as the epidermal growth factor receptor (EGFR), mitogen-activated protein kinases (MAPK), lactate, the receptor for advanced glycation end products (RAGE), STAT3, vascular endothelial growth factor (VEGF) can play a negative anti-tumor role. (The details of the studies are summarized in Table 1).
Summary of Preclinical Studies Defining the Role of MDSCs in Pancreatic Cancer and/or Therapy Efficacy.

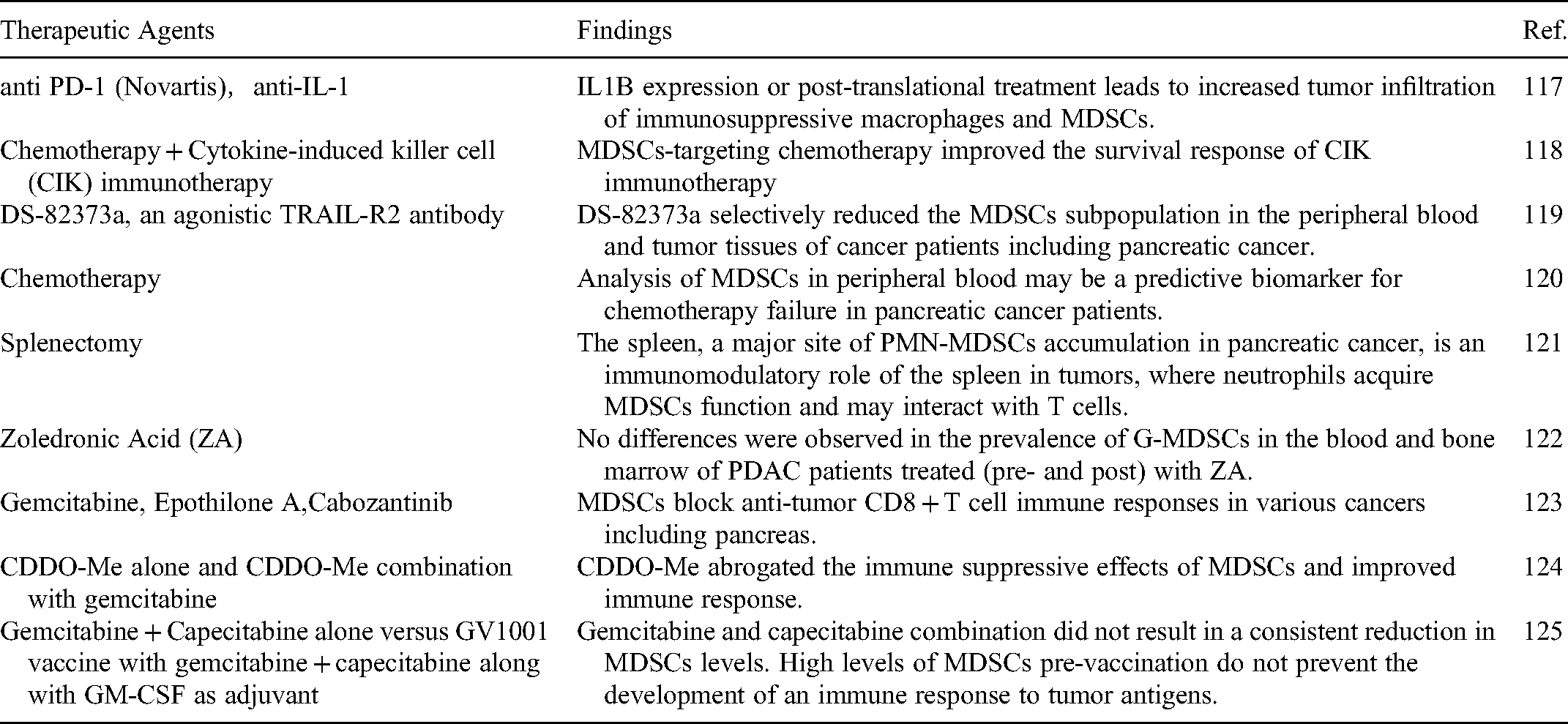
The Role of MDSCs in Pancreatic Cancer and Therapy in Clinical Studies
Multiple clinical studies have evaluated MDSCs in patients with PDAC and explored ways to target MDSCs with or without therapeutic agents, such as anti PD-1 (Novartis), anti-IL-1, chemotherapy, DS-82373a, splenectomy, Zoledronic Acid (ZA), gemcitabine, Epothilone A, Cabozantinib, and CDDO-Me in this population (Table 2).
Summary of Clinical Studies Defining the Role of MDSCs in Pancreatic Cancer and/or Therapy Efficacy.
Treatment of Targeted MDSCs
In the past, RT has been the front-line treatment for cancer patients. At present, about 60% of newly diagnosed cancer patients regard it as the first-line treatment. 71 By exposing the tumor to different energy rays, RT can cause irreversible damage to the DNA of tumor cells, promote the release of tumor antigens, activate anti-tumor immune response, increase the production of cytokines, and inhibit the proliferation of tumor cells. 72 RT can promote local and systemic antitumor immunity. 73 However, bone marrow-derived cells (including TAMs and MDSCs) in tumors often counteract with the immune responses. 74 Radiotherapy can have antitumor or tumor promoting effects, depending on the doses, grades, and tumors, through recruitment, removal, repolarization, and recombination, and using bone marrow-derived cells in tumors to induce antigen representation. 75 For MDSCs, cancer RT has two possible effects: either increase or decrease MDSCs function. On one hand, recruitment of bone marrow cells to the tumor because of RT is proposed to occur through the CSF1/CSFR signaling pathway. 76 The number of MDSCs and the level of macrophage colony stimulating factor 1 (CSF1) in the spleen, lymph nodes, and peripheral blood increase systematically after radiation exposure. 77 Further studies found that the sharp increase of CSF1 gene expression after RT of nasopharyngeal carcinoma was through the recruitment of the DNA damage induced kinase ABL1 into the nucleus, where it binds to the CSF1 gene promoter to enhance its transcription. 78 Local RT increases the tumor infiltration of MDSCs through the CSF1/CSF1R signaling pathway. If the CSF1/CSF1R signaling pathway is blocked, tumor recurrence after local RT can be inhibited. 79 In addition, the STING-type I interferon pathway was also found to enhance inflammation and tumor inhibition. 80 Stimulation of NF-kappaB by radiation can upregulate COX2, induce the production of the immunosuppressive factor PGE2, and trigger the production of MDSCs. 81
On the other hand, RT in combination with immunotherapy can effectively inhibit the function of MDSCs and promote the cytotoxic effect of CD8+ T cells in tumors. 82 Targeting MDSCs to enhance antitumor immunity is known as ablative hypofractionated radiation therapy (AHFRT). 83 AHFRT is more effective in cancer treatment when combined with anti-PD-L1 immunotherapy. 84 One study found that the combination of stereotactic body RT (SBRT) and sunitinib (an oral, small molecule, multi-target receptor tyrosine kinase (RTK) inhibitor) can rapidly reduce the proportion of Treg and MDSCs. 85 In animal models of spontaneous breast cancer (TUBO tumor) and colon cancer (CT26 and MC38), anti-PD-L1 combined with RT can effectively decrease the accumulation of MDSCs, activate CD8 + T cells, and finally, inhibit the growth of tumors.86,87 In addition, the local up-regulation of PD-L1/PD-1 axis after RT inhibits the radiation-induced immune response, thus limiting the expression of antitumor immunity and promoting recurrence. The combination of RT and PD-L1 blockers can optimize antitumor immunity, resulting in the elimination of MDSCs by enhancing the production of T cell-derived TNF. 88
The important roles in MDSCs in regulating tumor growth have stimulated the research on targeted therapy of these cells. MDSCs accumulation is closely associated with the clinical outcome of cancer patients, 89 and MDSCs are associated with drug resistance to antitumor therapies, including cisplatin, sunitinib, and other chemotherapeutic drugs in lung cancer, and doxorubicin and melphalan in multiple myeloma.90,91 Recent studies have shown that MDSCs levels are related to patients’ response to CTLA4/ipilimumab and PD-1. 92 MDSCs can be eliminated by chemotherapy with relatively low doses of gemcitabine and 5-fluorouracil. 93 Recent studies have shown that targeting the TRAIL receptor may be an effective and selective method to deplete MDSCs population. 94 The peptide body composed of S100A9 derived peptide and antibody Fc fragment shows the potential to eliminate MDSCs in a mouse model. MDSCs can be functionally inactivated by targeting its inhibitory mechanism. 95 Recent clinical reports have shown that patients with head and neck cancers and multiple myeloma when treated with the PDE-5 inhibitor tadalafil have fewer circulating MDSCs, lower expression of iNOS and arginase in these cells, and more spontaneously generated tumor-specific T cells. 96 Nrf2 is a transcription factor and it plays an important role in protecting cells from free radical damage. The synthesized triterpenoids reduce the production of ROS through MDSCs and inhibit the activity of ROS by up-regulating Nrf2. 97 Inhibition of COX-2 can down regulate the production of immunosuppressive prostaglandin E2, while nitroaspirin has been shown to down-regulate the production of NO. 98 The class I HDAC inhibitor entinostat has an inhibitory effect on MDSCs, but its mechanism is not clear. 99 All-trans-retinoic acid (ATRA) can target the expansion and differentiation of MDSCs. In patients with lung cancer that receive a short-term ATRA treatment, the immune response to the p53 vaccine is improved.100,101 Inhibition of STAT3 can induce MDSCs to differentiate into immunogenic DC. 102 A targeted antibody to phosphatidylserine (PS) can reduce the number of MDSCs in tumor-bearing mice, but its mechanism is not clear. 103
Conclusion
Preclinical and clinical studies have indicated that a variety of immune cells, cytokines/chemokines and signaling pathways play an important role in modulating the immunosuppressive function of MDSCs. MDSCs affect the progression, invasion, metastasis, and survival of pancreatic cancer patients. In human patients with pancreatic cancer and in mouse pancreatic tumor models, MDSCs inhibit the antitumor immune response of therapeutic drugs. MDSCs can be applied as a potential biomarker for evaluating tumor progression, defining the outcome of immunotherapy or chemotherapy in patients with pancreatic cancer. Targeting MDSCs could improve the efficacy of standard chemotherapy and immunotherapy. In addition, new interventions are aimed to understand the function of MDSCs and the exact mechanism(s) underlying their immunosuppressive activity, with the objective to provide a breakthrough for cancer treatment.
Footnotes
Abbreviations
Acknowledgments
No.
Data Availability
The datasets presented in this study are available from the corresponding author upon request.
Ethics Statement
The data need no ethic statement.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was supported by the Tumor prevention and control Joint Fund of Shandong province natural science fund (ZR2019LZL008), Clinical Research Fund of Shandong Medical Association-Qilu Special Project (YXH2022ZX02199), Bethune-Cancer Radiotherapy Translational Medicine Research Fund (flzh202113), Shandong Province Medicine and Health Science and Technology Development Plan Project (202009031334), and Basic Scientific Research Foundation (1191320113 to Y.Z.H).