
Abstract
Introduction
Hepatoblastoma (HB) is the most common hepatic malignancy in children, accounting for approximately 0.8% to 2.0% of all of the pediatric malignancies1,2 and usually occurring before the age of 3. 3 Although the pathogenesis of HB is unknown, it has been believed to be associated with preterm birth, low birth weight, genetic disorders such as Beck–Wiedemann, and familial adenomatous polyposis syndrome.4,5 The current treatment strategies for children include combination chemotherapy and curative resection of the primary tumor. 6 Moreover, even after surgery and intensive chemotherapy, a significant proportion of patients with HB is at risk of local or recurrent or distant metastasis. The main reason might be that most children with HB are diagnosed in the progression stage or stage 3 or 4.7,8 Therefore, early diagnosis, prognosis prediction, and effective therapies are still a utopia for this disease. As such, novel biomarkers for diagnosis and prognosis are urgently needed.
MicroRNAs (miRNAs) are small endogenous (19-23 nt) non-coding RNAs that promote cell fate determination, proliferation, and cell death.9-11 Growing evidence has indicated that miRNAs are involved in several pathophysiological processes of HB.12,13 On the basis of the dysregulated expression from tumor tissue or blood, miRNAs have been identified to correlate with the diagnosis of HB and may contribute to its treatment and prognosis. By searching the research on relevant topics, we found that different studies have reported inconsistent results and doubted whether miRNAs could be ideal biomarkers for the clinical application of HB patients. For example, Liu et al 14 found that plasma-origin miR-21 from HB patients was significantly more highly expressed than normal miR-21 (sensitivity, 68%; specificity, 70%). Furthermore, in Frowein's study, 15 miR-492 had a better diagnostic performance in HB tissue samples (sensitivity, 87.5%; specificity, 75%). Meanwhile, a similar conclusion could be drawn from various prognostic studies. Cui et al 16 confirmed that up-expressed miR-193a might be a good prognostic predictor and therapeutic target in HB (OS, HR value = 2.39). However, Jiao et al 17 confirmed that miR-34b could be an independent prognostic factor related to HB, but the HR value of miR34b was less obvious (OS, HR value = 1.43). As the different performance might be explained to be due to different miRNAs or research and methods, we think that it is necessary to pool all of the available studies to identify the diagnostic and prognostic performance and judge whether miRNAs could be applied clinically.
Methods
Search Strategy
In order to retrieve all of the articles analyzing the diagnostic and prognostic value of miRNAs in patients with HB, a comprehensive literature search (updated on December 01, 2019) in PubMed, Cochrane Library, EMBASE, and Web of Science databases was performed. The following medical subject headings (MeSHs) and free words in the literature retrieval were used: “hepatoblastoma” and “miRNA” or “microRNAs” or “miRNA” or “microRNA” or “RNA, micro” or “miR” or “primary microRNA” or “circulating microRNAs” or “circulating miRNA” and “diagnosis” and “prognosis” or “sensitivity” and “specificity.” We searched for relevant articles whenever possible to evaluate the text.
Study Selection Criteria
The studies included in our meta-analysis met the following criteria: (1) the relationship between miRNA and HB was analyzed in the study; (2) a definitive diagnosis of HB was conducted using the gold standard (such as histological confirmation); and (3) the articles provided sufficient data. In addition, we only included publications in English. The studies excluded from our meta-analysis met the following criteria: non-English, letters, reviews, expert opinions, and non-peer reviewed articles (eg, dissertations or conference proceedings).
Data Extraction
Two investigators screened the relevant studies independently on the basis of the title and the abstract, and the full text. Any differences were resolved through discussion with the author. The following data were extracted from the eligible studies: first author's name, publication year, country, miRNA type, ethnicity, source of sample, the number of cases and controls, diagnostic data, and prognostic data.
Quality Assessment
This meta-analysis was performed following the guidelines of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement. 18 For the diagnosis meta-analysis, the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies 2) was performed to evaluate the methodological quality assessment of the included articles. For the prognosis meta-analysis, the quality of the included studies was evaluated with the Newcastle Ottawa Scale (NOS).19,20 NOS scores were calculated on the basis of selection, comparability, and outcome. Studies with a final score of >6 were considered to be of a high quality.
Statistical Analyses
The statistical analyses of this study were performed using the Review Managers V5.3 and the Meta Disc 1.40 software. The numbers of patients with true positives (TP), false negatives (FN), false positives (FP), and true negatives (TN) from the included studies were extracted. We calculated the combined specificity, sensitivity, the combined positive likelihood ratio (PLR), the combined negative likelihood ratio (NLR), the diagnostic odds ratio (DOR), and the AUC of the summary receiver operating characteristic (SROC) using Meta Disc. 21 Firstly, we calculated the spearman correlation coefficient to determine whether there was threshold effect in our meta-analysis. If P>.05, it indicated that there was no threshold effect, and then the study effect quantity could be combined. Additionally, the heterogeneity among studies was estimated with the Q test and I2 statistics. If I2 <50%, which means the absence of heterogeneity, a fixed-effects model with the Mantel-Haenszel methods would be applied. Otherwise, if the I2 value was more than 50%, which indicated the existence of significant heterogeneity, a random-effects model based on the DerSimonian and Laird method would be used. Different sample size, race from Europe or Asia, various examining measurements, and different resourced specimen maybe resulted in significant heterogeneity. Thus, we performed the subgroup and meta-regression analyses to explore the potential sources of inter-study heterogeneity. Deeks’ funnel plot was used to evaluate the potential publication bias, and a P-value of <.05 was considered to be statistically significant among the enrolled studies.
For the prognostic studies, the HRs and their 95% CIs for OS and EFS were extracted. Pooled HR values with 95% CI were used to assess the relationship between the miRNAs and the HB prognosis. An observed HR of >1 indicated poor prognosis in patients with a high miRNA expression. Conversely, an observed HR of <1 indicated the good prognosis in patients with a high miRNA expression. The heterogeneity assessment was performed with a Q test and I2 statistics. The values of I2≥50% and P<.1 indicated the existence of significant heterogeneity. 22 Because of samples from different HB patients (formalin-fixed samples, frozen tissue samples, serum samples, and plasma samples) and cut-off values in individual studies, the random-effects model was adopted preferentially. Subgroup and meta-regression analyses were performed to explore the source of heterogeneity. We drew Deeks’ funnel plots to test the publication bias in this meta-analysis. The value of P<.05 was considered statistically significant.
Results
Study Selection and Characteristics of Eligible Studies
Our meta-analysis has submitting details of systematic review protocol to the INPLASY register (NO. 2021110045; DOI 10.37766/inplasy2021.11.0045). As shown in Figure 1, in all, 332 articles were initially identified using the major literature retrieval strategies, from PubMed, EMBASE, Cochrane Library, and Web of Science. Duplicate records (n = 158) were removed. After a review of their abstracts and titles, 151 articles were deleted as they were reviews, letters, animal research, or irrelevant studies. After careful full-text reading, we found that 17 articles lacked sufficient data for the meta-analysis or were unrelated to the diagnosis or prognosis. As a result, 20 studies (including 10 for the diagnostic analysis and 10 for the prognostic analysis) from 6 articles were included in the current meta-analysis. For example, in Jiao's article, we could conclude that there were 3 included miRNA (miR-34a, -34b, -34c) that could be pooled in diagnostic meta-analysis. That means 3 different studies not only with different microRNA, but also maybe with different sample size, ratio of sex, and diagnostic accuracy. The basic characteristics of 20 studies are summarized in Tables 1 and 2.

Flow chart of the selected process according to PRISMA 2009.
Main Features of 10 Included Studies in Diagnostic Meta-Analysis.

Abbreviations: TP, true positive; FP, false positive; TN, true negative; FN, false negative.
Main Features of 10 Included Studies in Prognostic Meta-Analysis.

Abbreviations: MiR, microRNA; HR, hazard ratio; CI, confidence interval; OS, overall survival; EFS, event-free survival; RT-PCR, reverse transcription PCR; qRT-PCR, quantitative reverse transcription PCR.
Quality Assessment
The diagnostic studies were consistent with the criteria in QUADAS-2, suggesting that the enrolled studies were suitable for quantitative integration. The bias risk and applicability concerns are detailed in Figure 2. NOS was used to evaluate the prognostic studies, with an average score of 6.6, indicating that the enrolled studies were of a high quality (Figure 3).

Overall quality assessment of included articles using the QUADAS-2 tool: (a) summary and (b) graph. Newcastle–Ottawa quality assessments scale.

Newcastle–Ottawa quality assessment scale.
Threshold Effect
The overall Spearman's correlation coefficient across the 10 studies considered in the diagnosis analysis was 0.248 (P = .49), which indicated no threshold effect.
Diagnosis and Prognosis of miRNAs
Ten studies involving 171 patients and 121 controls were evaluated to obtain the diagnosis value of miRNAs for HB. Among these 10 studies, only 1 was conducted in Europe; the rest of the studies were conducted in Asia. Three different samples were used in this study, namely serum (n = 2), plasma (n = 1), and tissue (n = 2). Quantitative reverse transcription PCR (qRT-PCR) was used to detect the expression of miRNAs. Forest plots of the pooled data from 10 studies, corresponding to the sensitivity and the specificity of miRNAs in diagnosing HB, are shown in Figure 4. The results were as follows: sensitivity of 0.76 (95% CI: 0.72-0.80) and specificity of 0.75 (95% CI: 0.70-0.80). Significant heterogeneity was observed (I2 = 66% and I2 = 54.1%); therefore, the random-effects model was used in this study. Pooled PLR, NLR, and DOR are shown in Figure 5. Additionally, the SROC curve was plotted in Figure 6, and the AUC was 0.83, suggesting that miRNAs had a relatively high diagnostic value for HB. Considering the I2 >50%, it is necessary to conduct the meta-regression and subgroup analysis to explore the sources of heterogeneity between studies. Based on different potential factors, the meta-regression analysis was analyzed and revealed that factors such as specimens, sample size, and different races had little influence on the study (all P>0.05). However, RNA measurements might be a source of heterogeneity in the study (P = .04), particularly the sensitivity (Table 3).

Forest plots of (a) sensitivity and (b) specificity in HB diagnosis.

Forest plots of (a) PLR, (b) NLR, and (c) DOR in HB diagnosis.

SROC of miRNA test in HB diagnosis.
Subgroup and Meta-Regression Analysis in Diagnosis Meta-Analysis.

* indicates p value less than 0.05 and means significant differences. Abbreviations: AUC, area under curve; CI, confidence interval.
Ten studies involving 242 patients and 196 controls were evaluated the prognosis value of miRNAs for HB. Eight miRNAs were identified in HB patients. The miRNA expression was analyzed using a qRT-PCR assay for the tissues, serum, and plasma obtained from the HB patients. Seven studies evaluated the correlations between abnormal miRNA expressions and OS, representing 182 patients. Three studies evaluated the relationship between miRNA expressions and EFS, representing 60 patients. Three increased miRNAs (miR-222, miR-224, and miR-492) and 5 decreased miRNAs (miR-21, miR-193a, miR-34a, miR-34b, and miR-34c) were found to be associated with very poor survival in HB. The combined HR (95% CI) for OS was calculated as 1.74 (95% CI: 1.20-2.29), indicating that miRNAs were significant prognostic biomarkers for HB patients. HR >1 revealed that the listed abnormal miRNAs were associated with a poor prognosis in HB. No heterogeneity was observed among the selected studies (I2 = 00.00%, P = .981). The random-effects model was applied in these studies (Figure 7). The pooled HR (95% CI) for EFS was calculated to be 1.74 (95% CI: 1.31-2.18). There was no heterogeneity in the included studies (I2 = 00.00%, P = .588). Lastly, we conducted the sensitivity analysis in the prognostic part of microRNAs. The results indicated the good literature quality evaluation.
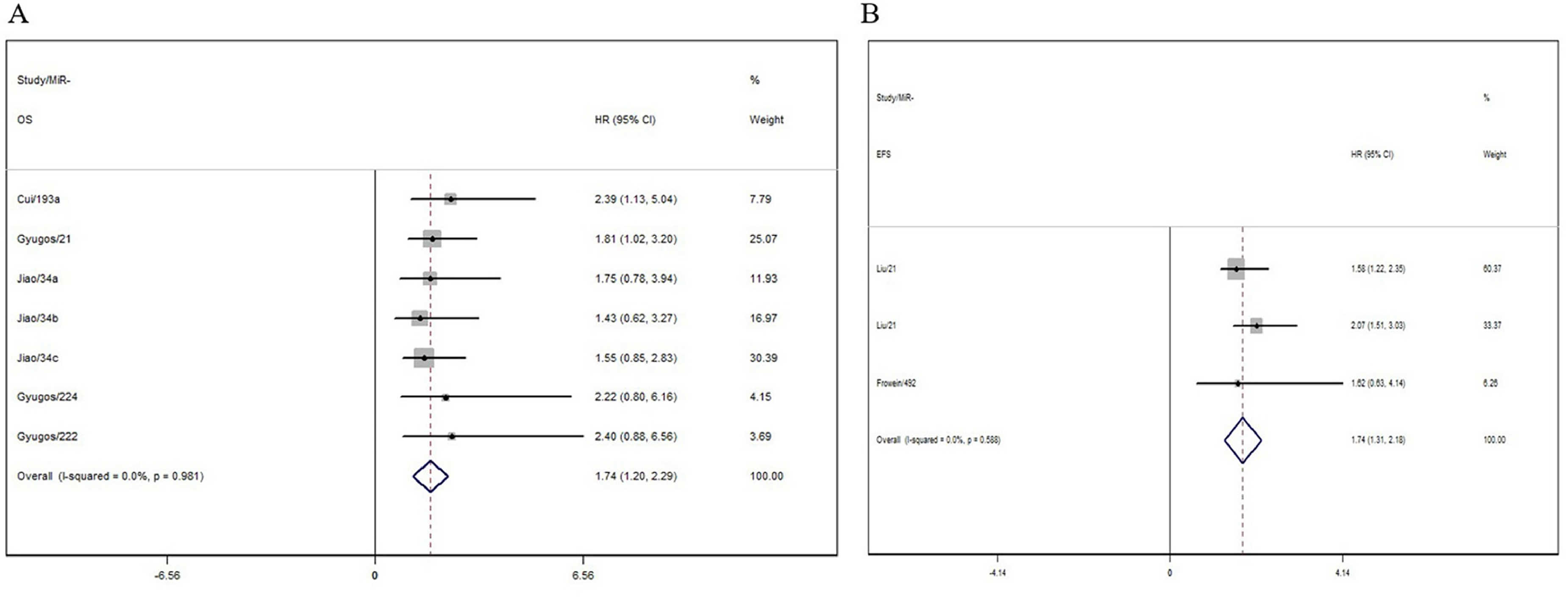
Forest plots of relationship between miRNA expression levels and HB prognosis: (a) OS and (b) EFS.
Publication Bias
In diagnostic studies, the pooled Deeks’ test result was P = .582 (Figure 8a), which indicated that there was no significant publication bias in this analysis. In the prognostic studies, the Begger plots for the OS/EFS meta-analysis are shown in Figure 8b and c, which suggested that no publication bias existed.

Funnel plot analysis of potential publication bias: (a) Funnel plots of studies included in diagnosis meta-analysis, (b) OS, and (c) EFS. Abbreviations: ESS, effective sample size; HR, hazard ratio; OS, overall survival; EFS, event-free survival.
Discussion
HB is a pediatric tumor that arises from hepatic progenitors or hepatoblasts, with an annual incidence rate of 1.5 cases per million that represents around 1% of the total cancers in childhood.25,26 Early diagnosis, prognosis prediction, and effective therapies are still a utopia for HB. Most children are diagnosed at Pre-Treatment Extent of Disease staging System (PRETEXT) III or IV, particularly in China, with poor prognosis and low long-term survival. Therefore, early diagnosis and targeted treatment are essential to improve the survival in patients with HB. The early diagnosis of HB without histology depends on a tumor in the liver, a high alpha-fetoprotein (AFP) level and an age between 6 months and 3 years. Moreover, the AFP declining after neoadjuvant chemotherapy is considered to have a strong prognostic value.25,27,28 However, the sensitivity and the specificity of AFP are not high because of the various sources from the fetus. Therefore, a large number of researchers are committed to finding appropriate non-invasive biomarkers to predict the diagnosis or prognosis of HB, hoping to provide directions for clinical treatment. To our knowledge, this is the first time to use meta-analysis to verify the diagnostic value of HB from the perspective of miRNAs.
MiRNAs play a key role in the regulating processes of HB, such as proliferation, differentiation, apoptosis, invasion, angiogenesis, and metastasis via gene expression manipulation. 29 Frowein et al 30 reported that miR-492 was overexpressed in metastatic HB and played an oncogenic function in HB, enhancing proliferation, anchorage-independent growth, migration, and invasion. They also suggested that miR-492 could be a strong biomarker of worse prognosis during the tumor progression of HB. Moreover, studies have shown that a high expression of miR-21 can promote the migration and invasion of HB.31-33 Gyugos 24 report revealed that high miR-21 and low miR-222 and miR-224 levels were associated with the increased overall survival of SIOPEL-treated HB patients. However, the results from different studies focusing on the diagnostic or prognostic performance may be inconsistent. Thus, this meta-analysis appears to be necessary to figure out the diagnostic and prognostic value of miRNAs for HB.
In the diagnostic meta-analysis, the pooled results of a SEN of 0.76 (95% CI: 0.72-0.80), a SPE of 0.72 (95% CI: 0.70-0.80), DOR of 10.24 (95% CI: 6.55-16.00), and AUC of 0.83 showed that miRNAs as potential biomarkers had a moderate influence on HB and its diagnostic accuracy. However, the PLR and NLR were 2.79 (95% CI: 2.12-3.66) and 0.34 (95% CI: 0.26-0.45), suggesting that miRNAs might not be insufficient to distinguish between HB patients and healthy individuals, because PLR>10 and NLR<0.1 were the thresholds representing a high accuracy. Using I2 > 50% from the forest plot, we found that heterogeneity existed in the data synthesis and analysis. Consequently, a subgroup analysis and a meta-regression analysis were performed; the results revealed that the different detection methods might be the possible sources of heterogeneity. Other factors, such as sample size, ethnic differences, and specimen orientation, might not contribute to heterogeneity. Moreover, the subgroup analysis confirmed that the SEN and SPE values obtained using the TaqMan detection method were better than those obtained using other methods. This might contribute to the limited number of studies with a restricted diagnostic accuracy. According to the 10 included studies, miRNAs could be stably detected in the blood (5 cases) and tissues (5 cases) of HB patients with significant differences, when compared with the control samples, suggesting that they might have potential applications as noninvasive biomarkers.
In our meta-analysis for the prognosis, the HRs and 95% CIs extracted from the studies were combined to analyze the relationship between the miRNA expression and the HB prognosis. The prognostic meta-analysis results suggested that the dysregulation of miRNAs (miR-34a, miR-34b, miR-34c, miR-21, miR-222, miR-224, and miR-193a) was associated with worse overall survival of HB patients, and the aberrant expression of miRNAs (miR-21, miR-492) was relevant to the poor EFS of the HB children. We performed a random-effects model analysis to calculate the pooled HR. Overall, our finding showed that a significantly positive relationship existed between the aberrant expression of miRNAs and the worsened prognosis in HB patients (HR = 1.74, 95% CI = 1.20-2.29, P<.001 for OS; HR = 1.74, 95% CI = 1.31-2.18, P<.001 for EFS). As we mentioned, some researchers conducted the joint diagnosis of HB with 4 genes, the HR value of OS is 6.202 and EFS is 3.611. 34 Typically, an HR of more than 1.5 is deemed a moderate prognostic factor. Our pooled HR was 1.72, indicating that miRNAs might be valuable prognostic biomarkers for HB patients. However, these conclusions were not persuasive enough due to some HRs of included studies were not statistically significant. It needed to be refined for some reasons. For example, miRNAs have been measured in tissue or serum, as these measurements might introduce overestimation of HR in one meta-analysis. In addition, we noticed that the relative lower HR value was single for each miRNA and not the combined one. If combined together, the HR value of joint diagnosis would be believed to be improved to a certain degree. In addition, microRNAs not only have the potential roles of prognosis of HB, but also have moderate accuracy of diagnostic value in HB diagnosis from our pooled results.
The mechanism of miRNAs in HB progression has been well identified to be associated with its pivotal signaling pathways. 35 Toyota et al 36 reported that the ectopic expression of all the members of the miRNA-34 family induced cell cycle arrest in a variety of cancer cell lines by the repression of their targets Cyclins D1 and E2, and the cyclin-dependent kinases CDK4 and CDK6. Dong et al 37 proved that transfection with a precursor of miR-34a-5p significantly reduced the HB tumor growth in vivo, as well as the microvascular density and number of proliferating tumor cells, which further emphasized the role of this miR in tumor angiogenesis. Frowein et al 15 proposed the ability of oncogenic miR-492 to regulate the progression of HB metastasis through CD44. In other words, the altered expression of miRNAs might have diagnostic or prognostic significance 38 and could be used to identify the clinicopathological features of the disease.
The meta-analysis has several limitations. First, the sample size was still relatively small in this study. Therefore, more studies based on larger samples and sufficient data are required to verify the diagnostic and prognostic value of miRNAs in HB. Second, the results might be inaccurate, as this study was based on a group of miRNAs rather than a single miRNA. In the process of the relevant literature search, we found that the number of a certain type of miRNA was too small. Therefore, we chose these different miRNAs instead of a certain type of miRNA. We now hope to promote the development of future research. In addition, some publications in other languages, such as German and French, were not included in this study, which might have influenced the publication bias.
Conclusion
To summarize, miRNAs could be potential and promising biomarkers in distinguishing HB patients from healthy people. Together, these findings provide important evidence for the further development of future non-invasive methods for diagnosing HB. Further large-scale relevant studies with better designs and more comprehensive data support will help to clarify the diagnostic and prognostic value of miRNAs in HB.
Footnotes
Abbreviations
Authors’ Contributions
Chao Sun and Kaikai Zhen designed the study, analyzed the data, and drafted the manuscript. Bin Wu and Lixia Guo acquired patient data and performed laboratory experiments. Chao Sun contributed to the study design and manuscript writing. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Project of Suzhou Municipal Science and Technology Bureau (SYS 201764).