
Abstract
Introduction
It is reported that bladder cancer is the second most common malignant cancer in the genitourinary system. 1 Radical cystectomy (RC) is known as the standard treatment for muscle-invasive bladder cancer (MIBC). 2 However, this procedure is highly invasive and risky, and has a significant impact on the quality of life of the patients. 3 A combined modality therapy that maximizes the preservation of bladder function without compromising oncotherapy is an alternative that may be considered.
The Massachusetts General Hospital (MGH) experience 4 introduced a tri-modality therapy (TMT) with bladder preservation for selective MIBC patients, which shares a similar OS to RC patients. And a large number of studies reported that the bladder-sparing methods may produce favorable results in carefully selected patients from western society.5-7 However, there is still a lack of data to verify whether this treatment is suitable for patients from China. Our study summarized the clinical data of 125 patients with MIBC admitted to the First Affiliated Hospital of Soochow University between December 2012 and December 2015, 79 of whom received TMT and 46 of whom received RC, and they were followed up for more than 5 years to compare the effects of 2 kinds of treatments on overall survival (OS) and progress-free survival (PFS).
Materials and Methods
Clinical Data
This is a single-center, retrospective study. From December 2012 to December 2015, patients diagnosed with MIBC were enrolled at the First Affiliated Hospital of Soochow University. Inclusion criteria included pathologically confirmed MIBC and clinical stage T2-T4aN0M0. Exclusion criteria included a history of autoimmune disease or infectious disease. A total of 125 patients were candidates for this study, including 114 males and 11 females, with 79 cases receiving TMT and 46 cases receiving RC. The mean tumor diameter was (33.90 ± 2.61) mm and the average age was (69.66 ± 1.92) years. According to TNM staging of the Union Internationale Contre le Cancer in 2017, there were 91 cases defined as T2, 22 cases defined as T3, and 12 cases defined as T4a. The follow-up time ranged from 5 to 97 months, with an average of 51.36 ± 4.12 months. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Our research was approved by the ethics committee of the First Affiliated Hospital of Soochow University (approved ID: No. 119[2020]) and all the patients signed consent forms before the study.
Treatment Protocols
RC Group
All the patients underwent transurethral resection of bladder tumor (TURBT) first and the pathology was confirmed as MIBC. Meanwhile, preoperative chest, abdomen, and pelvic enhanced computed tomography (CT) or magnetic resonance imaging (MRI) confirmed no distant metastasis. At the same time, the Eastern Cooperative Oncology Group (ECOG) score was 0 to 2 points. Finally, RC and urinary diversion were performed after informed consent was signed with the family members.
TMT Group
All the patients first received TURBT and the pathology was proved as MIBC. No distant metastasis was confirmed by preoperative chest, abdomen, and pelvic enhanced CT or MRI. And the ECOG score was 0 to 2, with no contraindication found for radiotherapy (RT) or chemotherapy. After the informed consent was signed, the patients underwent complete TURBT (cTURBT), in which all the visible bladder tumors should be resected with random bladder biopsy and surgical wound base biopsy negative. Intravenous chemotherapy including gemcitabine 1000 mg/m2 (day 1 and day 8), cisplatin 70 mg/m2 (day 2) was performed within 2 to 4 weeks after the surgery, with a cycle of 3 weeks, a total of 3 cycles. Carboplatin was used to replace cisplatin when the creatinine clearance rate was 40 to 60 mL/min. RT of 24 to 25 Gy was received after chemotherapy.
Follow-up
All patients were reexamined every 3 months within 2 years, every 6 months within 2 to 5 years, and once a year after 5 years. The reexamination included a chest x-ray and abdominal and pelvis CT or MRI. For patients who received TMT, cystoscopy, and urine cytology should be taken every 3 months for 2 years, every 6 months for 5 years, and annually for at least 10 years.
Statistical Analysis
The quantitative data were expressed as mean ± standard deviation, and comparisons between 2 groups were determined using the Mann–Whitney U-test. The comparisons of cumulative data between the 2 groups were examined by χ2 test. Statistical analyses were performed using SPSS 22.0. GraphPad Prism 8.0 was used to draw survival curves. Kaplan–Meier and log-rank tests were used for survival analysis. Multiple linear regression analysis was used to find independent risk factors. And a p-value was considered statistically significant if p < .05. The sample size calculation was calculated by R software (version 4.1.0) and the number in our study to show significance was 103. 8 All the data was checked by 2 different senior statisticians.
Results
Baseline Levels Comparison Between 2 Groups
There was no significant difference found between the RC group and TMT group in age, gender, body mass index (BMI), high blood pressure (HBP), diabetes mellitus (DM), TNM staging, tumor diameter, preoperative creatinine levels, and prognostic nutritional index (PNI) (Table 1).
Comparisons of patients’ characteristics between the TMT group and the RC group.

Abbreviations: TMT, tri-modality therapy; RC, radical cystectomy; BMI, body mass index; HBP, high blood pressure; DM, diabetes mellitus; PNI, prognostic nutritional index.
OS and PFS in 2 Groups
The TMT group was followed up for 9 to 97 months, with an average of 47.84 ± 5.18 months, and the RC group was followed up for 5 to 90 months, with an average of 57.41 ± 6.69 months. There was no significant difference between the 2 groups in follow-up time (t = 2.253, p = .051). The 1-year, 2-year, 5-year, and comprehensive OS rate (94.94% vs 93.48%, 79.75% vs 89.13%, 32.91% vs 50.00%, 26.58% vs 19.57%, respectively) and PFS rate (74.68% vs 82.61%, 50.63% vs 65.22%, 33.75% vs 48.89%, 10.13% vs 17.39%, respectively) in TMT group and RC group showed no statistical significance (Table 2). And the survival analysis proved that patients who received TMT or RC shared a similar time of OS and PFS (Figure 1).

Survival curve of OS and PFS for TMT group and RC group. (A) Survival curve of OS showed that there was no significant difference between the TMT group and the RC group (t = 1.690, p = .091). (B) Survival curve of PFS also showed that there was no significant difference between the TMT group and the RC group (t = 1.867, p = .062).
Comparisons of OS and PFS between 2 groups.
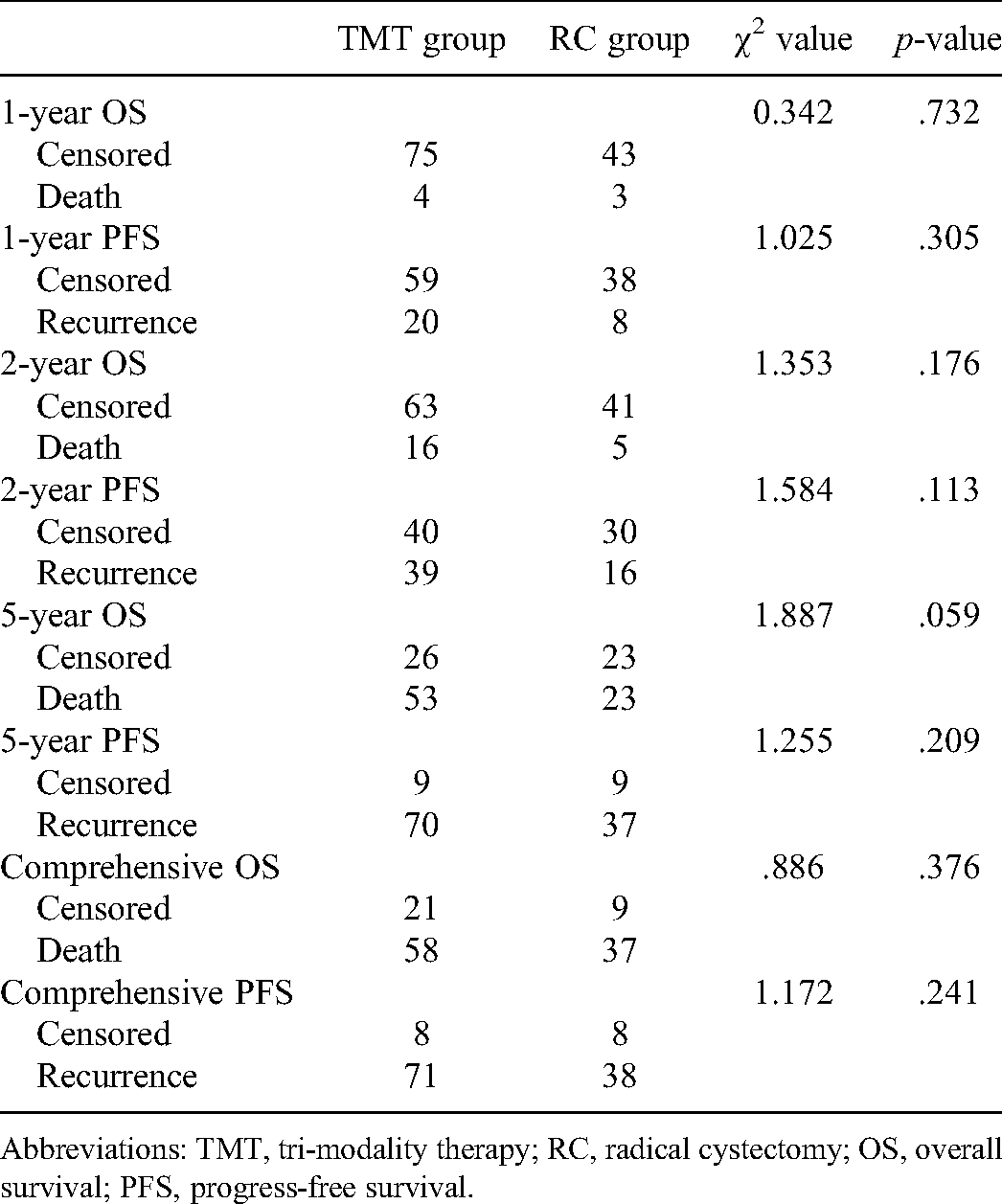
Abbreviations: TMT, tri-modality therapy; RC, radical cystectomy; OS, overall survival; PFS, progress-free survival.
Influencing Factors of OS and PFS
Univariate analysis demonstrated that age, TNM staging, and PNI were negatively associated with OS, while PNI was negatively connected to PFS (Table 3). Further multiple linear regression analysis found that TNM staging and PNI were independent risk factors for OS (Table 4). A receiver operating characteristic (ROC) curve was drawn and the area under curve (AUC) was 0.7675 (Figure 2).

ROC curve of the model for independent risk factors for OS with an AUC of 0.7675.
Univariate analysis of influencing factors of OS and PFS.

Abbreviations: BMI, body mass index; HBP, high blood pressure; DM, diabetes mellitus; PNI, prognostic nutritional index; OS, overall survival; PFS, progress-free survival.
Multiple linear regression analysis for independent risk factors of OS.

Abbreviations: OS, overall survival; PNI, prognostic nutritional index.
Discussion
Bladder cancer is 1 of the most common malignancies in urology. 1 Among the first diagnosed patients with bladder cancer, approximately 25% to 30% are MIBC. 9 The standard mode of treatment for MIBC is RC, which includes radical cystectomy, urinary diversion, and bilateral pelvic lymph node dissection. 4 For men, the prostate and seminal vesicle glands should be removed simultaneously, and for women, the uterus, bilateral adnexa, and part of the anterior wall of the vagina should be removed at the same time. It is reported that the 5-year PFS rate was 58% to 68%, and the 5-year OS rate was 66%. 10 However, due to the wide range of surgical resection, long operation time, and high incidence of complications, the quality of life of patients after surgery is greatly affected, young patients will lose fertility function, and most patients will lose sexual function, 3 many patients will finally give up the surgery.
James et al. 11 first reported that TURBT combined with postoperative chemotherapy, nearly one-third of patients benefitted from the degradation of TNM staging. Büchser et al. 2 conclude that the bladder preservation rate could reach up to 79% and the 5-year OS and PFS were 52% and 64% within 10 years under the strategy of TMT, which was made up of cTURBT and chemoradiotherapy. A prospective study also found that the complete response rate after TMT was 69% and the 5-year OS and PFS were 57% and 71%, and the outcomes were similar to that of RC. 4 Recently, more and more relevant studies have found that TURBT combined with postoperative chemoradiotherapy is another option for the treatment of MIBC.3,12-14 However, there are few reports on the effect of TMT strategy on the Chinese population.
Our study was aimed to compare the efficacy of TMT treatment with RC treatment in some Chinese populations. Despite the 1-year OS (94.94% vs 93.48%), TMT group had a lower rate than RC group in 2-year and 5-year OS (79.75% vs 89.13%, 32.91% vs 50.00%). But no statistical significance was found between the 2 groups. And although the 1-year, 2-year, and 5-year PFS rates of the TMT group were lower than that of the RC group (74.68% vs 82.61%, 50.63% vs 65.22%, 33.75% vs 48.89%, 10.13% vs 17.39%), there was still no significant difference between 2 groups. The survival curve of OS and PFS of the TMT group and RC group further verified that the 2 treatments were statistically equally effective for patients with MIBC of T2-T4aN0M0. Our research also found that PNI was negatively associated with OS and PFS in MIBC, which was consistent with the results of Peng et al. 15
We summarized the experience of our hospital in TMT strategy as follows: (1) cTURBT emphasizes the resection of all visible bladder tumors, and the resection depth should be appropriate to see the fat layer outside the bladder. And pathology of the basal tissue must be negative. (2) Platinum-based chemotherapeutic regimens are recognized as effective therapeutic measures for MIBC. If renal function is poor, it is recommended to change cisplatin to less nephrotoxic carboplatin. The main adverse reactions during chemotherapy included nausea and vomiting, alopecia, bone marrow suppression, and abnormal liver function, and no serious complications occurred in our study. The response rate of MIBC to RT is low, but Gemcitabine has a radiosensitization effect for patients who received low-dose external irradiation, which included bladder and pelvic lymph nodes. There were 4 patients who developed radiation cystitis, of which 2 patients disappeared after the end of RT after symptomatic treatment, and 1 patient developed urethral stricture requiring regular urethral dilation. (3) Bladder preservation requires close follow-up, and timely salvage cystectomy is recommended in the case of recurrent invasive tumor or recurrent nonmuscular invasive bladder cancer. There were 12 cases that underwent salvage RC after recurrence, which accounted for 15.19% of the TMT group. And among the 12 recurrent cases in the TMT group, 5 cases were diagnosed with pelvic metastasis.
There were some limitations reserved in this study. First, it is a retrospective study and conducted in a single-center, which may cause bias and misleading findings. Second, the limited number of patients may make the conclusions statistically underpowered. Third, the follow-up period is not very long compared to similar studies, which makes the results less convincing.
Conclusions
Based on the experience of our center, TMT strategy for MIBC with the T2-T4aN0M0 stage can help improve the quality of life while preserving the bladder, and also achieve a similar long-term OS and PFS to RC. Therefore, under the premise of strict control of indications, full informed consent before surgery, rigorous follow-up after surgery, and timely salvage cystectomy, the TMT strategy can be used as an alternative to RC for MIBC patients.
Footnotes
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accord with the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics committee of the First Affiliated Hospital of Soochow University (No. 119) and informed consent was taken from all individual participants.
Author Contributions
(I) Conception and design: Zhang Zhiyu and Zhang Jianglei; (II) administrative support: Jun Ouyang and Zhang Jianglei; (III) provision of study materials or patients: Zhang Zhiyu and Zhou Qi; (IV) collection and assembly of data: Zhang Zhiyu, Zhou Qi, and Song Zhen; (V) data analysis and interpretation: Zhang Zhiyu and Zhou Qi; (VI) manuscript writing: all authors; (VII) final approval of manuscript: all authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Suzhou Science and Technology Project (grant numbers SLC201906 and SYS2019053).