
Abstract
Approximately 25% to 30% of breast cancer patients will progress to distant metastasis, and the 5-year survival rate decreases to 25% in metastatic patients. The most common metastatic sites of breast cancer are bones, lungs, liver, and brain. 1 Patients with bone or lung metastasis have better survival rates when compared to patients with liver or brain metastasis. 2 Although systemic therapies have advanced, the prognosis for patients with breast cancer liver metastasis (BCLM) remains poor. Moreover, some research suggests that the median survival for untreated BCLM was no more than 6 months, while the median survival rates for patients after treatment did not exceed 15 months. 3 Untreated patients with BCLM have reported median survival of ∼3 to 6 months from diagnosis. 4 Although systemic treatment can prolong survival, the peak median survival reported for patients who responded to systemic therapy is only 15 months, and surviving longer than 5 years is exceptional with medical therapy alone.5,6 Furthermore, patients with diffuse metastases have different characteristics and prognoses compared to patients with oligometastasis, by an unlikely slow progression. 7 Systemic therapy is not frequently the appropriate treatment for patients with liver metastases, because the diffuse metastatic liver disease may cause severe impairments to liver function and endanger the patient. As a result, it is especially crucial for us to choose the appropriate treatment protocols early on.
Due to the extent and locations of diseases and physical conditions, surgical excision or tumor ablation strategies are often considered for patients with limited disease and favorable histology. Moreover, breast cancer diffuse liver metastases are almost not eligible for surgery. 8 Many types of breast cancer were sensitive to radiotherapy, which led to radiotherapy on breast cancer patients with diffuse liver metastasis. Low-dose radiation therapy administered to the whole-liver radiation therapy (WLRT) is not regularly used for patient palliation with massive liver metastases. 9
Despite the treatment opinion for BCLM being palliative, different local treatment modalities have been applied together with systemic treatment to improve the outcomes.
Because of the extensive liver involvement with cancer, borderline liver functions, and/or the presence of extra-hepatic metastases, many patients are not applicable for high-dose radiation.10,11 Furthermore, the risk of classic radiation-induced liver disease (RILD) was estimated to be 5% when the whole liver was treated with 30 Gy in 2 Gy per fraction. 11
Although WLRT was possibly effective in palliating symptoms related to liver metastases, it was only occasionally used because of dose tolerance limits of the liver with liver diffuse metastatic lesions. According to the relationship between the dose tolerance and the volume of irradiation for liver cancer, a larger volume of irradiation meant a lower dose tolerance. Compared with the WLRT, the volume of fractionated irradiation was reduced by semi-liver radiotherapy, the radiation response from normal liver cells could be further reduced, and protecting liver functionality was effective. Compared with stereotactic body radiation therapy (SBRT), the average dose of radiotherapy for semi-liver radiotherapy was relatively lower, late tissue damage was reduced. 12 However, until now, there have been no reports on radiotherapy for diffuse liver metastasis of breast cancer. Therefore, semi-liver radiotherapy has been creatively applied in our research. The preliminary results are summarized as follows.
Materials and Methods
Patient Characteristics (Table 1)
The present study of semi-hepatic alternate radiotherapy for breast cancer patients with diffuse liver metastasis was approved by the ethics committee of the Fifth Hospital of Wuhan (Wuhan, Hubei, China) (November 11, 2014) and was initiated after compliance with procedures in December 2015. Written informed consent was obtained from the patients for participating in the study.
General Data and Clinical Characteristics of the Cases in the 2 Groups (n).

Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase.
From December 2015 to January 2018, 68 cases of diffuse liver metastasis from breast cancer were treated by semi-liver alternating intensity-modulated radiotherapy (IMRT) in our department (all confirmed by percutaneous liver biopsy, pathology, or cytology). Liver function was compensatory in all cases. Sixty-eight patients recruited were first-line radiotherapy instead of standard chemotherapy, targeted therapy or hormonal treatment Eastern Cooperative Oncology Group performance status of the patients was 2 to 3 scores. The median age was 48 years (32-65 years). All of them had simultaneous metastasis of the left and right lobes of the liver with more than 4 lesions in each lobe. The Child-Pugh grade of liver function was A or B, and transaminase was normal or slightly elevated (transaminase < 100 units/L). The patients were divided into Group A (34 cases) and Group B (34 cases) by a random number table.
Semi-Hepatic Alternate Radiotherapy on Diffuse Liver Metastasis in Patients with Breast Cancer
Radiotherapy Equipment
An Elekta electron linear precise accelerator (configuration iView-GT portal imaging verification system, 40 pairs of electric MLC; Elekta AB [Publ], 2008, Stockholm, Sweden), Xinhua SL-11 simulator (Shandong Xinhua Medical Instrument Co., Ltd), Philips 64-slice spiral computed tomography scanner (Brilliance 64, Philips Medical Systems), Elekta Precise 3-dimensional (3D) treatment planning system (Elekta AB [Publ]), immobilization vacuum pad (Shanghai Gerui Co., Ltd) and an abdominal bandage (Hengshui Runde Medical Instrument Co., Ltd) were used in the present study.
Radiotherapy Treatment Protocol
The patients were randomly divided into 2 groups (n = 34): Group A and Group B. For the alternating semi-hepatic radiotherapy group (Group A), The livers from Group A were divided into first and second semi-livers based on the anatomical features of the liver, planning target volume 1 (PTV1), and PTV2, and treated with semi-hepatic alternate IMRT. The interval between the radiotherapy treatments for PTV1 and PTV2 semi-livers was 6 h to avoid radiation hot spots. The average radiotherapy dose to the first and second semi-livers were both 2 Gy/fraction, once a day, 5 times per week, treating the clinical tumor volume with a total dose of 30 Gy for 15 days. The total radiation therapy duration was 15 days.
For the semi-hepatic sequential radiotherapy group (Group B), The livers from Group B were divided into the first and second semi-livers and treated with semi-hepatic sequential radiotherapy. The first semi-liver was treated in the first stage of radiation therapy, and the average radiotherapy dose to the semi-liver was 2 Gy/fraction, once a day, 5 times per week, treating the PTV1 with a total dose of 30 Gy for 15 days. The second semi-liver was treated in the second stage of radiation therapy, and the average radiotherapy dose to the semi-liver was 2 Gy/fraction, once a day, 5 times per week, treating the PTV2 with a total dose of 30 Gy for 15 days. The total radiation therapy duration was 30 days.
Radiotherapy was performed with the Elekta electron linear accelerator and precise treatment planning system. The abdominal bandage was used to control breathing during radiotherapy to reduce tumor motion. Target volume delineation was performed by the same doctor and medical physicist for all patients. To perform palliative radiotherapy, an electronic image treatment verification system (Elekta AB [Publ]) was used to improve the precision. Based on the clinical target volume (CTV), the crown sagittal axis of the PTV was extended outwards by 3 mm and was extended outwards by 5 mm along the axis of the body. In total, 7 to 9 irradiation fields were designed, and 85% to 90% of the isodose curve covered the PTV. Protection was provided for the normal liver and adjacent organs (maximum dose of stomach ≤ 40 Gy, stomach V45 ≤ 15%, maximum dose of spinal cord ≤ 40 Gy, small intestine V50 ≤ 15%, bilateral kidneys V20 ≤ 30%, normal liver V30 < 50%) as much as possible, using the Elekta Precise 3D treatment planning system. During radiotherapy, the patients were treated with liver protection drugs reductive glutathione (1.2-2.4 g/day, intravenous drip, Shanghai Fudan Fuhua Pharmaceutical Co. Ltd) and magnesium isoglycyrrhizinate (0.1-0.3 g/day, intravenous drip, Chia Tai Tianqing Pharmaceutical Group Co. Ltd). Regular inspections of peripheral blood and liver function were conducted during the course of treatment.13–15
Follow up. Patients were monitored over the 2 to 3 months following treatment, and trimonthly thereafter. Regular blood tests, liver function tests, measurements of magnetic resonance imaging (MRI; Achieva 1.5T, Philips Medical Systems) of the liver were performed at every follow-up appointment. Treatment responses were evaluated by MRI every 3 months with the modified response evaluation criteria in solid tumors. The treatment responses were defined as complete response (CR) was defined as the disappearance of the target lesion; partial response (PR) was defined as at least 30% decrease in size of the target lesion; progression of disease (PD) was defined as at least a 20% increase in the size of the target lesion; and stable disease was defined as neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD.16,17 Adverse reactions to radiotherapy were evaluated according to the standard criteria of the American Radiation Therapy Oncology Group (RTOG). Survival was evaluated from the date treatment commenced. The follow-ups were completed in April 2019.
Statistical Analysis
SPSS 22.0 statistical software (SPSS, Inc.) was used for statistical analysis. Effective rates, survival rates, and the incidence of adverse reactions were analyzed using the chi-square test. The Kaplan–Meier method was used to estimate survival rates, and the log-rank test was used to compare differences in survival. A 2-sided P < .05 was considered to indicate a statistically significant difference.
Results
Dose comparisons of PTV and peripheral organs at risk between Group A and Group B are given in Table 2. Figures of dose distribution and dose–volume histogram of a patient were given (Figures 1 and 2). A figure of CTV and PTV delineation was given (Figure 3). There were no significant differences in average PTV1 and PTV2 doses between Group A and Group B. There were no significant differences in the maximum doses of gastric and cord and bilateral lung V20.

Dose distribution of a patient.

(A, B, C) Dose–volume histogram of a patient given.

CTV and PTV delineation of a patient.
Targeted and Organ-threatening Doses of Radiotherapy in the 2 Groups.

Abbreviations: PTV1, planning target volume 1; PTV2, planning target volume 2.
Short-Term Efficacy
In Group A, 2 patients failed to complete radiotherapy due to severe intolerable radiotherapy reactions, such as abdominal pain, nausea, and vomiting. In Group B, 1 patient failed to complete radiotherapy due to a fear of the side effects of radiotherapy. Treatment responses were evaluated by MRI every 3 months, using the modified response evaluation criteria in solid tumors. 16 The overall response rates of the 2 groups were equivalent (p = .903), but the total effective rate of Group A exhibited a tendency to improve when compared with Group B (see Table 3). One of the patients in Group A was found to have significantly reduced lesions after radiotherapy (see Figure 4A and B). One of the patients in Group B was found to have smaller lesions after radiotherapy (see Figure 4C and D).

Comparison of MRI before and after RT of 2 Patients with Diffuse Liver Metastasis of Breast Cancer in Group A and Group B. (A) MRI before RT of 1 patient with diffuse liver metastasis of breast cancer in Group A. (B) MRI after RT of 1 patient with diffuse liver metastasis of breast cancer in Group A. (C) MRI before RT of 1 patient with diffuse liver metastasis of breast cancer in Group B. (D) MRI after RT of 1 patient with diffuse liver metastasis of breast cancer in Group B.
Comparison of Short-term Efficacy between the 2 Patient Groups.

Abbreviations: CR, complete response; PR, partial response; SD, stable disease; PD, progression of disease; ORR, objective response rate.
Follow-up Survival Rates
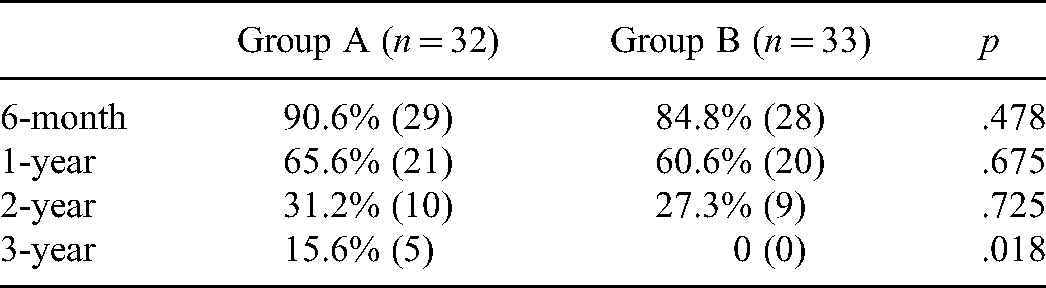
The follow-ups ended in January 2021. The median survival time for Group A was 16.7 months, compared with 16.2 months for those in Group B (see Figure 5). The median survival time for Group A was slightly longer than that of Group B, with no significant difference (p = .411). The 6-month, 1-year, 2-year, and 3-year overall survival rates of the 2 groups were similar (see Table 4) The differences in survival rates of the 2 groups at 6 months, 1 year, and 2 years were not statistically significant, however, 3 years were statistically significant. It could be related to the inadequate number of cases.
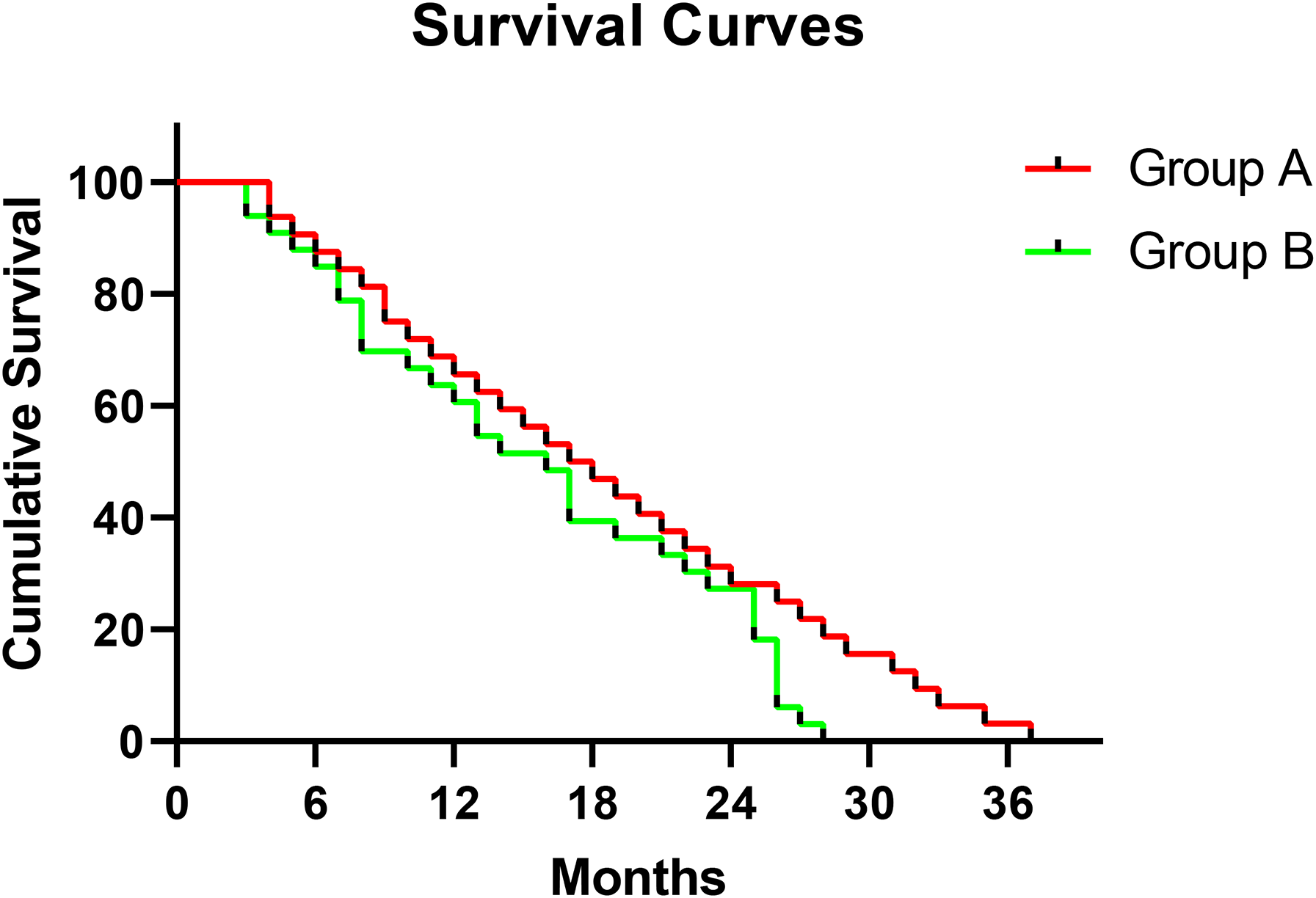
Survival curves of the 2 patients groups. Survival analysis using a Kaplan–Meier plotter. Comparison of overall survival of 2 techniques of semi-hepatic alternating radiotherapy on diffuse hepatic metastasis in patients with breast cancer (time [months]).
Comparison of the 6-Month, 1-Year, 2-Year, and 3-Year Overall Survival Rates of the 2 Groups.
Treatment Associated Toxicity
The criterion for evaluating toxicities was RTOG. The main toxic reactions during treatment were gastrointestinal reactions, abnormal liver functions, and myelosuppression. RILD usually occurs within 3 months after radiotherapy.18,19 The I to II degree gastrointestinal reactions, I to II degree abnormal liver functions, I to II degree myelosuppression, and radiation-induced liver diseases of the 2 groups were similar (see Table 5). RILD was diagnosed by an elevation of alkaline phosphatase level of ≥2-fold and/or elevated transaminases of ≥4-fold of the upper limit of normal levels.
Toxic and Side Effects of the 2 Patient Groups (% [case]).
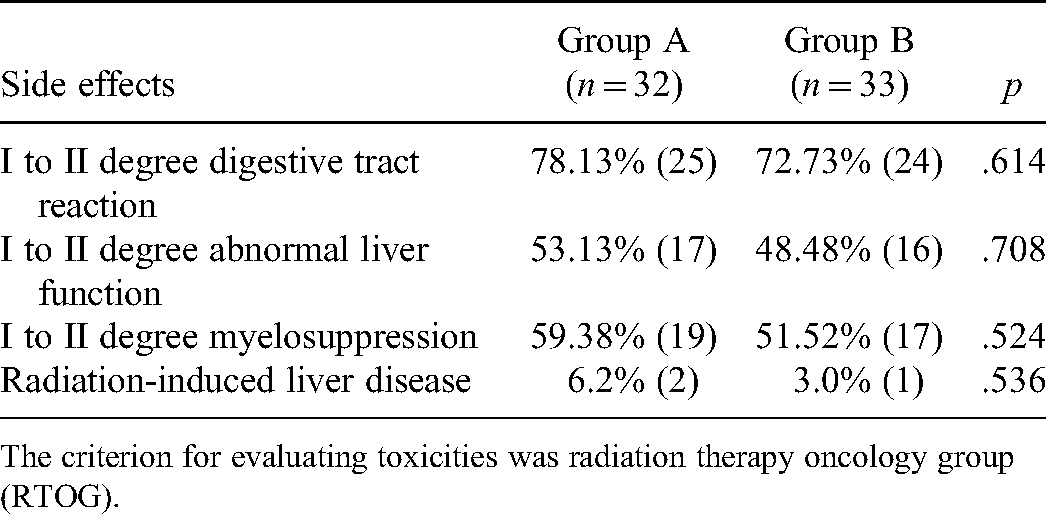
The criterion for evaluating toxicities was radiation therapy oncology group (RTOG).
Discussion
Current treatments for BCLM include systematic therapy, such as endocrine therapy, targeted therapy, chemotherapy, and local therapy, such as radioembolization, chemoembolization, microwave ablation, and stereotactic body radiotherapy.20,21 Despite comparing patients with primary versus metastatic liver cancers, the risk of developing nonclassic RILD differs considerably, as patients with primary liver cancers have a higher chance of having this toxicity after external beam radiation. 19 For patients with diffuse liver metastasis of advanced breast cancer with compensatory or decompensatory liver function, there was still more to explore for the therapeutic effects and toxicity of the radiotherapy. Diffuse BCLM was difficult to implement because of its scattered focus and no specific target area. The sublethal injuries were repaired during alternating irradiation intervals by dividing the liver into the first and second semi-livers for irradiation, so that the cells could proliferate again, thus increasing the tolerance of normal tissues to radiation. Alternate irradiation could also redistribute cancer cells in the alternating irradiation interval, which increased the sensitivity to subsequent radiation and increased the fatality rate of cancer cells. With better oxidation of the tumor margin, the death of radiation-sensitive cells, and the retraction of lesion masses, the blood supply to deep hypoxic cells was increased, and the hypoxic cells in the center of the lesion with an interval of alternate irradiation were reoxidized to increase radiosensitivity. 22
Until now, diffuse hepatic metastasis of breast cancer has been rarely reported by radiotherapy around the world. Although for diffuse metastatic hepatocellular carcinoma, both mobile strip radiotherapy and whole-liver field radiotherapy have been used all over the world, mobile strip technology was gradually abandoned because the equipment of radiotherapy had been greatly developed, the repeatability of daily irradiation was very poor, the dose distribution was very uneven. 23 Semi-liver intensity-modulated radiation therapy (IMRT) was creatively used to treat diffuse BCLM, expecting to prolong the survival time with few radiation responses. Group A and Group B were both administered with semi-liver radiotherapy. In this study, the radiotherapy targets were divided into 2 areas: the first and second semi-livers. When one-half of the liver was irradiated, the other half of the liver was not, so that normal liver metabolism could be maintained. Most of the sublethal injuries were repaired within 6 h after a radiotherapy session concluded, and the dose intensity in the radiation field could be adjusted by intensity-modulated radiotherapy technology according to needs, which could maximize high-dose irradiation of targets, reducing the doses to at-risk organs around the radiation field, and the occurrences of radiation-induced liver injuries. Shortening the total treatment time will increase tumor death, and generally aggravate the injuries of early response tissues. So, early response tissue damage in Group A was greater than in Group B. Compared with SBRT, the average dose of radiotherapy of semi-liver alternating IMRT was relatively lower, and late-reaction tissue damage was reduced. Compared with Group B, the biologically effective dose of tumors in Group A was higher, the tumors were more difficult to repair, and they were more prone to apoptosis.
The total irradiation time was 15 days in Group A and 30 days in Group B. The total irradiation time in Group A was half of that in Group B. Because of the different total irradiation times, the biological effect doses of the 2 groups were different, and the equivalent biological effect doses in Group A were larger than that in Group B. For RILD, there was no significant difference between Group A and Group B, but there seemed to be a decreasing trend in Group B were compared with Group A. Despite there being no significant differences in short-term efficacies between Group A and Group B, the total effective rate of Group A presented an upward trend, when compared with Group B. Despite there being no significant difference between Group A and Group B, the median survival time of Group A was slightly longer than that of Group B, and there was a trend of prolongation. Although the equivalent biological effect doses of Group A and Group B were different, the differences between curative effects were not significant. The reason could be related to the advanced stages of the 2 groups, insensitivity to treatment, and small sample size. Despite no significant differences in adverse reactions between Group A and Group B, the adverse reactions in Group B had a declining trend when compared with Group A.
To summarize, semi-liver IMRT was an effective palliative treatment for diffuse liver metastasis of breast cancer. Semi-liver alternating IMRT could prolong the survival time of diffuse liver cancer of breast cancer. Semi-liver alternating IMRT showed a prolonged trend in survival when compared with half-liver sequential IMRT. Compared with the former, the latter tended to see a decrease in side effects, and the therapy could be well tolerated. However, due to the small number of cases, it is necessary to expand the sample sizes in further studies. The emergence of modern radiotherapy techniques has helped to minimize the toxic side effects from radiation to the liver, and ongoing studies will help refine the clinical indications for radiation treatment for patients with liver tumors. 19 However, given the limited sample size and retrospective nature of this study, further studies are needed to elucidate the optimal dose-fractionation schemes for treating such patients.
Supplemental Material
sj-docx-1-tct-10.1177_15330338211051808 - Supplemental material for Clinical Study of 2 Radiotherapy Techniques for Semi-Hepatic Alternating Radiotherapy on Diffuse Liver Metastasis in Patients with Breast Cancer
Supplemental material, sj-docx-1-tct-10.1177_15330338211051808 for Clinical Study of 2 Radiotherapy Techniques for Semi-Hepatic Alternating Radiotherapy on Diffuse Liver Metastasis in Patients with Breast Cancer by Jiangzhou Zhang, Shuheng Bai, Xingzhou Zhang, Yanli Yan, Haojing Kang, Guangzu Li, Zhaode Feng, Wen Ma, Hong Sun and Juan Ren in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-2-tct-10.1177_15330338211051808 - Supplemental material for Clinical Study of 2 Radiotherapy Techniques for Semi-Hepatic Alternating Radiotherapy on Diffuse Liver Metastasis in Patients with Breast Cancer
Supplemental material, sj-docx-2-tct-10.1177_15330338211051808 for Clinical Study of 2 Radiotherapy Techniques for Semi-Hepatic Alternating Radiotherapy on Diffuse Liver Metastasis in Patients with Breast Cancer by Jiangzhou Zhang, Shuheng Bai, Xingzhou Zhang, Yanli Yan, Haojing Kang, Guangzu Li, Zhaode Feng, Wen Ma, Hong Sun and Juan Ren in Technology in Cancer Research & Treatment
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.