
Abstract
Introduction
Microcalcifications within the breast are present in approximately 30% of malignant lesions and masses, and they are important indicators of early breast cancer.1,2 Microcalcifications expressing calcifications smaller than 1 mm in diameter can be detected utilizing digital breast tomosynthesis (DBT) mammography modality with a resolution of less than 100 μm. 1 DBT, which is an advanced form of x-ray mammography evolved by Gershon-Cohen, Leborgne, and others, is one modality being developed to detect lesions, masses, and microcalcifications in a breast.3–7 Analytical and iterative algorithms have been used for reconstructing three-dimensional (3D) images slice by slice to detect distortions, masses, lesions, and microcalcifications in each slice in DBT. Iterative algorithms such as the algebraic reconstruction technique (ART) introduced by 8 and the simultaneous ART (SART) introduced by 9 have been used as new alternative methods for analytical image reconstruction techniques such as filtered back projection (FBP) which was first advanced by Bracewell and Riddle 10 and later independently by Ramachandran and Lakshminarayanan 11 to reconstruct 3D images of a breast. 12 Shepp and Logan demonstrated the superiority of FBP over algebraic reconstruction methods in 1974. 13 However, FBP requires a full scan of the target to provide a better image, while algebraic reconstruction methods do not. For example, with SART, a 3D image of the breast can be created with only a few projections, usually ranging from 9 to 25, 5 obtained from a limited viewing angle scan of the breast that causes incomplete data.5,14 FBP algorithm is based on the inverse Radon transform, 15 while the SART algorithm yields a solution discretizing the Radon transform for a linear algebraic system iteratively. 16 Due to the FBP requires complete projection data, the results of reconstruction provide less accuracy because of using incomplete projection data in DBT. Compared with the FBP, the main advantage of SART is that it is opportune to apply to incomplete and noisy projections in DBT.16–21
A large No. of projections are required for the FBP to provide a successful image reconstruction in DBT. However, as a high No. of projections will cause high doses of radiation and this carries the risk of cancer even in a healthy breast, it becomes necessary to view with a limited No. of projections. SART provides a considerable superior over FBP in terms of high-quality image reconstruction using a few No. of projections taken in a narrow angle range. Regardless of the image reconstruction method, comprehensive analyses of the proposed method should be performed in a simulation environment before applying it in clinical DBT in terms of cost, duration, and radiation risk. Some software tools such as the open-source DBT reconstruction toolbox developed at Laboratory of Computer Vision (LAVI), Research group at University of São Paulo (USP),22,23 open virtual clinical trials (OpenVCT),24–26 and The All Scale Tomographic Reconstruction Antwerp (ASTRA) toolbox generated by the collaboration of Antwerp University, Belgium, and the Centrum Wiskunde Informatica, Amsterdam, The Netherlands27,28 have been introduced for 3D image reconstructions in medical imaging such as tomography and DBT. ASTRA offers reconstruction ability for tomographic applications such as computed tomography (CT) and electron tomography, while open-source DBT reconstruction toolbox by LAVI (we will henceforth refer to as the LAVI) provides a software environment that mimics a realistic implementation of clinical DBT. LAVI offers several reconstruction methods such as FBP, SART, simultaneous iterative reconstruction technique (SIRT), and maximum likelihood expectation maximization (MLEM).
On the other hand, recently, several open-source software packages such as XDesign, 29 TomoPy, 30 syris, 31 and TomoPhantom 32 have been released that provide the generation of the analytical phantoms mainly based on application to x-ray-based image reconstructions. TomoPhantom, which was written in the C-OpenMP language providing wrappers for Python and MATLAB supports 2D objects, including circles, ellipses, rectangles, and parabolas and enables computationally efficient generation of 2D-4D high-resolution phantoms. In literature, there are a few existing studies about digital breast phantoms. These studies have some limitations such as computation time cost (2 h 32 min) 33 and applying only FBP as a reconstruction method. 34
In this paper, we present a realistic breast phantom mimicking the main structures of a real breast including nodules, milk ducts, lesions, masses, and microcalcifications using the TomoPhantom software package for testing and benchmark studies in DBT. The proposed phantom enables a variety of dimensions with 64 × 64 × 64 (643), 128 × 128 × 128 (1283), 256 × 256 × 256 (2563), and 512 × 512 × 512 (5123) which can be used to rigorously evaluate image reconstruction algorithms. Another advantage of this phantom is computational efficiency compared to other digital breast phantoms. The creating time of our proposed realistic breast phantom was a maximum of 8 min for maximum dimension of 5123. We also performed various reconstruction methods such as FBP and SART (with 1-2-4-8 iterations). To validate the characterization of our proposed realistic breast phantom, we tested the visibility of the structures and especially the distinguishability of the microcalcifications that mimic cancerous cells in the breast using the reconstruction tool of LAVI.
Materials and Methods
Traditionally, the FBP algorithm, which performs a filtering operation on the projections before backprojection using a ramp filter as a high-pass filter and the Hann filter as a windowing technique, is used for DBT reconstruction.26,34 FBP uses the mathematical fundamentals of Radon transform and Fourier transform, 15 on the other hand, SART is based on solving a linear algebraic equation system. These reconstruction algorithms are generally tested on the simplistic numerical phantoms, which do not appropriate for DBT imaging applications. The aim of this study is (1) to introduce a realistic breast phantom that is computationally efficient and (2) to validate that the phantom mimics the real breast characterization by applying FBP and SART. Details of the phantom design and SART are explained in the next subsection.
Realistic Breast Phantom Design
Breast phantoms are numerical or physical models of the breast developed to evaluate and improve the image quality of breast imaging systems. Simulation environments are of undeniable importance for the development and testing of 3D image reconstruction methods used in clinical DBT applied by giving radiation to patients. TomoPhantom includes various geometric objects such as ellipses, cuboids, rectangles, and volumetric extensions of them. This software allows producing complex phantoms using geometric shapes and their combinations. 32
In our realistic breast phantom design, we created the many anatomical structures and combinations of them adapting some geometrical objects offered by TomoPhantom software to mimic complex breast anatomy. TomoPhantom software creates the objects by defining the unitless parameter of user inputs such as the x-y-z positions (range in [−1, 1]), diameters (range in [0, 2]), and rotation angles (range in [0, 180]) in 3 axes and intensity values (range in [0, 1]). The basic object name, eg, ellipsoid, cuboid, and phantom dimension, eg, 64-512 are also defined in the software by the user. Therefore, our realistic breast phantom was generated unitless dimension-based. The objects selected to create the complex breast phantom and their name of structure and number of objects are given in Table 1, and the basic versions of them are shown in Figure 1. Many structures mimicking the main parts of real breast anatomy including the nipple, milk ducts, lobules (glandular tissue), ribs, and chest wall were created in the phantom via TomoPhantom software. Due to the incapability of very small size object generation via TomoPhantom, the microcalcifications with one-pixel size in the breast were generated using a separate MATLAB code. The phantoms of different sizes ranging from 643 to 5123 were created and microcalcifications were embedded in the central slice of the phantom as 4 groups of 4 each, eg, in the
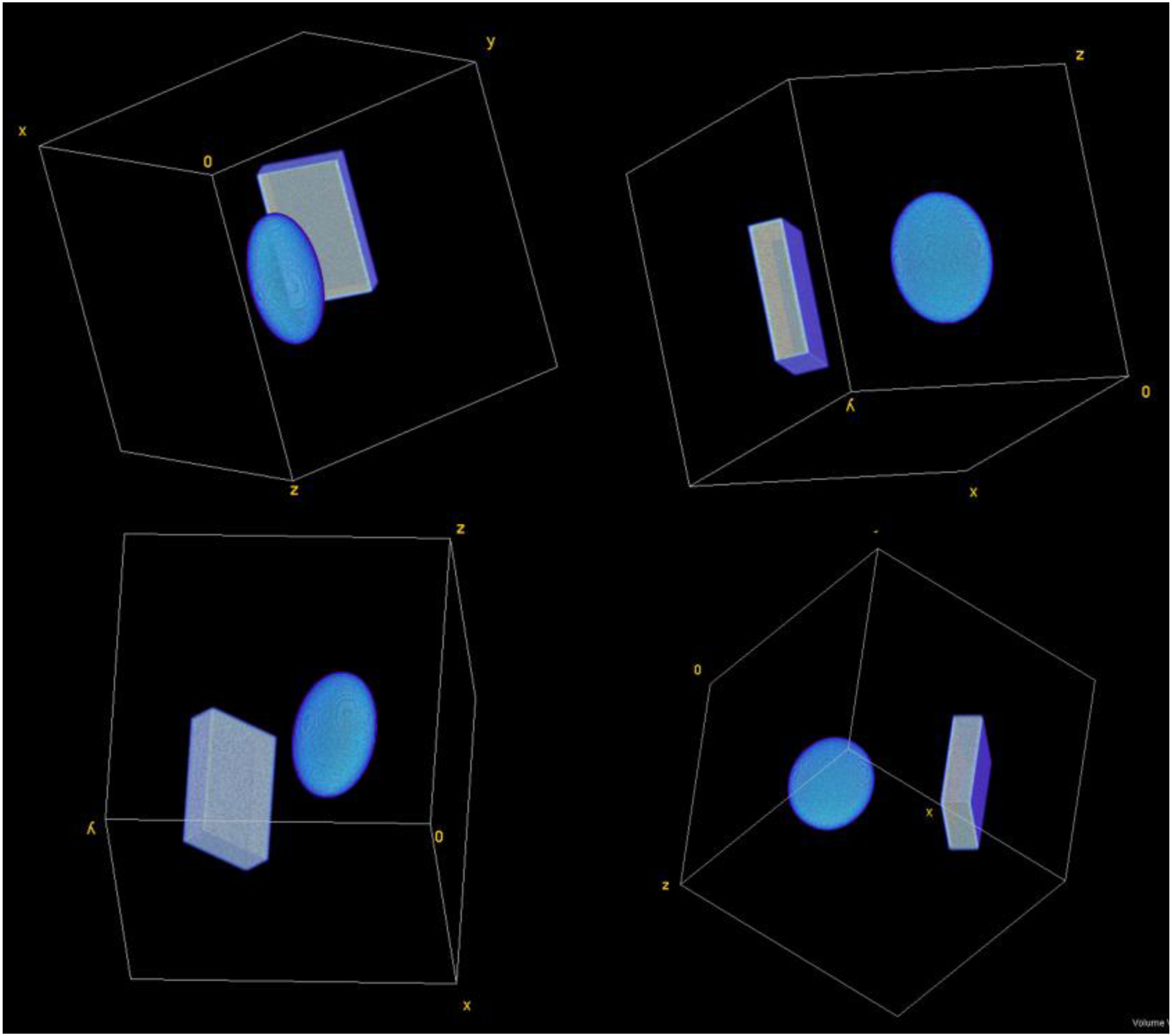
The various perspectives of the visualization of the three-dimensional (3D) volume of basic objects (eg cuboid and ellipsoid) used in the realistic breast phantom design.
The description of realistic breast phantom.

Simultaneous Algebraic Reconstruction Technique (SART)
The SART, which can capture great details of the objects with only a few projections, has been widely used in medical image reconstructions after introducing by Anderson and Kak in 1984.
9
SART is a superior implementation of the ART introduced by Kaczmarz in 1937,
8
which focuses on finding a solution iteratively to a linear algebraic problem. The imaging system of the DBT can be modeled as a formulation in equation (1) which is an ill-posed linear inverse problem.

Finally, we compared the outputs of the reconstructed images by FBP and SART quantitatively and qualitatively. We enlarged the views of embedded microcalcifications to increase the visibility in the original phantom in Figure 2. For qualitative analysis, after reconstructions, we checked the visibility of microcalcifications comparing the images of the original layer of interest (LOI), FBP, and SART (Figures 3 and 4), respectively. For quantitative analysis, we utilized the metrics; the contrast-to-noise ratio (CNR) (see equation (3)),39,40 full width half maximum (FWHM), and 1D profile. FWHM is defined as 

The visualization of the three-dimensional (3D) volume of breast for the dimensions of 643, 1283, 2563, and 5123; the enlarged views of microcalcifications.

The comparison of the original layer of interest (LOI) (128th slice) (a), the reconstructions of LOI via filtered back projection (FBP) (b), and simultaneous algebraic reconstruction technique (SART) (1 iteration) (c) for 11 projections. (a) The description of region of interest (ROI), background of ROI, full width half maximum (FWHM) line, and 1D profile line.
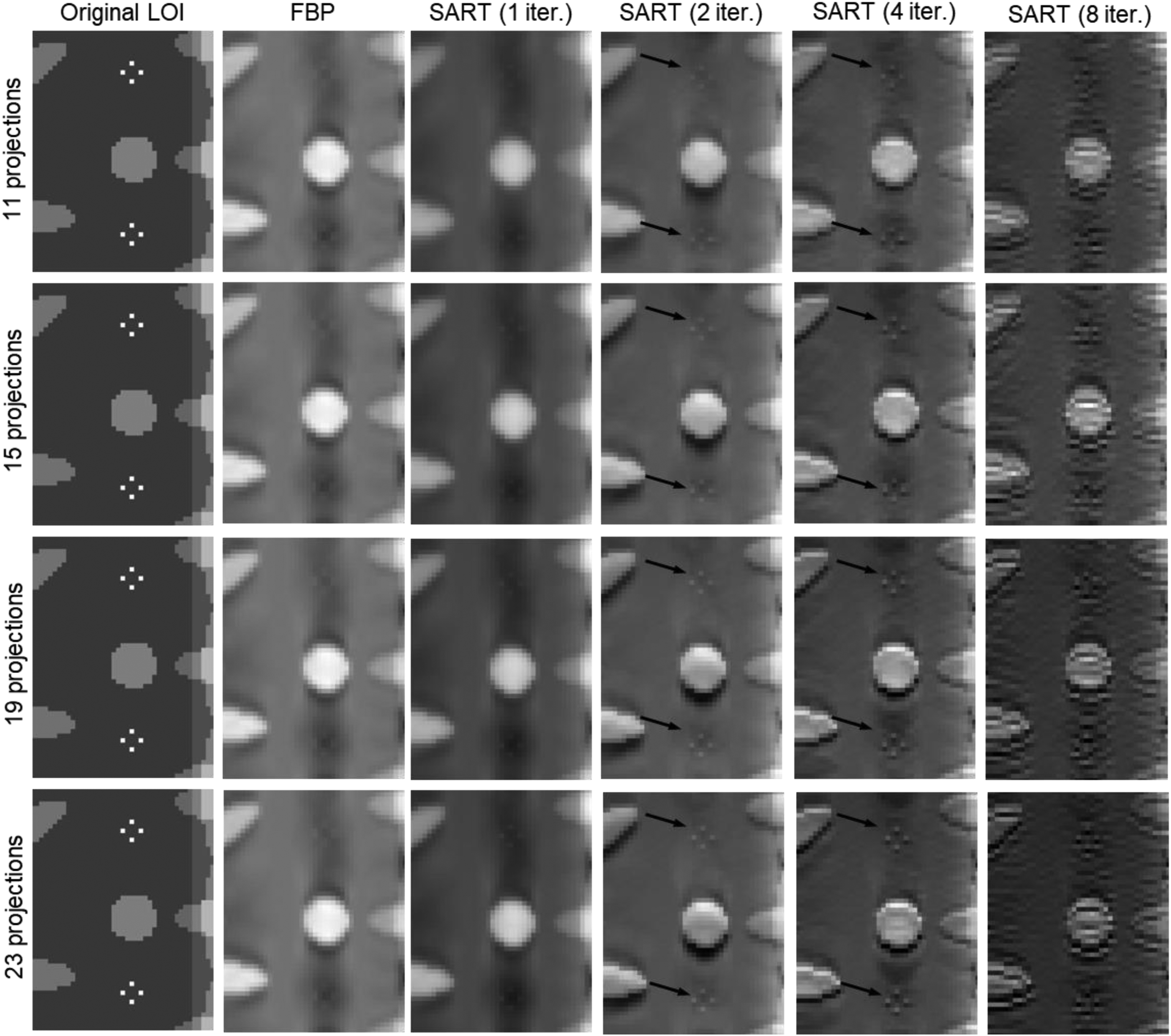
The comparison of enlarged views of regions of interest (ROIs) of the reconstructed images via filtered back projection (FBP) and simultaneous algebraic reconstruction technique (SART) (1-2-4-8 iterations) for 11, 15, 19, and 23 projections.
In equation (3),
Results
The realistic breast phantom that ranges from 643 to 5123 in dimensions including the anatomical structures and microcalcifications was created successfully and made eligible for reconstruction. The visualization of a 3D volume of realistic breast phantom with sizes 643, 1283, 2563, and 5123 in various styles, and the enlarged views of microcalcifications (4 × 4 set) are given in Figure 2. The ratio of glandular/adipose tissue of the phantom was calculated as 3.4765%. The creating times of our proposed realistic breast phantom for 643, 1283, 2563, and 5123 were 2.5916 s, 8.4626 s, 57.6858 s, and 472.1734 s, respectively. These computation times were performed with a workstation that has 11th Gen Intel(R) Core(TM) i9-11900H @ 2.50 GHz, 16 cores, 32 GB RAM, and 16 GB NVIDIA GeForce RTX 3080. The reconstructed images of the 2563 size phantom as 256 slices in the longitudinal axis were obtained by FBP and SART modules of LAVI and compared qualitatively and quantitatively. The center slice, 128th layer, of the phantom that includes the microcalcifications was chosen as the LOI. The comparisons of the original LOI, the reconstructed LOI via FBP, and the reconstructed LOI via SART are given in Figure 3(a), (b), and (c), respectively. The iteration number of SART was 1 and the projection numbers of both FBP and SART were 11.
In Figure 3, for qualitative analysis, we focused on the top set of 4-microcalcification and enlarged a frame at 2 levels with the 1000% magnification ratio. For quantitative analysis, we determined the 4-microcalcifications as the ROI and surrounding them in the frame as the background to calculate the CNR values of the LOI of the original, FBP, and SART. Additionally, we defined an FWHM line to its element below the 4-microcalcification group and a 1D profile line that intersects the middle-left and -right members of the group. To evaluate qualitatively, as a result of FBP and SART (1 iteration) obtained with 11 projections, microcalcifications could be reconstructed. However, to analyze which method is better quantitatively, reconstruction results applied with the increased number of projections and iterations is discussed below. We presented the enlarged views of the top 2 groups of 4-microcalcification set for original LOI, FBP, SART (1 iter.), SART (2 iter.), SART (4 iter.), and SART (8 iter.) for 11, 15, 19, and 23 projections in Figure 4. In the quantitative assessment in Figure 5, we demonstrated the comparison of the CNR values for all reconstruction methods with the determined iteration and projection numbers. We also presented the more quantitative analysis of reconstructed images applying the FWHM metric in Figure 6 and applying the 1D profile metric in Figure 7, respectively.

The comparison of the contrast-to-noise ratio (CNR) values of the regions of interest (ROIs) of the reconstructed images via filtered back projection (FBP) and simultaneous algebraic reconstruction technique (SART) (1-2-4-8 iterations) for 11, 15, 19, and 23 projections.

The comparison of the full width half maximum (FWHM) of the reconstructed images via filtered back projection (FBP) and simultaneous algebraic reconstruction technique (SART) (1-2-4-8 iterations) for 11, 15, 19, and 23 projections.

The comparison of the 1D profiles of the reconstructed images via filtered back projection (FBP) and simultaneous algebraic reconstruction technique (SART) (1-2-4-8 iterations) for 11, 15, 19, and 23 projections.
Discussions
The meticulousness of the phantom design was that the microcalcifications were very small compared to the size of the breast as they really are hidden in only 1 layer and they can be captured with FBP and SART. The generation time of the realistic phantom, which is less than 8 min for 5123, is pretty feasible to examine the different reconstruction algorithms easily and quickly. This provides an opportunity for various revisions on the realistic breast phantom. The phantom has some limitations such as the inability to express dimensions in metrics and the lack of real x-ray attenuation values of breast tissue.
According to the comparison of the reconstructed images, SART (2 iter.) and SART (4 iter.) yields the best visibility of the microcalcifications (pointed with black arrows on the images) for all numbers of the projections. It is clear that increasing the number of the iteration to 8 in SART causes distortion of the images. The reconstructed images by FBP and SART (1 iter.) yield very close results in the manner of visibility of the microcalcifications, but they are not as clear as the reconstructed images by SART (2,4 iter.) (Figure 4). These qualitative evaluations are also supported by the values of the CNR, which is the first metric used for quantitative analysis. The CNR values of SART (2 iter.) and SART (4 iter.) are very close to each other and they are also much higher than the CNR values of FBP, SART (1 iter.), and SART (8 iter.). Besides, when the CNR graph is examined, it is very clear that increasing the number of projections increases the CNR values as expected. For example, while CNR values of SART (2 iter.) for 11 and 23 projections were calculated, respectively,
The value of FWHM of original LOI was
In Figure 7, when the 1D-profile tendency is examined, the closest behavior to the original LOI profile behavior (black solid line) was shown by the reconstructed images obtained with 19 (red) and 23 (green) projections SART (2 iter.) (dash line) and SART (4 iter.) (solid line). Considering the results of FWHM, 1D profile, and CNR metric in general, SART (2), and SART (4) methods with 11 and 15 projections also provided images with acceptable quality. According to the overall qualitative and quantitative evaluation of the reconstructed images obtained from all methods applied with all projections, FBP and SART (1 iter.) captured the microcalcifications slightly, while SART (8 iter.) gave completely distorted results. On the other hand, for all projections, SART (2 iter.) and SART (4 iter.) were able to successfully capture microcalcifications with significant results.
Conclusions
In this study, we created and proposed a realistic breast phantom that mimics the structures in a real breast such as the nipple, lobules, ribs, milk ducts, chest wall, and also includes the microcalcifications. We tested the performance of iterative (SART) and analytical (FBP) image reconstruction methods with various parameters such as the number of projections (11-23) and iterations (1-8 for SART) applying to this realistic breast phantom. In this way, it was possible to analyze the effects of the selection of reconstruction methods before clinical applications of DBT and to control its parameters. We proved that a computationally efficient realistic breast phantom can be used for pretest purposes in DBT in terms of establishing the basis for clinical applications. In future work, with the development of the phantom that has more sophisticated breast tissue modeling and applying the appropriate parameters of reconstruction in the clinic, overdose radiation of patients will be prevented.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Türkiye Bilimsel ve Teknolojik Araştirma Kurumu (grant number 119E388).