
Abstract
Introduction
Sleeve lobectomy is a frequently used operation for central lung cancer or tracheal/bronchial tumor treatment. It allows for complete tumor resection, maximized preservation of residual pulmonary function, and improvement of life quality, especially for those who cannot tolerate pneumonectomy due to poor cardiopulmonary function.1–3 However, sleeve lobectomy using minimally invasive surgery is still challenging.
With the development of endoscopic technology and artificial intelligence, robotic-assisted surgery (RAS) systems have been utilized for sleeve lobectomies.4,5 Although their results are encouraging, a longer learning curve, lack of tactile feedback to the operator, and tricky bronchial anastomosis RAS techniques are all associated issues that remain unresolved.6–8 Some current studies have pointed out that visual compensation may be a better alternative to the tactile feedback once the surgeon is proficient.8,9 Therefore, we created a new modified approach to RA sleeve lobectomy optimization in order to improve surgical field visualization and simplify anastomosis techniques. The study retrospectively reviewed and analyzed the clinical data for sleeve lobectomy using the optimized RAS and mini-thoracotomy (MT), especially focusing on the efficacy, safety, and postoperative outcomes.
Patients and Methods
Patients
The retrospective study included 26 consecutive patients between January 2017 and April 2020. The cohort included 11 cases (10 males, one female, mean age, 54.82 ± 9.21 years) of sleeve lobectomy using RAS (RAS group) and 15 cases (13 males, two females, mean age, 56.53 ± 8.25 years) of sleeve lobectomy using MT (MT group). Systemic examinations including enhanced chest computed tomography (CT), head magnetic resonance imaging (MRI), abdominal B-ultrasound, whole-body bone scan (or positron emission tomography [PET]-CT), fiberoptic bronchoscopy, electrocardiogram, and pulmonary, hepatic, and renal function evaluations were administrated for all patients prior to surgery. All patients who agreed to participate in the study signed an informed consent form. This retrospective study was approved by the Ethics Committee of Army Medical Center of PLA (Daping Hospital, Chongqing City, P.R. China) on September 26, 2019 [IRB: 2019 to 081].
Inclusion criteria included the following: (i) central lung tumors that have moved to the lobar bronchus; (ii) sufficient bronchus for anastomosis; (iii) no invasion of blood vessels; (iv) no obvious calcification in hilar and mediastinal lymph nodes; (v) relatively abnormal physical function of the heart, lung, liver, and kidney; and (vi) no other absolute contraindications.
Exclusion criteria were as follows: (i) invasion of multiple lobes requiring pneumonectomy; and (ii) invasion of blood vessels or obvious calcification in hilar and mediastinal lymph nodes.
Surgical Methods
(1) Anesthesia, position, and port approaches
The patient was positioned in the lateral decubitus position after general endotracheal anesthesia was induced using a double-lumen tube to facilitate lung isolation.
In the RAS group (Da Vinci Si Robot Surgical System [Intuitive Surgical, Sunnyvale, CA, USA], our exclusive optimized “3-4-6-8/9” four-port technique was performed according to a previously published method. 10 Lap protectors of the same size were placed in all incisions prior to port insertion as follows [Figure 1a]: [i] the assistant port was located at the fourth intercostal space at ∼4 cm outward from the midclavicular line; [ii] the 1-cm camera port was inserted at the sixth intercostal space in the posterior axillary line; and [iii] the 0.5-cm da Vinci ports for instrument arms were placed at the third intercostal space in the anterior axillary line and the eighth or ninth intercostal space in the posterior axillary line. The patient cart entered from the back of the patient's head and shoulders at 75° to the longitudinal line. The assistant was located at the ventral side of the patient in order to install the endoscope and instruments for linkage [docking process; Figure 1a].

Right upper sleeve lobectomy using RAS (surgical processes prior to anastomosis)
In the MT group, the seventh intercostal space in the midaxillary line was selected as the endoscope port (1 cm), and the lateral incision (15-20 cm) was performed over the fourth intercostal space in the inframammary groove.
(2) The surgical steps and suture methods for RAS and MT were similar. For the lobectomy using RAS: (i) the inferior pulmonary ligament and mediastinal pleura were dissected; (ii) the pulmonary vessels were divided and exposed; (iii) the hilar and mediastinal lymph nodes were removed; (iv) the main and all lobar bronchi were exposed and the tumors and invaded bronchus and lung parenchyma were removed (Figure 2); (v) end-to-end anastomosis using continuous 3 to 0 Prolene sutures was performed after negative bronchus stump biopsy results were confirmed; and (vi) figure-of-8 (F8) suture and a surgeon's knot were made at the midpoints of posterior walls of both bronchial ends. The two ends of Prolene suture were used to make continuous sutures posterior to lateral and anterior walls with a bulldog clamp holding the other stitch end to avoid twisting. The final surgeon's knot was made on the anterior walls of the bronchial ends to complete the anastomosis (Figure 3); and (vi) in case of air leakage, the interrupted sutures using Vicryl 3.0 were introduced with an absorbable polyglycolic acid sheet (NEOVEIL, GUNZE limited, Japan) coating the anastomosis.

Right upper sleeve lobectomy using RAS (anastomosis processes)

Evaluation of postoperative bronchius protrusion via chest CT (three months after RA sleeve lobectomy).
Retrieving Clinical Data
Retrieved demographical and clinical data included operation time, anastomosis time, intraoperative blood loss, chest drainage time and volume, postoperative pain scores (Visual Analogue Scale), 11 complications, and white blood cell (WBC) levels on days 1, 3, and 7 after the operation and hospital stay.
Follow-up
All of the patients underwent a routine outpatient or telephone follow-up every three months after the operation. Physical and systemic examinations, including chest CT, brain MRI, abdominal B-ultrasonography, and bone scintigraphy or PET-CT as an alternative, were administrated to monitor recurrence or metastasis.
Chest CT was used for evaluating bronchial angulation. Representative CT in anastomotic stoma showing a protrusion arising from the posterior wall or bronchial kinking while other was straight. 12
Statistical Analysis
All data analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corporation, Armonk, NY, USA) and GraphPad Prism software (GraphPad Software, Inc., San Diego, CA, USA). Measurement data were expressed as means and standard deviation (x̅ ± s) in cases of normal distribution. Otherwise, a median (range) was used. The X2 test or one-way analysis of variance was used for comparison between groups. Count data were expressed as cases or percentage, and Pearson's chi-square test was used for comparison between groups. A two-sided p < 0.05 was considered statistically significant. The statistical powers were calculated using XLSTAT (Addinsoft Inc., New York, NY, USA).
Results
There was no significant difference in sex, age, smoking status, underlying disease, tumor location, tumor size, pathological type, and TNM stage between the two groups (Table 1).
Clinical demographical characteristics of RAS and MT groups
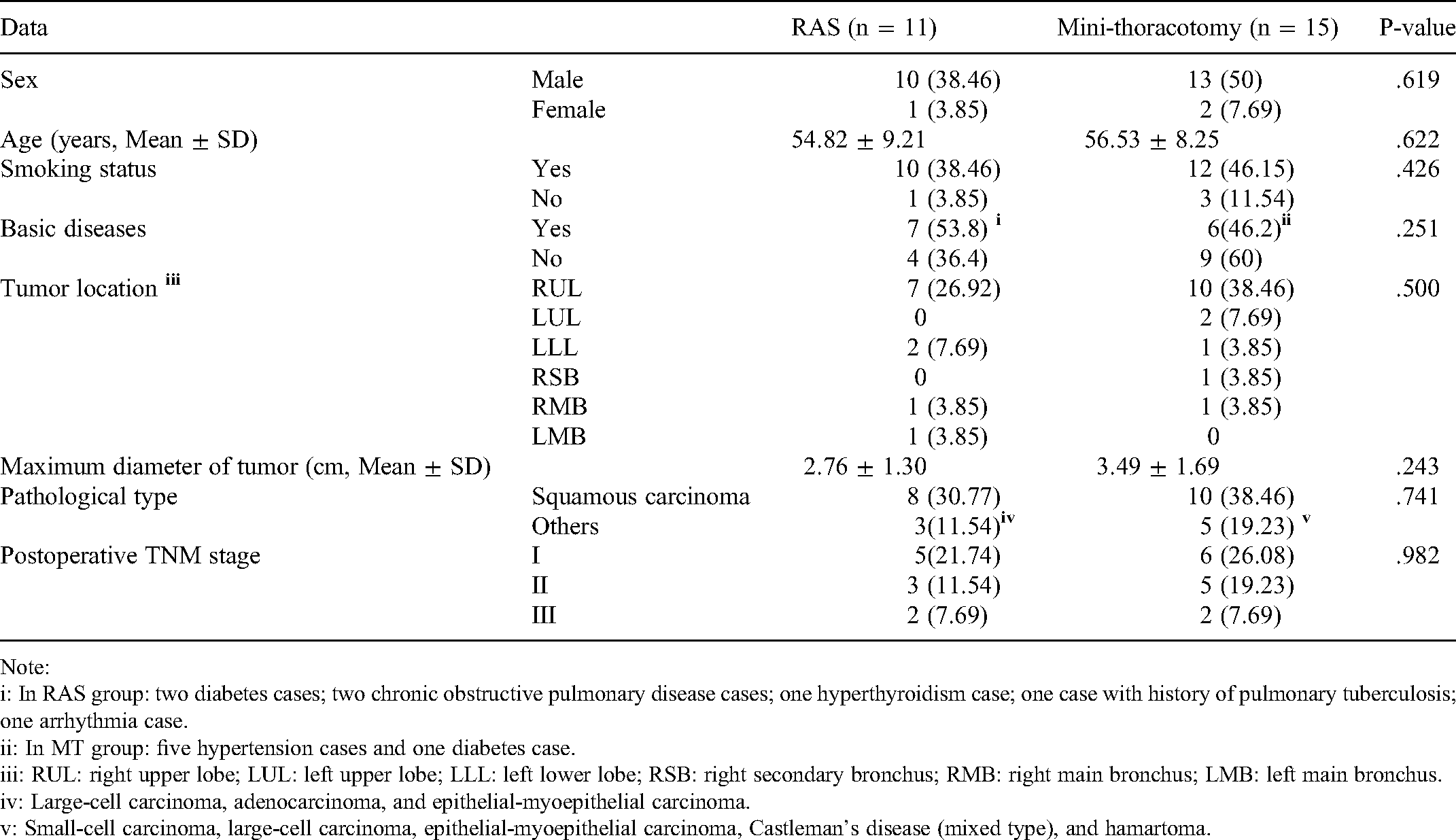
Note:
i: In RAS group: two diabetes cases; two chronic obstructive pulmonary disease cases; one hyperthyroidism case; one case with history of pulmonary tuberculosis; one arrhythmia case.
ii: In MT group: five hypertension cases and one diabetes case.
iii: RUL: right upper lobe; LUL: left upper lobe; LLL: left lower lobe; RSB: right secondary bronchus; RMB: right main bronchus; LMB: left main bronchus.
iv: Large-cell carcinoma, adenocarcinoma, and epithelial-myoepithelial carcinoma.
v: Small-cell carcinoma, large-cell carcinoma, epithelial-myoepithelial carcinoma, Castleman's disease (mixed type), and hamartoma.
RAS Group had Similar Anastomosis Time but Shorter Operation Time
There were no cases of perioperative death. All of the cases underwent an end-to-end bronchial anastomosis procedure, which took approximately half an hour in the RAS and MT groups (30.82 ± 6.08 vs 33.20 ± 7.73 min, p > 0.05). However, the operation time in the RAS group was 30 min shorter compared to the MT group (189.73 ± 36.41 vs 225.33 ± 38.19 min, respectively, p < 0.05). This was probably due to more convenient manipulation and shorter time needed to open and close the chest cavity. Intriguingly, the docking did not significantly increase the operation time in the RAS group because it only took 6.64 ± 2.91 min compared to our approach. Furthermore, there were no significant disparities in blood loss and number of resected lymph nodes (Table 2).
Comparison of clinical outcomes between RAS and MT groups

Note: statistical powers: i: .752; ii: .989; iii: 0.842; iv: .936
RAS Group had Lower Pain Scores and WBC Levels and no Anastomotic Complications Following Operation
Postoperatively, there were two and three cases with complications in the RAS and MT groups, respectively (2/11 vs 3/15, p > 0.05). However, stratified analysis indicated that anastomotic complications were more likely to occur in the MT group, which included one anastomotic stenosis and two bronchopleural fistulas. Intriguingly, the RAS group had one incident of prolonged air leakage and one case of chylothorax without any anastomotic complications.
Moreover, the postoperative pain scores in the RAS group were 4.23 ± 0.26, which is statistically significantly lower than those in the MT group (4.23 ± 0.26 vs 4.91 ± 0.51, p < 0.05).
The two groups had similar results for postoperative drainage time, total thoracic drainage volume, and postoperative hospital stay (Table 2).
WBC levels in both groups increased on the first postoperative day (Table 2). However, the RAS group patients had lower WBC levels on the third and seventh day after operation compared to the MT group (Table 2), demonstrating a lower inflammatory response caused by RAS.
Both Groups Demonstrated Successful Bronchus Reconstruction with low Risk of Angulation and Satisfactory Short-Term Outcomes
Bronchial angulation can be clearly identified using a chest CT after three months following the operation (Figure 3). Fortunately, the incidence of bronchial angulation was low in both groups (1/11 vs 1/15, p > 0.05). To date, the follow-up times in the RAS and MT groups have been similar (32.27.30 ± 17.65 vs 33.93 ± 13.92 months, p = 0.922). In the RAS group, one (3.85%) and two (7.70%) patients suffered from metastasis of mediastinal lymph nodes and distal metastasis, respectively. One patient (3.85%) died from chemotherapy side effects. In the MT group, two patients (7.69%) experienced anastomotic recurrence and another two patients (7.69%) had intracranial metastasis. Two patients (7.69%) died from anastomotic recurrence and chemotherapy side effects. The K-M plotter did not show any statistical differences in disease-free survival of the two groups (Figure 4).

Kaplan–Meier curve showing that cases in two groups had no significant differences and present satisfactory short-term outcomes.
Discussion
In 1947, Thomas et al. reported the first sleeve lobectomy 13 that can achieve the same effect as pneumonectomy and retain a maximum pulmonary function.1,14 With the developments of a variety instruments and techniques, thoracic surgeons began to perform video-assisted minimally invasive sleeve lobectomy in 2002. 15 Sleeve lobectomy via video-assisted thoracoscopic surgery (VATS) has the advantages of less trauma, less bleeding, less postoperative pain, and better quality of life.2,16–21 Thus, the National Comprehensive Cancer Network guidelines recommend this technique as a standard operation for lung cancer treatment.22,23
Currently, RAS represents a feasible and reliable alternative to this complex surgery. For instance, the da Vinci surgery provides a realistic three-dimensional stereoscopic image that can amplify the surgical field of view 10 to 40 times. Furthermore, the robotic instruments make the manipulations of pulling, rotating, clipping, cutting, suturing, and knotting more flexible and accurate. All of these advantages are supposed to facilitate sleeve lobectomy in a narrow space.4,7,24,25 However, there are some barriers to effective RAS, which include slower post-surgery recovery, increased set-up time, and higher cost. 26 RAS shows a promise in reducing the operation time for treating large and complex lesions when compared to the VATS approach, when an effective RAS team is involved in. 26 Furthermore, when assessing hospital stay cost exclusive of initial purchase cost, RAS has been found to be cheaper than open thoracotomy. 26
In 2006, Ishikawa et al. 27 performed the first “hybrid” surgery in a freshly frozen human cadaver using VATS to separate and dissect vessels and using RAS to perform bronchus anastomosis. They located three ports for RAS, including a 5-cm-long in the fourth intercostal space and a 0.5-cm-long in the third intercostal space on the anterioraxillary line and in the sixth intercostal space on the midaxillary line. In 2007, Schmid et al. reported a right upper sleeve lobectomy on a 30-year-old female patient using a similar “hybrid” surgery. 28 Subsequently, more experience has been accumulated and reported on sleeve lobectomies achieved using only RAS, which demonstrated feasibility and safety.4,29–31
Thus far, Jiao et al. 32 reported the largest series of 67 patients with sleeve lobectomy using RAS. They demonstrated their experience with three 1.5-cm port incisions and one 3-cm utility incision (the sixth intercostal space on the posterior axillary primarily for the robotic camera, the 4rd intercostal space on the anterioraxillary line, the seventh intercostal space on the scapularis line for arms, and the sixth intercostal space on the midaxillary line for the assisted port). However, the study curve seemed to be relatively long with ∼100 sleeve lobectomies using thoracotomy or VATS and 30 cases using RAS as the study cohort before stably entering the plateau phase. Furthermore, the robotic system was brought into the operating field and situated over the patient's head, which potentially affects anesthesia management during the operation.
Scheinerman et al. 5 reported another series of 23 patients receiving sleeve lobectomy using RAS with minimal morbidity and without short-term mortality. They designed and used four robotic ports and one assistant port. Pan et al. 33 reported a series of 21 cases of sleeve lobectomy using RAS via similar approaches. However, one patient suffered from an anastomosis fistula and subsequent pneumonia and died of multiple organ failure. Thus, some controversies remain regarding robotic arm and camera use. Moreover, RAS anastomotic techniques need to be optimized.32–37
Sleeve lobectomy using RAS has been carried out in our institution since 2017. With the accumulation of clinical cases and surgical experience, we modified the sleeve lobectomy using RAS approaches to reduce the port number and simplify the anastomotic techniques. The comparative analysis showed that intraoperative blood loss, postoperative complications, chest drainage time, and hospital stay are similar to those of the MT group, demonstrating safety, efficiency, and feasibility. Moreover, both operation time and postoperative pain scores are significantly superior to those of the MT group.
Anastomotic complications and bronchial angulation after sleeve lobectomy are a common and expected postoperative change, leading to atelectasis, pneumonia, dyspnea, and even complete collapse of the residual lung.12,38 Our study demonstrated no anastomotic complications even at the early stage of the learning curve, which was in accordance with the published studies focusing on sleeve lobectomy using RAS. (1) In a cohort of 67 cases, there were two cases of prolonged air leaks, one of bronchial stenosis, one of pneumonia, one of chylothorax, and one of cough-variant asthma, but no anastomotic complications. 32 (2) In a cohort of 23 cases, there was one case of pneumonia and one of transfusion, but no anastomotic complications. 5 (3) In a cohort of 21 cases, there were two cases of pneumonia, two cases of pyothorax, and only one of anastomotic leak. 33 All of the studies with small sample sizes demonstrated that the incidence of anastomotic complications when using RAS was promisingly low.
In this study, the RAS group had one case of prolonged air leakage and one case of chylothorax, which delayed chest tube removal and caused a longer hospital stay. Furthermore, the sample size was relatively small. Therefore, there are no statistical advantages for postoperative rehabilitation between the two groups. However, it is possible that the RAS group may exhibit rapid rehabilitation in a large cohort study.
Postoperative detection of WBCs has been demonstrated to be an indicator that predicts complications, such as infection or anastomotic leakage. 39 Theoretically, it is supposed to be conducive to evaluation of an inflammatory reaction following sleeve lobectomy. In the present study, the RAS group had lower WBC levels after operation compared to those of the MT group.
We believe that these encouraging outcomes are attributed to the following novel attributes of our technique:
Less docking time (2-10 min, mean: 6 min) compared to traditional RA technique (17 ± 10 min)9,33 because the camera can directly and conveniently guide the instrument arms via the ports to avoid repeating cannula adjustments; The surgical field of view is similar to that of VATS, thus shortening the learning curve and operation time for the surgical team with VATS experience. The process of running 3 to 0 Prolene suture with bulldog clamps holding the other suture end can smooth and simplify the anastomosis and avoid suture twisting. In addition, a nerve hook can be used to pull and tighten sutures; The needle distance and margin should be adjusted and matched appropriately to reduce stress and avoid tearing of bronchial walls; Additional reinforced suture is unnecessary unless there is air leakage confirmed by the intraoperative water testing.
Moreover, anastomosis is critical in sleeve lobectomy. The techniques include multiple interrupted sutures using absorbable VICRYL, running 3 to 0 Prolene suture, or a combination of both.4,8,40 All of the bronchial anastomoses in the present study were made using continuous running suture with 3 to 0 Prolene. Notes on our experiences using this method are as follows:
We also acknowledge the limitations of the study, which include a small sample size and the lack of survival evaluation due to limited follow-up time. However, the present pilot study demonstrates the strengths of the optimized RAS in comparison with MT. In addition, our results underscore the importance of adopting minimally invasive surgery for this type of operation.
Conclusion
The optimized approach for RA sleeve lobectomy is convenient and efficient and provides satisfactory clinical outcomes that include shorter operation time, lower incidence of anastomotic complication, and lower pain scores. Further study with a large sample size and evaluation of long-term survival are warranted.
Ethics Approval and Patient Consent Statement
This retrospective study was approved by the Research Ethics Board in Daping hospital (Chongqing City, P.R. China) [IRB: 2021 to 014]. However, it was not a prospective trial, consent to participate was not required.
Footnotes
Acknowledgments
This study is supported by the joint project of Science and Technology Committee and Health Commission of Chong-qing(No. 2020FYYX061) and the Natural Science Foundation of Chongqing City (No. cstc2015jcyjA10073, No. cstc2019jscx-msxmX0252)
Conflict of Interests Statement
Tao Shaolin, Feng Yonggeng, Kang Poming, Mei Longyong, Shen Cheng, Fang Chunshu, Wu Licheng, Deng Bo and Tan Qunyou have no conflicts of interest or financial ties to disclose.
Funding
The authors declare no competing financial and non-financial interests in relation to the work described in the manuscript.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Code Availability
All data, models, and code generated or used during the study appear in the submitted article.
Author Contribution Statement
Shao-Lin Tao and Yong-Geng Feng performed the operations, reviewed the clinical data and write the manuscript.Mei Longyong, Fang Chunshu and Wu Licheng reviewed the clinical and pathological data.Kang Poming and Shen Cheng designed the clinical treatment strategies. Deng Bo and Tan Qunyou designed the surgical strategies, supervised the whole project and proofread the manuscript.
Consent to Participate
Written informed consent for publication was obtained from all participants.
Consent for Publication
Written informed consent for publication was obtained from all participants.