
Abstract
Keywords
Introduction
Colorectal cancer (CRC) is still a deadly disease in many countries, including China,1,2 and there is a decreasing trend in the age of patients who die from CRC. 3 To date, the majority of metastatic cases of CRC, except for a small cluster featuring high microsatellite instability (MSI) that respond well to immunotherapy, 4 are poorly controlled and patients have poor survival rates. The search for biomarkers that guide not only patient selection for certain therapeutic regimens but can also be used for prognostic prediction is increasingly important.
Previously, a group of biomarkers collected from hematoxylin and eosin (HE) staining slides, including tumor budding (TB), tumor stroma ratio (TSR, also referred to as tumor stroma proportion), and tumor infiltrating pattern (TIP, also referred to as tumor growth pattern), were reported to be useful prognostic indicators in many malignant diseases, including gastric cancer,5–7 breast cancer,8,9 lung cancer, 10 and CRC.11–14 TB is defined as “a single tumor cell or a cell cluster consisting of 4 tumor cells or less” 15 and has been reported to be closely correlated with disease recurrence and poor patient prognosis in CRC.12,16–18 In addition, TSR has also been found to be a predictor of local tumor growth and invasion,13,19 and TIP has been found to be associated with disease recurrence in CRC.14,20 It is notable that TB, TSR, and TIP are morphological parameters that were collected from HE slides. It is plausible that these parameters are innately connected, and that their individual prognostic potency is not identical; however, few related studies have been conducted.
It is well recognized that systematic inflammatory markers, including the neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR), are simple and reliable prognostic indicators in many malignant diseases, such as head and neck cancer, 21 gastric cancer, 22 pancreatic cancer, 23 breast cancer, 24 and CRC.25–28 In particular, the LMR has been proven to be superior for predicting prognosis than other markers, including the NLR, in CRC. 29 Notably, several studies have suggested that TB, TSR, and TIP are associated with cancer-related inflammation; 30 nonetheless, the underlying correlations among TB, TSR, TIP, and LMR have never been reported.
In this study, we aimed to explore the correlation among these markers and determine their individual prognostic potency in CRC.
Methods
Patient Enrollments
From January 2011 to October 2016, patients who underwent colectomy either laparotomy or laparoscopic surgery were enrolled at the Hainan Hospital of Chinese PLA General Hospital. Patients who met the following criteria were included: 1. age ≥ 18 years old; 2. no neoadjuvant therapies; and 3. radical excision of the primary tumor. The exclusion criteria were as follows: 1. age <18 years old; 2. complications requiring glucocorticoids or other immunosuppressors; 3. any neoadjuvant therapies; 4. absence of laboratory tests within a week before surgery or key information loss in postoperative pathological reports; 5. multiple or recurrent malignancies, in situ lesions; and 6. lost to follow-up or follow-up period was less than 36 m. Clinicopathological parameters were collected as previously described. 31 The study was approved by the ethics committee of the Hainan Hospital of the PLA General Hospital (approved ID: 301HLFYLS15), and written informed consent was obtained from the patients or his/her authorized relatives.
Determination of TB, TSR, and TIP and Definition of Subgroups
Surgical tissue samples were immediately processed by standard pathological procedures in the Department of Pathology as previously described, 32 and 5-μm HE-stained sections were analyzed by conventional microscopy (DM3000, Leica). In brief, the slides were first observed under a 20 × objective lens to determine the most invasive front (areas with mucinosity, necrosis or breakage were excluded). TB was defined as “an isolated cancer cell or a cluster composed of fewer than 5 cancer cells” 33 and was determined according to the recommendations for reporting TB in CRC in the ITBCC 2016. 15 At least 10 individual fields were identified as the “hotspot,” and the final results were divided into low (<5 buds and 5-9 buds) and high (≥10 buds) subgroups as previously reported. 34 For TSR, after selecting target areas in the same manner as for TB, areas were chosen where both tumor (present at all borders of the image field) and stromal tissue were visible under a 10 × objective and patients were classified into TSR low (≤50%) or high (>50%) subgroups.19,35 For TIP, the definitions of expansile (the invasive margin was pushing or well circumscribed), intermediate (large- to medium-sized glands presented and the border was not clear) and infiltrative (cancer cells invaded in a diffuse pattern with extensive penetration of normal tissue, often with no legible margin) were determined in selected target areas, determined in the same manner as performed for TB,7,36 and patients were divided into TIPa (expansile + intermediate) and TIPb (infiltrative) subgroups as in previous studies.7,36 All the parameters were read by 2 independent senior pathologists who were blinded to the clinical information of the cohort.
Calculating for LMR
Routine laboratory tests were performed between 6:00 and 9:00 am by peripheral venous blood collection within 1 week before surgery. The LMR was calculated as previously reported. 37
Definition of Relapse-Free Survival (RFS) and Overall Survival (OS) Intervals
Follow-up was performed by telephone, WeChat or visit as per the hospital medical records at intervals of 3 to 6 months for the first 3 years and 6 to 12 months for the subsequent 3 years. The RFS interval was defined as the time between the date of surgery and the date of the first recurrence at any location, disease progression identified by imaging or death from any cause. The OS interval was defined from the date of surgery until the date of death from any cause. The latest follow-up date was in June 2020.
Statistical Analysis
All statistical analyses were conducted by using SPSS 20.0 (SPSS Inc.). A receiver operating characteristic (ROC) curve analysis was used to determine the optimal discriminator value for LMR. The areas under the curve (AUCs) were compared by MedCalc v19.0.7 (MedCalc Software Ltd). The differences in clinicopathological parameters among low or high TB/TSR/LMR and TIPa or TIPb subgroups were calculated by χ2-test or Fisher's exact test or Student's t where appropriate. The associations among these markers were determined by Spearman's correlation analysis, Kaplan–Meier (K-M) survival curves were applied to compare patients in different subgroups, and significance was determined by log-rank tests. Univariate and multivariate analyses were conducted by using the Cox proportional hazards model. A two-sided P < .05 was considered statistically significant.
Results
Demographic Characteristics and the Differences in Clinicopathological Parameters Among TB, TIP, and LMR Subgroups
In total, 147 colorectal adenocarcinoma patients staged I to IV (according to the seventh edition of the AJCC) were enrolled (Figure 1). There were 57 female and 90 male patients, and the mean age of the patients was 59.87 years (range: 24-85 years) with a medium follow-up time of 48.81 m (range: 1.00-91.00 m). In the ROC analysis, both TB and TIP, but not TSR (Figure 2), were useful for predicting survival (Figure 3A), and the LMR had a sensitivity of 50.00% and specificity of 79.40% at the cutoff point of 3.15 (Figure 3B). However, subsequent comparison of the AUCs for TB, TIP, and LMR displayed no significant differences (P > .05). Patients with a poor histological grade and large tumor diameter were more likely to present with high TB and TIPb and low LMR; in addition, those with advanced T, N, and TNM stages as well as elevated CA199 displayed high TB and TIPb (Table 1).
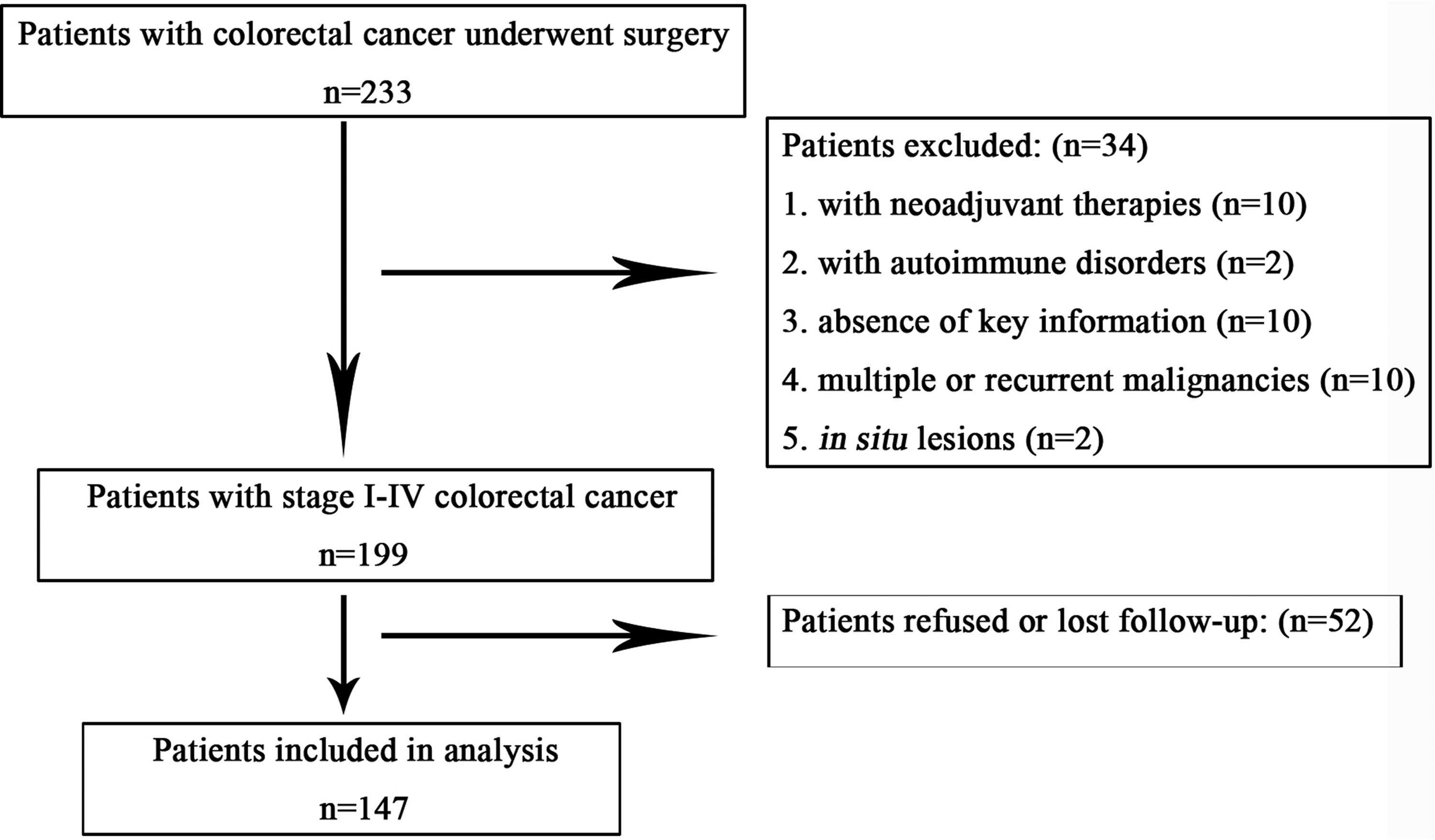
Flow diagram of the study.

H&E staining to evaluate TB, TSR, TIP: (A) low TB; (B) high TB (black arrows indicate typical buddings); (C) low TSR; (D) high TSR; (A-D with magnification × 200); (E) TIP expansile growth pattern; (F) TIP intermediate growth pattern; (G) TIP infiltrating growth pattern (E-G with magnification × 100).

Receiver operating characteristic curve analysis of TB, TIP (A) and LMR (B) in patients.
Differences of TB, TIP, and LMR Among Different Clinicopathological Parameters.

Abbreviations: TB, tumor budding; TSR, tumor stroma ratio; TIP, tumor infiltrating pattern; LMR, lymphocyte-to-monocyte ratio; BMI, body mass index; No., number of the patients.
Correlation among TB, TSR, TIP, and LMR
Spearman correlation analyses of TB, TSR, TIP, and LMR indicated no significant correlations among TB, TSR, and LMR, and only TB and TIP showed statistically significant correlations (r = .63, P < .01). Patients with low TB (82.14%) were more commonly found to have TIPa; whereas those with high TB (80.95%) more commonly had TIPb, as revealed by further analysis.
Predictive Value of TB, TIP, and LMR for Survival Outcomes
In the K-M analyses, patients with high TB or TIPb had significantly worse RFS (TB low vs high: 49.92 ± 20.30 m vs 38.19 ± 24.98 m, P < .01; TIP a vs b: 50.83 ± 18.88 m vs 37.61 ± 25.71 m, P < .01) and OS (TB low vs high: 52.90 ± 18.54 m vs 43.33 ± 22.05 m, P < .01; TIP a vs b: 52.80 ± 16.63 m vs 43.89 ± 23.84 m, P < .01) outcomes than those of patients with low TB or TIPa; in contrast, patients with high LMR had significantly poorer RFS (low vs high: 33.11 ± 24.45 m vs 50.26 ± 20.40 m, P < .01) and OS (low vs 39.17 ± 21.65 m vs 19.11 ± 24.45 m, P < .01) outcomes (Figure 4).

Impact of low or high TB; TIPa or TIPb; and LMR on RFS and OS outcomes in patients.
Univariate and Multivariate Analyses of the Prognostic Factors for RFS and OS Outcomes
Univariate tests revealed that TB, TIP, and LMR were significant prognostic factors for RFS (Table 2) and OS outcomes (Table 3); multivariate tests revealed that TB and LMR were independent prognostic factors for RFS outcomes (Table 2), but only LMR was an independent factor for the OS outcome (Table 3).
Univariate and Multivariate Analyses of Different Parameters for RFS.

Abbreviations: TB, tumor budding; TSR, tumor stroma ratio; TIP, tumor infiltrating pattern; LMR, lymphocyte-to-monocyte ratio; RFS, relapse-free survival; BMI, body mass index; HR, hazard ratio.
Univariate and multivariate analyses of different parameters for OS.

Abbreviations: TB, tumor budding; TSR, tumor stroma ratio; TIP, tumor infiltrating pattern; LMR, lymphocyte-to-monocyte ratio; RFS, relapse-free survival; BMI, body mass index; HR, hazard ratio; OS, overall survival.
Discussion
In the present study, we found that TB, TIP, and LMR, but not TSR, were useful markers for predicting the survival outcomes of CRC patients. Patients with a poor histological grade and large tumor diameter are likely to present with high TB and TIPb and low LMR. In addition, although both TB and LMR were independent prognostic factors for RFS outcomes, the LMR was the only independent factor for OS outcomes among these markers.
Previously, TB, TSR, and TIP were reported to be important prognostic factors in CRC. Oh et al 18 conducted a study including 4196 staged I to III patients and found that high TB was associated with several adverse clinicopathological parameters, such as advanced stages and poor histological grade, as well as inferior disease-free survival (DFS) and OS outcomes. Similarly, Nagata et al 12 conducted a study of 371 stage IV patients and found that those with a high TB had poor OS outcomes. In addition, TIP has also been reported to a robust indicator of local or distant recurrence14,20 and of OS outcomes (confined to stage I-III patients) in CRC patients. 36 Our results regarding TB and TIP were in line with those of these reports.12,18,36 In addition, the TSR has been found to be an important prognostic marker in CRC, but with conflicting results; for example, Mesker et al.'s 35 study revealed that DFS and OS outcomes in patients with a high TSR were remarkably superior, but other reports yielded opposite conclusions.13,19,38 Nonetheless, the TSR failed to predict survival outcomes in our study, even though we excluded stage IV patients according to the recommendations in previous reports.13,19,35,38 We speculate that these findings may be attributable to the relatively low proportion of high TSR levels in our study cohort (11.56%) compared to that reported by others (70.8%, 13 73.00%, 35 and 70.51% 39 ).
Notably, TB, TSR, and TIP are potentially correlated with each other and related to the stroma. For example, a several studies have indicated that TB is associated with TIP, 40 and both TB and TIP have been suggested to be related to TSR.13,39 In addition, TB is a marker of cancer cells that undergo epithelial-to-mesenchymal transition;41,42 these cells are supported by key signaling molecules such as twist-related protein 1 (TWIST1) and TWIST2 in the surrounding stroma. 43 However, the prognostic potency of these markers may not be identical. Eriksen et al 39 conducted a study that included 573 stage II patients and compared the prognostic role of TB and TSR and found that TB had no prognostic value. In our study, we also found a significant correlation between TB and TIP, 40 both of which are important patient prognostic factors, particularly TB; however, due to the heterogeneity of TSR in our cohort, no correlation was found among TB, TIP, and TSR, and larger study sample sizes are needed in the future.
The preoperative LMR has long been regarded as an important prognostic indicator in CRC. Previously, Stotz et al 25 conducted a study of 372 stage II to III patients and reported that an elevated preoperative LMR was significantly associated with increased OS times, but this was limited to stage III patients. Ozawa et al 44 conducted a study that included 117 stage IV patients and found that LMR was not correlated with DFS outcomes but was linked to cancer-specific survival outcomes in patients who underwent curative resection. Subsequently, Chan et al 29 reported in a study of 1623 stage I to IV patients and found that the LMR was superior for predicting OS outcomes in comparison to the results obtained with other established biomarkers. Recently, Tan et al 26 performed a meta-analysis including 11 783 patients and found that a high LMR was a significant predictor of better DFS and OS outcomes and was also associated with tumor invasion depth and tumor size. In our study, the preoperative LMR was also significantly correlated with histological grade and tumor diameter and boundary linked to invasion depth; in addition, the LMR was an independent prognostic factor for DFS and OS outcomes, which was in line with previous reports.25,26,29
Interestingly, the LMR is believed to be an indicator of the inflammatory process not only at the tumor level but also systemically and can be manipulated by several cytokines, growth factors, and other mediators released by tumor cells and tumor-associated stroma. 29 From this point of view, TB, TSR, and TIP could potentially be associated with LMR; a typical example is TB featuring increased expression of CXCL12, 45 which plays an important role in regulating lymphocytes and monocytes.46,47 Surprisingly, no significant correlation was found between TB and peritumoral or intratumoral inflammatory infiltration; 48 additionally, the TSR was not found to be associated with the systemic inflammatory response in a previous report. 13 In our study, we also failed to find a correlation between LMR and TB, TSR and TIP, and additional studies are still needed in the future.
The present study had some limitations. First, the study was retrospectively performed at a single center, and the limited sample size may have impaired the statistical power and biased the findings; in particular, the relatively small proportion of high TSR in the cohort may have influenced the results. Second, as some patients, in particular those staged III and IV, subsequently received chemotherapy and other therapies after surgery, the final survival outcome of the patients could have been affected by these treatments. Third, the proportion of patients with distant lesions in the cohort was relatively low, and the study of more patients with these characteristics could balance the demographic characteristics. Fourth, some important molecular information, such as MSI and K-Ras status, was lacking. In previous studies, correlations among MSI and TB, TSR, and TIP have been reported.16,35,38,49 Ultimately, additional studies with larger sample sizes in the future could attenuate these biases and validate the results of this study.
Conclusion
In conclusion, our results indicate that TB, TIP, and LMR are useful prognostic markers for CRC; however, LMR is likely to be the only independent prognostic factor for both RFS and OS outcomes.
Footnotes
Acknowledgments
The study was conducted with grants from the Chinese Natural Science Foundation (81503391) and Sanya Medical and Health Science Innovation Project (2018YW06 and 2016YW08).
Ethics Statement
The study was approved by the ethics committee of Hainan Hospital of PLA General Hospital (approved ID: 301HLFYLS15), and written informed consent was obtained from the patients or his/her authorized relatives.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.