
Abstract
Purpose:
To evaluate geometric and dosimetric effects of bra application during radiotherapy planning for breast cancer patients with large and pendulous breasts.
Materials and Methods:
Twenty patients with chest sizes >38 inches between April 2019 and July 2019 underwent radiotherapy planning with and without a radiation bra (Chabner XRT®). Geometric and dosimetric parameters included the breast volume, superior-inferior (SI) distance, separation (S) as the distance of the longest diameter of the clinical target volume (CTV), conformity number (CN), and homogeneity index (HI) of CTV. The organs at risk (OARs) were defined as the lungs, heart, and liver.
Results:
The use of the radiation bra provided mean changes of −0.51 cm for S, −1.45 cm for SI, and −61.18 cc for breast volume (all P < 0.05). Breast volume was correlated with bra-related changes in cross diameter (r = 0.641, P = 0.002) and volume (r = 0.680, P = 0.001). Significant dose reductions were observed for the lungs (mean V10: 19.58 cc, V20: 17.13 cc, Dmean: 86.24 cGy) and heart (Dmean: 170.23 cGy). No significant differences were observed for CN (0.62-0.67) and HI (0.19-0.20) of the CTV.
Conclusion:
The application of a radiation bra was associated with better geometric and dosimetric planning parameters, with a smaller CTV and lower doses to the OARs (lungs and heart) in the radiotherapy field. In addition, we expect that bra use during radiotherapy would provide emotional benefits.
Introduction
Radiotherapy plays an important role in managing breast cancer that is treated using breast-conserving surgery. 1 Three-dimensional conformal radiotherapy (3DCRT) is commonly used during breast radiotherapy and is performed using opposite tangential field arrangements, with the field sizes determined based on the breast’s volume and shape. Although treatment planning generally requires highly conformal and homogeneous dose distribution, heterogeneous dose distributions can occur with or around the target volume. Large or pendulous breasts have a large inframammary fold and lateral displacement of the structure, which affects the radiotherapy dose distribution and risk of skin toxicity. 2,3 These conditions also influence the dose that is delivered to the organs at risk (OARs), such as the lungs and heart. Therefore, breast volume is closely correlated with the degree of dose heterogeneity. 4,5
The lateral decubitus position using the large fabric band showed excellent dosimetric profile. 6 It extremely reduced the dose to the heart and ipsilateral lung for patients with large breasts. Prone position also provided a favorable alternative for radiotherapy for patients with pendulous breasts. 7 Nevertheless, there are limited studies regarding the dose distribution during whole-breast irradiation according to bra use. 8,9 Therefore, the present study aimed to evaluate the geometric and dosimetric effects of bra application during radiotherapy planning for women with large and pendulous breasts.
Materials and Methods
Patients and Radiation Treatment Planning
This retrospective study included 20 patients with breast cancer (10 left-side cases and 10 right-side cases) who underwent radiotherapy between April 2019 and July 2019 in our institution. We evaluated the patients who had the large or pendulous breasts, which were hanging below the inframammary fold and had not much fullness at the top of the breast. All patients underwent computed tomography (CT)-based simulations for planning with and without a radiation bra (Chabner XRT®; CIVCO, USA). According to the patient’s chest size and oncologist’s judgment, a suitable bra was applied to each patient, and bra size was 96.52 cm or more generally. The patient was immobilized in the supine position on a breast board with both arms raised. This study was approved by the Institutional Review Board (N0: 2020-10-010). All patients provided an informed consent for 2 CT simulations and radiotherapy. The patient records/information were anonymized and de-identified prior to analysis.
The clinical target volume (CTV) was defined as the whole breast and OARs as the heart, liver, and both lungs. The CTV was delineated according the breast cancer contouring atlas of the Radiation Therapy Oncology Group. Treatment was planned with 3DCRT using tangential beams. The isocenter point was at the center of the CTV, and the field margins in the superior-inferior directions were adjusted 0.5 cm from the CTV. The prescribed dose was 50.04 Gy in 28 fractions, and plans were considered acceptable if the CTV was covered by 95% of the isodose curves. Dose tolerances for ipsilateral lung were defined as <20% for V20, <35% for V10, and <18 Gy for the mean lung dose. Heart dose constrain was defined as <5 Gy for the mean heart dose. The radiation therapy was subsequently administered in daily fractions without the radiation bra.
Geometry and Dosimetry Analyses
Data from each patient’s scans with and without the radiation bra were transferred to the EclipseTM treatment planning system (Varian Medical System, Palo Alto, CA). Geometrical changes were evaluated by comparing the scans with and without the radiation bra, and the total breast volume (V) in the CTV was measured. Using the largest tangential field level, we evaluated the following bra-related factors: cross (S: separation) as the longest diameter of the CTV shown (Figure 1) and the superior-inferior (SI) distance between the upper and lower margins of the CTV, which was counted based on the number of CT slices.

A, Patient simulated with a radiation bra. B, The geometrical definition of the breast. The separation (S) was defined as the longest diameter of the clinical target volume (CTV).
The CTV coverage was evaluated via the conformity number (CN) and the homogeneity index (HI):

where TV95% is the target volume covered by at least 95% of the prescription dose, TV is the target volume, and V95% is the volume of the 95% isodose. The D2%, D50%, and D98% parameters were defined as the received dose by 2%, 50%, and 98% of the TV, respectively. 10,11
The lung parameters were defined as the volumes that received 10 Gy (V10) and 20 Gy (V20), as well as the mean dose delivered to the lung (Dmean). We also considered the mean dose (Dmean) received by the heart, the liver volume that received 90% of the prescription dose (V90%), and the mean dose to the ipsilateral axillary lymph node.
The Wilcoxon’s signed rank test was used to compare the variables from the scans with and without the radiation bra. All statistical analyses were performed using IBM SPSS software (version 20.0; IBM Corp., Armonk, NY, USA) and differences were considered statistically significant at P-values of ≤0.05.
Results
The patients’ median age at the radiotherapy was 64 years (range: 42-74 years). Breast volume was measured with 500-800 cc in 40% (n = 8), >800 cc in 35% (n = 7), and <500 cc in 25% (n = 5), respectively. Among them, 16 patients had pendulous breasts regardless of breast volume. Detailed information regarding patient characteristics is presented in Table 1. Table 2 shows the values for cross, SI distance, and volume according to radiation bra use. The use of the radiation bra was associated with mean changes of −0.51 cm for the cross diameter, −1.45 cm for SI distance, and −61.18 mL for volume (all P < 0.05). The geometric parameters were all superior with bra use, and larger breast volumes were related to greater differences in cross distance and volume difference (Figure 2). Breast volume was linearly correlated with the change in cross distance (r = 0.641, P = 0.002) and change in volume (r = 0.680, P = 0.001).
Baseline Patient Characteristics.

Abbreviation: RT, radiotherapy.
Comparing the Geometric and Dosimetric Results Between the Two Groups.

Abbreviations: Cross, separation(S) as the longest diameter of the CTV; SI, superior-inferior distance of the CTV; Volume, total breast volume (V) in the CTV.
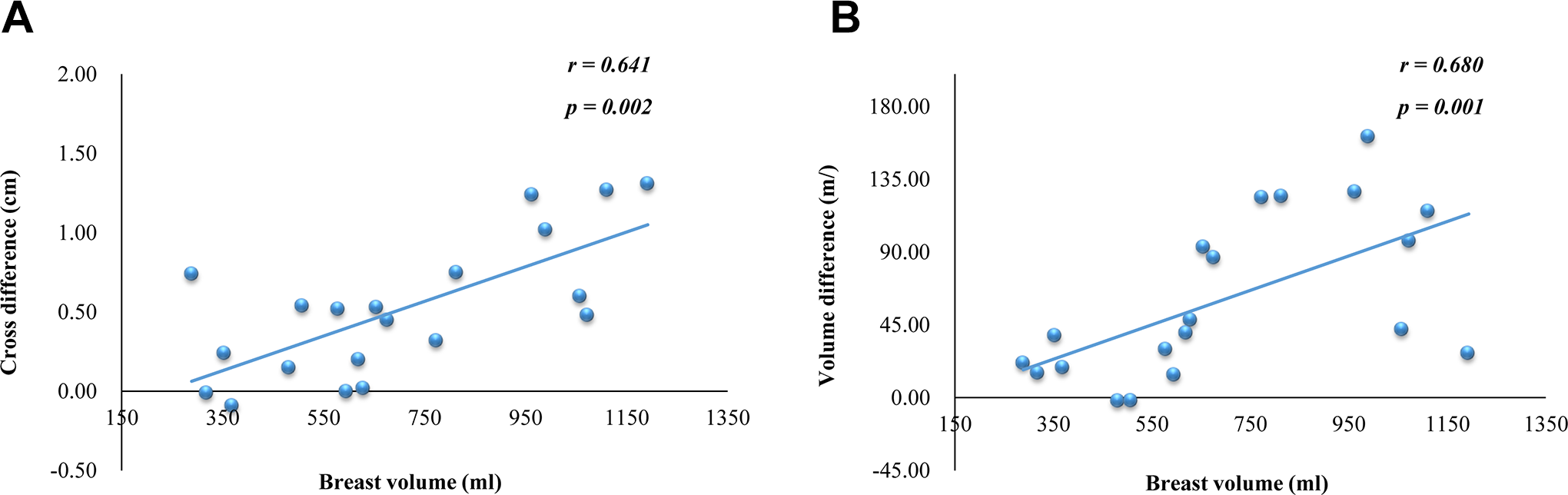
The relationships between breast volume and cross diameter difference (A) and volume difference (B).
Table 3 and Figure 3 show the dosimetric results for the CTV and OARs according to radiation bra use. No significant differences between the two groups were observed in terms of average CN (0.62-0.67) and average HI (0.19-0.20). In addition, there were not dosimetric differences in TV95% (88.71%-90.18%), D98% (4294.15-4336.40 cGy), D50% (5073.08-5084.21 cGy), and D2% (5296.01-5319.23 cGy) for the CTV. From a dosimetric point of view for the OARs, there was significant differences dose to the ipsilateral lung. The V10 with and without bra were 116.45 ± 53.09 cc and 136.03 ± 63.38 cc, respectively (P = 0.002), V20 were 79.12 ± 37.81 cc and 96.25 ± 46.89 cc, respectively (P = 0.002). The mean lung dose was 469.3 cGy with bra and 555.54 cGy without bra (P = 0.001). Bra use was associated with reductions in the doses delivered to the ipsilateral lungs (mean V10: 19.58 cc [range: 7.28-20.45 cc], mean V20: 17.13 cc [range: 7.84-17.53 cc], Dmean: 86.24 cGy [range: 65.40-170.90 cGy]) and to the heart (Dmean: 170.23 cGy [range: 3.50-210.00 cGy]). There was also significant mean heart doses between two groups (190.27 cGy vs. 256.28 cGy, P = 0.028). Bra use was not associated with a significant reduction in the dose delivered to the liver (P = 0.327). None of the dosimetric parameters was linearly correlated.
Conformity Number (CN), Homogeneity Index (HI), and Parameters for Target Volume Coverage.a

a Data are shown as mean (standard deviation). TV95% , the target volume (TV) covered by at least 95% of the prescription dose; D98%, D50%, and D2%, dose by 2%, 50%, and 98% of the TV.

Dosimetric parameters of both groups with or without bra. All parameters were significantly different between groups. Data on box represents interquartile range (Q3-Q1). The upper and lower of bar means the maximum and minimum value of data.
Discussion
The present study revealed that use of a radiation bra was associated with possible reductions in the values for the CTV in the treatment field and the doses to the lungs and heart. Similarly, previous studies have indicated that large or pendulous breasts were associated with an increased and inhomogeneous dose distribution in the OARs and breast. 4,12 Our results suggest that use of a radiation bra may help minimize the inframammary skin fold and re-position the skin of pendulous breasts, as it helped decrease the cross diameter and the superior-inferior margin of the CTV. Excluding loose normal tissues from the treatment area might help reduce the dose that is delivered to normal skin, as folding and displacement of a large breast with loose normal tissue can lead to acute side effects that are related to dose heterogeneity. 8 We also observed that radiation bra use was associated with a greater reduction in volume for larger breasts. Previous reports have classified breast size as large (CTV: ≥1,600 cc), medium (975-1,600 cc), and small (500-975 cc), with acute grade ≥2 breast skin toxicity observed in patients with medium or large breasts, but not in patients with small breasts. 13 -15 Thus, helping to minimize the CTV may improve treatment-related outcomes. During radiotherapy, ideal conformation is defined as a CN value of 1 and a homogeneous dose distribution is defined as an HI of 0. 16 The present study failed to detect significant differences in the CI and HI values according to radiotherapy bra use, which suggests that the bra helped increase safety for the normal skin and preserved the dose coverage of the CTV.
Bra use was also associated with reductions in the doses delivered to the lungs and heart. In this context, changes to the breast volume and cross distance can influence the dose delivered to adjacent normal organs. One technique to reduce the dose delivered to OARs is intensity-modulated radiation therapy, although Hannan et al have reported that greater breast size was associated with higher heart and skin doses, even when intensity modulated radiation therapy was used. 17 The prone position has also been suggested for patients with large breasts, in an attempt to improve the dose homogeneity within the breast and reduce the dose to the OARs. 7 Compared to supine, prone position reduced the dose inhomogeneity within the target by approximately 15%. It was also associated with lower delivered doses to the mean lung as 3.8 Gy and maximum heart as 5.1 Gy. Whole breast radiotherapy in the lateral decubitus position for patients with large breasts showed extremely lower ipsilateral mean lung dose as 0.96 Gy and mean heart dose 1.35 Gy. 6 Nevertheless, using a radiation bra and the supine position for patients with large breasts was associated with a reduction in breast ptosis, which significantly reduced the chest wall separation and the heart volume within the treatment field. 8 Furthermore, Heineman et al 18 reported that the chest wall separation exhibited a strong positive correlation with the dose delivered to the ipsilateral lung. The separation of ≥28 cm was associated with increased volume values (V5, V10, and V10 of the lung), and our results indicated that a larger cross distance was associated with better chest wall separation.
Many researchers have evaluated the psychological condition of women who undergo radiotherapy, 19,20 which has revealed post-radiotherapy rates of 64% for anxiety and 50% for mood disorders. 21 Thus, use of medications for these conditions has been linked to reduced anxiety, reduced fatigue, and improved quality of life among women undergoing radiotherapy for breast cancer. 22 In addition, we expect that bra use during radiotherapy would provide emotional benefits.
This study had several technical limitations. First, after putting on the radiation bra, some adjustments may be needed after the patient lies down on the breast board because the bra cannot prevent changes related to those movements. Although the dosimetric effects on a radiation bra were analyzed in this study, the reproducibility and skin dose are related to the clinical results for the breast cancer. Further study assessing the efficacy of bra for large or pendulous breast should be stratified by the breast reproducibility and skin dose. Second, it can be difficult to mark the isocenter lines on the bra rather than on the skin. Thus, it would be useful to have personalized and fitted bras that can help hold the breast’s intended position, even during patient movement and position changes. Owing to retrospective nature and the small number of patients, we need further study to see what is the best cutoff parameters and values for use the radiation bra. Nevertheless, it appears that use of a radiation bra helped improve the dosimetric parameters for patients with large and pendulous breasts who were undergoing breast radiotherapy.
Conclusion
During radiotherapy for breast cancer, large and/or pendulous breasts make create dose inhomogeneity in the treatment field and lead to higher doses delivered to the adjacent normal organs. Our results suggest that application of a radiation bra may help preserved the dose coverage of the CTV and reduce the dose delivered to the OARs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from Jeju National University Hospital in 2019.