
Abstract
Colorectal cancer (CRC) is one of the most common malignant tumors in the digestive tract in humans. The development of colorectal cancer is composed of multiple stages, starting with benign adenomatous polyps in the inner wall of the large intestine and rectum, and then gradually developing. Then it developed into advanced adenomas carcinoma in situ and invasive carcinoma. Represents the distant metastasis of the most advanced development. The purpose of this review is to novel routine screening and diagnostic methods (e.g., Endoscopy and CT colonoscopy, SEPT9 methylation assay, Fecal test) and find reliable molecular markers for early diagnosis of CRC.
Introduction
According to data from the American Cancer Society (ACS), an estimated 147,950 people will be diagnosed with colorectal cancer and an estimated 53,200 people will die of colorectal cancer, with an estimated 3,640 deaths among those younger than 50 years of age in 2020. 1 Colorectal cancer is the third most common cause of cancer-related deaths (other than skin cancer diseases) in men and women outside the United States, making it the third most common cause of cancer-related deaths in men and women outside the skin in the United States.
Colorectal adenoma may progress to an advanced adenoma (> 1 cm in size, and/or villous histology), and eventually to colorectal cancer. The accumulation of mutations and changes in epigenetics lead to the development of colorectal adenoma to colorectal cancer. 2 This process takes about 10-15 years, but in some settings (for example, in patients with Lynch syndrome) can develop more quickly.
About 65% of CRC cases are sporadic and the rest are familial. About 85% of sporadic CRCs show chromosomal instability (CIN), and are accompanied by changes in chromosome number and structural abnormalities. 3 -5 About 15% of sporadic colorectal cancers have a high frequency microsatellite instability (MSI) phenotype. 5,6 About 15% of sporadic colorectal cancers have a high frequency microsatellite instability (MSI) phenotype. 7 In recent years, biomarkers that have contributed to the early diagnosis and screening of CRC have received increasing attention.
Early colorectal cancer refers to any size of colorectal epithelial tumor with limited infiltration depth in the mucosa and submucosa, regardless of lymph node metastasis. Under endoscopy, it is divided into 3 types (developmental morphological types):
Lumen type: the lesion has obvious lumen and intestinal cavity, and its bottom diameter is significantly smaller than the maximum diameter of the lesion (pedicled or subpedicled); Or the lesion is hemispherical and the diameter of the base part is obviously larger than the diameter of the lesion head. (2) Flat type: those with high and low lesion or flat uplift are collectively referred to as flat type. (3) Shallow surface depression type: those with obvious depression compared with the surrounding mucosa endoscopic ultrasonography showed thickening of the mucosa, disorder of the layers, interruption and disappearance of boundaries of the layers in colorectal lesions, and small irregular hypoechoic shadows.
Status of Screening and Diagnostic Methods
Currently, many screening tests are used to screen CRC, including noninvasive and invasive tests. The gFOBT (Guideline Fecal Occult Blood Test), Fecal Immunochemistry Test (FIT), FIT-DNA (Multi-Targeted Fecal DNA), SEPT9 Test, and Direct Visualization Tests (Colonoscope, CT Colonoscopy, and Sigmoidoscopy) are serviced by the United States. The Working Group (USPSTF) is listed as the current CRC screening program. 8 gFOBT is not sensitive to the screening of advanced colorectal tumors. Among the opportunistic and procedural screening of CRC, quantitative matching has become the most widely used noninvasive survey. 9 But the levels of f-Hb may vary significantly from day to day, which can greatly affect the result; One defecation was so haphazard that there was concern that the samples were not representative; Limited sensitivity for advanced adenoma and needs repeated screening. Colonoscopic screening and surveillance have a well-documented benefit in reducing the risk of CRC by direct removal of precancerous lesion and early detection of CRC 10 and has long been the gold standard for screening and diagnosis of colon cancer. 11,12 But the most prone to colonoscopy is missed diagnosis.The more common missed diagnoses are adenomas less than 10 mm, atypical serrated polyps and lipomas.
Molecular Mechanisms in the Early Development of CRC
Heredity and Epigenetics
Loss of genomic and/or epigenomic stability has been observed in most early neoplasias (i.e., abnormal crypt lesions, adenomas, and serrate polyps), and their loss accelerates the accumulation of oncogene and tumor suppressor gene mutations and epigenetic changes. The malignant transformation of colon cells is driven by these mutations and epigenetic changes through the clonal expansion cycle selected for the cells with the most aggressive and malignant behavior. Microsatellite instability (MSI), chromosomal instability (CIN) and CpG island methylation phenotype (CIMP) are the 3 main ways that cause the development of colorectal adenoma to cancer. 13,14 Therefore, the substances involved in the process of CRC heredity and epigenetics can be used as molecular markers to monitor the progress of CRC and contribute to the early diagnosis of CRC. Some have been confirmed, others are still being studied.
CpG island methylator phenotype
In addition to mutations, the 2 mechanisms of promoter hypermethylation and chromosomal instability (CIN) also lead to the destruction of gene function and participate in the progression of adenoma to cancer. CIMP refers to a subset of CRCs with a large number of promoter CpG island genes that are widely hypermethylated. 15 In normal cells, the CpG site located on the CpG island promoter is not affected by methylation; But in colorectal cancer (CRC), the opposite is true, and about 10% is expressed in normal colonic epithelial cells active genes 15 ; The principle is that hypermethylation of the promoter CpG island inactivates actively expressed tumor suppressor genes or tumor-related genes, resulting in a series of changes in cells, such as promoting cell proliferation or inhibiting apoptosis or senescence, thereby promoting tumorigenesis. The transcription of many genes must be dependent on the methylation of CpG islands in gene promoter regions. However, once the hypermethylation of these CpG islands changes, it will inhibit the binding of transcription factors to the promoter region, resulting in gene inactivation. PCR detection can clearly detect DNA methylation changes, so CIMP is a good target for early detection of CRC, such as SEPT9 gene promoter.
Microsatellite instability
Microsatellite is a short sequence consisting of 16 bases. It is repeatedly distributed in the coding and non-coding regions of the entire genome. Because of this, they are particularly prone to errors during replication, but can usually be repaired by the MMR system. The interaction of the 4 proteins MLH1, MSH2, MSH6 and PMS2 constitutes the MMR repair system. The MMR repair system detects the gene mismatch and cuts it off. At this time, under the action of DNA polymerase and DNA ligase, the correct DNA strand can be re-synthesized and recombined. When MSI occurs in the coding regions of genes involved in some key cell functions and pathways, it may have carcinogenic potential.
Chromosomal instability
CIN refers to an inherited phenomenon in which cells of an individual’s body are prone to spontaneously or induce breakage. The nucleus will mutate due to CIN, resulting in aneuploid formation, subkaryotype expansion, chromosomal rearrangement, and high frequency heterozygosity loss of tumor suppressor gene loci. The recognition of CIN tumors is attributed to the mutation accumulation of KRAS proto-oncogene GTPase (KRAS), B-Raf proto-oncogene serine/threonine kinase (BRAF), and tumor suppressor genes such as APC and tumor protein p53 (TP53), thereby promoting CRC happened.
APC inactivation is the first event in the CIN process, and tumorigenic KRAS mutation occurs in the adenoma stage, and then it is transformed into malignant tumor through 18q chromosome deletion and 17p chromosome tumor suppressor gene TP53 inactivation. The genomic changes involved in colorectal cancer are shown in Figure 1. Mutations in the WNT signaling pathway usually cause colorectal cancer, and then tumor cells will follow other signaling pathways (including RAS, RAF, MAPK, transforming growth factor-TGF-TGF, p53, and phosphatidylinositol kinase (PI3 K)/AKT) progress while relaxing.
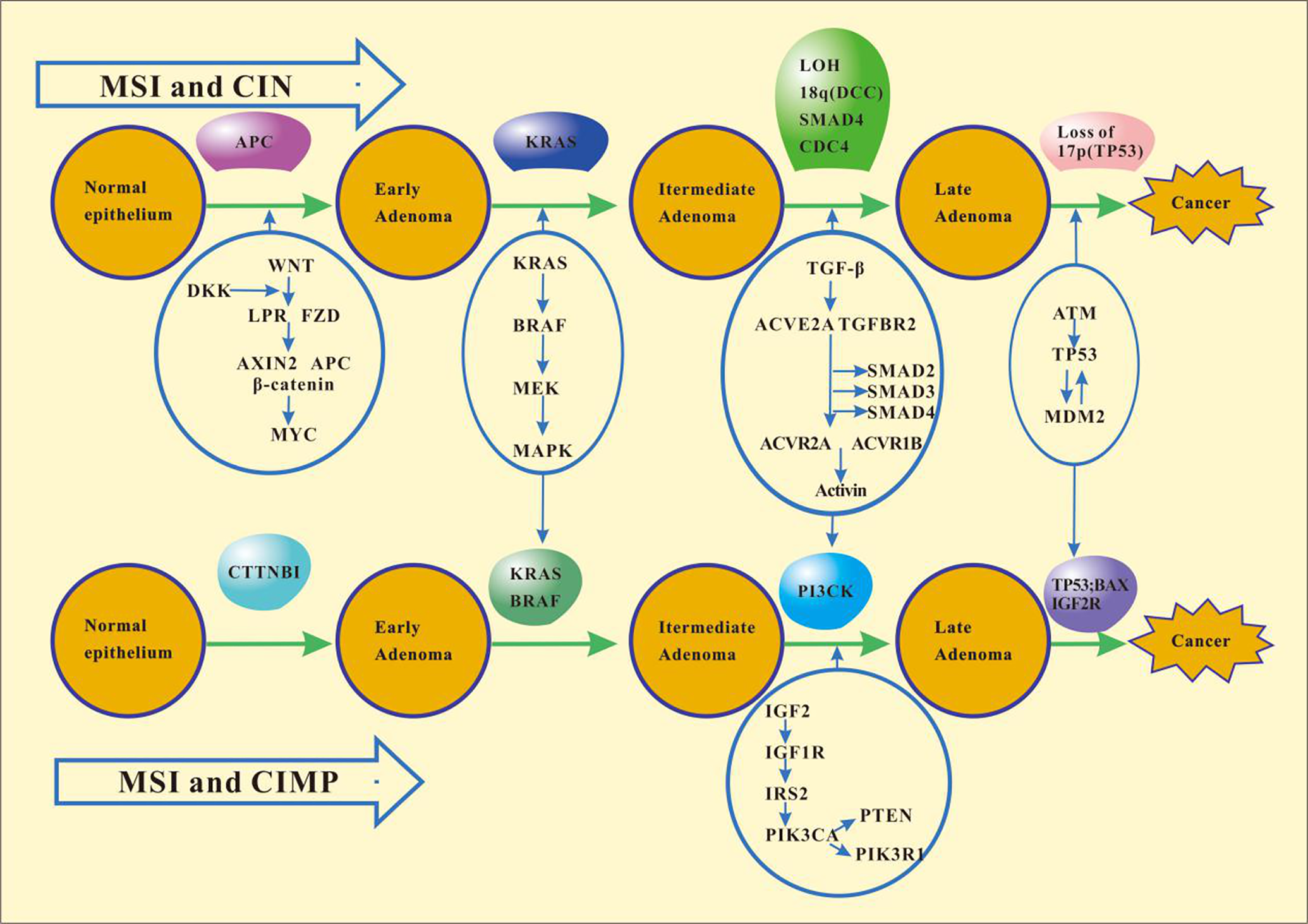
Schematic of genomic changes in colorectal cancer development. CTTNBI, catenin-β1; BRAF, B-Raf proto-oncogene serine/threonine kinase; DCC, DCC netrin 1 receptor; BAX, BCL2 associated X apoptosis regulator; IGF1 R, insulin like growth factor 1 receptor; CDC4, cell division control protein 4. MAPK, mitogen-activated protein kinase; PI3KCA, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit-α.
Predictive Molecular Markers in the Molecular Mechanism of Early Colorectal Cancer
The most common mutations in colorectal cancer include those in APC, catenin-β1 (CTNNB1), KRAS, BRAF, SMAD family member 4 (SMAD4), transforming growth factor-β receptor 2 (TGFBR2), TP53, phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit-α (PIK3CA), which promote tumorigenesis by perturbing the function of key signaling pathways, including the WNT β-catenin, epidermal growth factor (EGF) mitogen-activated protein kinase (MAPK), phosphatidylinositol 3-kinase (PI3 K) and TGFβ signaling pathways, or by affecting genes that regulate the central behaviors of cells, such as DNA repair and proliferation. Therefore, detection of these mutated genes can reflect the progress of colorectal cancer to a certain extent, realize the early diagnosis of colorectal cancer, and achieve the purpose of early detection and early treatment. Table 1 lists molecular markers that are predictive of early colorectal cancer. 16 -22
Molecular Markers That Are Predictive of Early Colorectal Cancer.

APC
Adenomatous Polyposis Coli (APC) is an oncosuppressor gene which acts as a cellular gate keeper to prevent the development of tumors in the colon. But APC will become the oncogene for FAP when it mutates in the germline. APC mutation is the first event of colorectal cancer, and can be considered as a prediction marker of early colorectal cancer. When the APC gene is mutated, a disrupted complex is formed, thereby inhibiting degradation of the tandem protein. After this process, a lot of catenin can be accumulated.Then catenin translocates to the nucleus, and the transcription of tcf regulatory genes is activated, promoting cell proliferation. Therefore, dysplastic cells begin to grow under the stimulation of APC mutations or other mechanisms that disrupt the WNT signaling pathway. These cells initially took over the crypts and gradually formed polyps. 16 -18 Therefore, APC mutation is considered as a good diagnostic marker to identify CRC risk individuals.
TP53
TP53 is a tumor suppressor gene located on the short arm of chromosome 17. It has always been defined as the guardian gene of the genome and is involved in many cell activities, including DNA repair, cell cycle arrest, aging, apoptosis and metabolic response to various stress signals. Approximately 50%-70% of CRC mutations in p53, which are tumor suppressor genes, are positively correlated with poor prognosis. Therefore, when TP53 loses its function, it will facilitate the proliferation of damaged DNA to daughter cells and the malignant development of CRC. At the same time, p53 gene is also considered as the prognostic gene of CRC.Meanwhile, p53 gene is also considered as a prognostic gene of CRC.
KRAS
The KRAS gene belongs to the RAS gene family. It belongs to membrane-bound GTP/GDP protein and has inherent GTPase activity. It is involved in regulating cell proliferation, differentiation or survival signaling pathways, 16 and mutations are found in 17%-25% of cancers and 35%-45% of CRC. RAS GTPase becomes constitutively active through these mutations. 2 However, active RAS can induce many signaling pathways in tumorigenic cells, leading to the occurrence and development of CRC.The high frequency of KRAS mutations and their occurrence in the relatively early stages of tumor progression show that KRAS has an indispensable role in human tumorigenesis. And detecting whether KRAS mutation is important for the diagnosis of colorectal cancer. KRAS is referred to as predictive factor by ASCO, EMSO and NCCN.
PIK3CA (Phosphatidylinositol-4,5-bisphosphate 3-kinase)
Phosphatidylinositol-inositol-3 kinase (PI3 K) is a kind of cell-specific phosphatidylinositol-inositol-3 kinase, which plays a pivotal role in various cellular functions. It leads to an increase in the PI3 K signal which is one of the most common changes that occur in human cancers.Somatic mutations are often found on PIK3CA and PIK3CB in cancer cells and are known to induce activation of PI3 K. PIK3CA gene mutation is classified as an advanced adenoma event. The mutated PIK3CA gene can reduce apoptosis and promote tumor invasion and metastasis.
PTEN (Hosphatase and tensin homologue protein)
PTEN is the first tumor suppressor gene with phosphatase activity. It is located at chromosome 10q23 and has phosphatase activity, which can act on lipid and protein substrates to dephosphorylate them PTEN dephosphorylates PIP3 to PIP2. Loss of the PTEN gene can occur in the early stages of cancer.It is involved in many cellular activities, such as the regulation of Akt (serine threonine protein kinase) function;Inhibition of PI3 K (phosphatidylinositol-3-kinase) /Akt (Pkb, protein kinase B) signaling pathway; Negatively regulate cell growth, inhibit cell proliferation, and induce cell apoptosis. 24
Molecular Biomarkers in Stool
The idea behind faecal testing is that both early and late precancerous lesions can cause bleeding, which can be detected by existing technology by shedding blood cells into the lumen of the intestine. 2 DNA, RNA and proteins used to detect CRC in feces are shown in Table 2. 23,25 -27
DNA, RNA and Proteins Used to Detect CRC in Feces.

DNA
Because human gut are alkaline environment, to save, and high quality DNA extracted DNA have advantage, and if the subjects suffering from cancer, feces can also contain lots of cancer cells and tumor off free of tumor DNA, therefore, excrement gene methylation detection method as a noninvasive diagnosis of colorectal cancer is gradually recognized abnormal methylation in colorectal cancer early. Abnormal gene methylation in feces has become a highly effective and less invasive method to screen colorectal tumors. Stool detection with single gene, such as secreted frizzled related protein 2 (SFRP2), family member 4 (NDRG4), bone morphogenetic protein 3 (BMP3), etc. There are also multi-gene combination tests, such as SFRP2 and WNT inhibitory factor 1 (WIF-1) combination tests.
RNA
MicroRNAs is a single-stranded RNA molecule length less than 22 nucleotides, it inhibits messenger RNA translation, also can promote the mRNA degradation. 28,29 In recent years, research has shown that after the miRNA gene expression is an important transcription regulatory factor, also is the key to the tumorigenesis adjustment factor to the existence of microRNAs tissue fluid blood in the urine and other biological samples, complex controlling cancer cell signal transduction and various physiological and pathological process.Due to their tissue specific expression, miRNAs are expected to become biomarkers.
Studies have shown that miRNAs can be stably present in feces, and there are also differences in miRNA expression in feces of CRC patients and healthy individuals that can be repeatedly extracted.The test works by quantifying RNA from tumor cells that fall off the lumen walls to determine whether they have CRC. Summarize the relevant reports found that miR-92a, 30 miR-20a, 31 miR-21, 30 miR-135, 32 and miR-144* are differentially expressed in CRC patients. But, now we all use small sample sizes to study fecal DNA, and the techniques and methods of these studies are not mature. However, miRNA as a biomarker can better indicate the formation and development of tumors, making it promising to use fecal miRNA as a marker for the diagnosis of CRC.
Protein
Hemoglobin in feces can be detected by gFOTB and FIT, but due to the low specificity of guaiac-based fecal occult blood test (gFOTB), many places no longer use gFOTB to detect CRC or only for auxiliary diagnosis of CRC. FIT is considered a new guaiac-based FOBT. It is a globulin antibody that does not cross-react with the hemoglobin found in meat, so it is not affected by foods with higher peroxidase activity. Quantitative fitting yields numerical estimates of fecal hemoglobin concentration (f-Hb). While the numerical of f-Hb is low, FIT has high sensitivity for CRC. Therefore FIT can therefore be used to provide rapid screening for colorectal cancer, especially when symptoms are more severe. 9,33
Molecular Biomarkers in Blood
DNA, RNA, proteins and other molecular biomarkers used to detect CRC in blood are shown in Table 3. 34,35,36,37,40,41
DNA, RNA, Proteinsand Other Moleculer Biomarkers Used to Detect CRC.

Circulating tumor DNA (ctDNA)
Currently, changes in ctDNA epigenetics are being studied as a method for malignant tumor diagnosis and recurrence monitoring. 42 Current research shows that the free methylated SEPT9 gene (mSEPT9) in the peripheral blood can be used as a biological tumor marker for colorectal cancer. As one of the genes of SEPT family, septin9 is widely present in eukaryotic cells and is a tumor suppressor gene. The SEPT9 protein it encodes is involved in biological processes such as cell division, vesicle transport, and cell membrane remodeling, and these evolutionary processes have all participated in the development of tumors. And when it is methylated, it will inhibit the transcription and translation of the SEPT9 gene, affecting the normal expression of the SEPT9 protein, resulting in the loss of corresponding cell functions, which in turn leads to abnormalities and canceration during cell division. It is currently approved. The first screening principle of colorectal cancer serum detection is that qRT-PCR can be used to detect tumor DNA in the peripheral blood of patients with colorectal cancer and the release cycle of colorectal cancer necrosis and apoptotic cells. Therefore, the risk of CRC can be judged by detecting the DNA methylation level of the SEPT9 gene-specific promoter region in peripheral blood. In addition to SEPT9, other methylated biomarkers including tachykinin-1 (TAC1), somatostatin (somatostatin, SST), and runt-related transcription factor 3 (RUNX3) 38,43 have been proven to be effective in detecting multiple samples. Type of CRC. But a lot of research is still needed to prove its role in the early diagnosis of CRC.
RNA
microRNA
MiRNAs can be released into the peripheral blood by cancer cells, so certain circulating mirnas associated with specific diseases can be detected in serum and plasma. The correlation between mirnas and cancer has been studied in recent years, which is expected to be a potential biomarker for the diagnosis and monitoring of CRC progression or treatment in the future.
It was found that serum let-7 g, 44 miR-21, 37,38,43 miR-92a, 45 miR-29a were highly sensitive and specific as biomarkers for CRC diagnosis. 40 A study by Imaoka et al showed that Mir-1290 can promote epithelial mesenchymal transformation (EMT), proliferation and metastasis potential, and is expected to be a diagnostic marker for colorectal cancer. Although mirnas play an indispensable role in the occurrence and development of colorectal cancer, no mirnas have been found in the blood to screen for CRC, which will be a major breakthrough in the future non-invasive detection of CRC.
CircRNAs
Due to the low expression level of circrnas, these circrnas, as rare RNA types, can only be treated as transcriptional noise circrnas as post-transcriptional regulatory retainers that compete with other RNA molecules to bind protein fragments. They can regulate the effects of RNA binding proteins and RNA molecular concentration;Some circrnas participate in endogenous competitive RNA (ceRNAs) regulatory networks. Compared with mirnas, circrnas have no end, which also makes them resistant to mirNA-mediated RNA degradation and other accounting extranuction activities. Bioinformatics analysis showed that most circrnas were significantly down-regulated in colorectal cancer tissues and cell lines. 41
Huang et al, 35 have demonstrated that circHIPK3 is significantly overexpressed in colorectal cancer compared with normal subjects. Cir-ITCH expression was significantly reduced in colorectal cancer compared with adjacent non-cancer tissues. These studies suggest that specific circrnas play a critical role in the development of colorectal cancer. Recent studies have shown that ringed RNA can be detected in bodily fluids such as saliva and plasma. The analysis of candidate circRNAs from RNA-SEQ data showed that the exosomes of colorectal cancer were more abundant than those of donor cells, suggesting that circRNAs may be involved in the development and progression of colorectal cancer.
However, the molecular role of circRNAs in the prevention, diagnosis and treatment of colorectal cancer is not completely clear. But, as more and more circRNAs have been found and are abundant in saliva, exosomes and blood specimens, circRNAs have undoubtedly become important markers in the development process of colorectal cancer.
Protein
CEA and CA 19-9 have low sensitivity and specificity for colorectal cancer screening, and are therefore commonly used to monitor the response to treatment of colorectal cancer. 5,10
sDC-SIGN/sDC-SIGNR
The human DC-SIGN gene is located at 19p13.3, a type II transmembrane protein with a molecular weight of 44KDa and approximately 13 kb in length. Studies have found that DC-SIGN can play an important role in the adhesion migration of DC and the inflammatory response to activate the initial T cells and initiate the immune response as well as the immune escape of pathogens and tumors. 36 DC-SIGNR is called DC-SIGN-related molecule (DC-SIGNR). The gene of DC-SIGNR is adjacent to the similar structure of DC-SIGN, and has 77% homology in amino acid sequence, and the molecular structure is also very similar. 45
Jiang et al, analyzed the correlation between the expression levels of sDC-SIGN and sDC-SIGNR in serum and CEA andCA199 in serum, and found no correlation, suggesting that sDC-SIGN and sDC-SIGNR in serum may be new markers of colorectal cancer. Moreover, although sDC-SIGN and sDC-SIGNR are homologous molecules, their expression trends in serum of colon cancer patients are different. Compared with healthy people, the level of sDC-SIGN is lower in patients with early colon cancer, while the level of sDC-SIGNR is higher than that in healthy people.
The study also found that serum sDC-SIGN and sDC-SIGNR level, can be used as the diagnosis of colon cancer, especially early diagnosis biomarkers of serum sDC—SIGN for the diagnosis of colon cancer has high sensitivity, play a role in colorectal cancer screening, and serum sDC-SIGNR has high specificity, play a role in colorectal cancer diagnosis and differential, combined diagnostic analysis is made for the 2 kinds of markers, both reached the complementary in joint diagnosis process, sensitivity and specificity were greater than 90%, indicating a high diagnostic value.
ADH
In human colorectal mucosa exist a variety of alcohol dehydrogenase (ADH) isozyme (including ADH Ⅰ isozyme activity change is most obvious) and aldehyde dehydrogenase (ALDH) isozyme. Long-term consumption of ethanol produces acetaldehyde, a highly toxic carcinogenic compound, in the presence of ADH. 46 Long-term consumption of ethanol produces acetaldehyde, a highly toxic carcinogenic compound, in the presence of ADH. In theory, acetaldehyde will be decomposed by ALDH, but studies have found that ALDH activity has little difference between cancer cells and normal cells. In other words, cancer cells have a strong ability to oxidize to acetaldehyde from exogenous ethanol, but have a weak ability to clear acetaldehyde. 42 In Jelski’s experiment, the activity of total vasopressin and isozyme I in tumor tissues was significantly higher than that in normal mucosa, which may indicate that these changes may be reflected by the enzyme activity in serum. 46 They also found in the different stages of colorectal cancer, plasma total ADH in each period were significantly higher than the control group and ADH Ⅰwere positively correlated, and the later when it comes to colorectal cancer staging, the higher the sensitivity of the ADH Ⅰ. 41 Total serum ADH sensitive can amount to 60%, ADH Ⅰ sensitivity can reach 76% and the area under ROC curve for ADH I was 0.72, so the serum ADH (especially the ADH Ⅰ) may be as early detection markers of CRC. 39
Interleukin
Cytokine-Interleukin 8 (IL-8)
Cytokines are a category of soluble peptides and have a variety of functions, such as regulating innate immunity and adaptive immune hematopoietic cell growth and repairing damaged tissue that and participate in the carcinogenesis of colitis and colorectal adenoma. Cytokines are divided into 3 types: chemokine lymphoid factor and interferon, of which interleukin-8 in chemokine is the most promising candidate for early diagnosis of CRC.Interleukin-8 (IL-8) is one of the most significantly upregulated chemokines in CRC and has been found to be involved in angiogenesis of a variety of cells, including neutrophils, endothelial cells, macrophages and cancer cells. It has been reported to be involved in the migration of tumor cells, and its expression is associated with angiogenesis, tumor progression and metastasis of various tumors in human and animal models. IL-8 induces CRC cell proliferation and migration, a process that plays an important role through mining and the binding of heparin to epidermal growth factor (EGF-like) growth factor (HB-EGF) as the main ligand of this pathway.
Conclusion
In this review, screening methods and early detection of CRC are reviewed, focusing on a large number of markers currently under study. The ongoing improvement of CRC screening programmes at this stage aims to detect CRC at an early stage, preferably at the pre-cancer stage, so as to reduce CRC related mortality. 16 Current screening and early diagnosis methods are either rapid response to fecal stamping or uncomfortable, expensive and potentially dangerous, leading to low patient compliance. Reasonable screening and early diagnosis methods should be convenient, sensitive, specific, safe, economical and practical. At present, our existing technology requires a high degree of participation and compliance in different screening schemes, requiring the correction of all congeners. More importantly, cost-effective, highly sensitive and specific non-invasive methods need to be developed to reduce patients’ anxiety about CRC screening and improve the acceptability of the screening process.
Due to the increase of potential process and the understanding of the molecular pathways were disrupted, genomics can affect a lot of the early detection of cancer, colorectal cancer because of this many new and better biomarkers and molecular changes help adenoma to carcinoma, malignant transformation, for the development of ideas is of great significance to detect colorectal cancer biomarkers in CRC test research in recent years had the huge progress. 14 But most of the function of the mutations have not yet fully clear, clear so molecular properties in the role of diagnostic tests and treatment decisions are still limited. The development of more easily applicable molecular detection methods for early CRC is critical to improving the prognosis and treatment efficiency, 9 which requires further research. 7
Footnotes
Authors’ Contributions
ZW: Data collection and drafting of manuscript; YL, YZ, HH, TW, SL and WC: drafting of manuscript; SX and ZL: organizing the structure of the manuscript, drafting and editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Key project of Natural Scieces Foundation of Hubei Province (2015CFA078), the Yellow CraneTalent Plan Foundation, Research Fund of Wuhan Public Health Bureau (WX19Q14 and WX18Y11).