
Abstract
Objective:
This study aimed to explore the efficacy and safety of using transarterial chemoembolization (TACE) combined with anlotinib in patients with unresectable hepatocellular carcinoma, compared with TACE alone.
Methods:
This was a single-center study, retrospectively recruited 82 unresectable HCC patients who received either TACE alone (TA group; n = 46) or TACE combined with anlotinib (TC group; n = 36) between Jan 2018 and Jan 2019. The primary outcomes were progression-free survival (PFS) and overall survival (OS). While the secondary outcomes were the objective response rate (ORR), the disease control rate (DCR), and main complications. Log-rank test and Kaplan–Meier method was used to calculate the survival difference. All statistical tests were 2-sided and P value <0.05 were taken as statistically significant.
Results:
Patients in TC group had a significant higher PFS than those in TA group (7.35 months vs. 5.54 months, p = 0.035). Although 3-month survival rate in the 2 groups was not statistically different (97.2% vs. 93.5%, p = 0.627), the survival rate at 6 months and 1 year were strongly higher in TC group (83.3% vs. 56.5%, p = 0.016; 66.7% vs. 19.6%, respectively, p < 0.05). Furthermore, there was a significantly higher ORR in TC group, while no statistical difference existed in DCR. Neither treatment-related mortality nor grade 4 adverse events (AEs) occurred. However, 2 patients in TC group had grade 3 AEs (one suffered with erythra, and the other with hand-foot-skin reaction), which disappeared after prompt treatment.
Conclusion:
TACE combined with anlotinib is safe and may improve outcomes for unresectable HCC patients comparing with TACE alone. Randomized controlled trials are warranted to further evaluate treatment effects of anlotinib in HCC.
Keywords
Introduction
Hepatocellular carcinoma (HCC), which composes about 65% of all liver cancers, is among one of the leading causes of cancer-related death. 1 -3 Together with lung cancer, HCC is the most common cancer happened in Chinese population. 4 There are a variety of treatment options for HCC, including surgery, liver transplantation, molecular-targeted therapy, local-regional therapies, and immunotherapy. 5 Traditionally, only surgery and transplantation are taken as curative options for HCC patients. However, curative resection or transplantation was not suitable for the majority of HCC patients when diagnosed, considering the tumor size, number, location, vascular involvement, extrahepatic metastases, liver function, and patients’ general condition. 6 -8 Therefore, it is extremely urgent to develop an effective therapy for unresectable HCC.
In recent years, local-regional therapies, including transarterial chemoembolization (TACE) and radiofrequency ablation have been regarded as optimal therapies for HCC patients. 9,10 TACE has been generally recommended as the standard palliative therapeutic regimen by guidelines and expert consensus for unresectable HCC. 11 -13 However, comparing with the other treatment options, such as chemotherapy, molecular targeted therapy or immunotherapy, TACE displays limited benefits. 14 -16 Two main reasons may contribute to the unsatisfactory effects. First, TACE, especially after incomplete embolization, may leads to the regaining of vascular supply of nutrients and oxygen to residual tumors. Second, TACE can’t prevent recurrence and metastasis of the tumor effectively. After interdicting the blood supply of tumor, the increased level of HIF (hypoxia-inducible factor) will promote the release of VEGFR sequentially, which may facilitate the recurrence and metastasis of tumor. 17
A multidisciplinary approach is needed for HCC patients to obtain optimal outcomes. 18 Therefore, TACE should be combined with other treatment regimens to improve clinical efficacy. It has been reported that TACE combined with tyrosine kinase inhibitors (TKIs), for example, sorafenib or lenvatinib can been applied in patients with unresectable HCC. 19 Anlotinib, a novel TKI, is used as a third-line treatment agent for patients with advanced non-small cell lung cancer, approved by Chinese Food and Drug Administration (CFDA) on May, 2018. 20,21 However, the treatment efficacy and safety of anlotinib in HCC patients is still undetermined.
Based on the above findings, the study aimed to evaluate the efficacy and safety of using TACE combined with anlotinib in unresectable HCC patients, comparing to TACE alone.
Methods
Patients
We recruited unresectable HCC patients who underwent either TACE alone or a combination of TACE and anlotinib thorugh January 2018 to January 2019 at the First Affiliated Hospital, Sun Yat-sen University, retrospectively. The Unresectable HCC includes one or more aspects as following: i) residual liver volume is insufficient, ii) distant metastasis or great vascular invasion, iii) liver function or physical condition is poor, iv) resection is highly risky assessed by 2 experienced surgeons. Among 82 patients included, 46 received TACE alone (TA group), while 36 received TACE combined with anlotinib (TC group). The eligibility of each participant was confirmed, using the following inclusion criteria: (1) Diagnosed HCC using noninvasive criteria, which is consistent with the European Association /American Association guidelines for Liver Disease or pathological diagnosis; (2) HCC deemed to be unresectable or incurable after multidisciplinary treatments; (3) Liver function, class A or B of Child-Pugh; (4) Performance score of Eastern Cooperative Oncology Group (ECOG) <2; (5) Available of complete medical records, including imaging (enhanced computed tomography [CT) and/or magnetic resonance imaging [MRI)), and prognostic data. Exclusion criteria were prior therapy or contraindicated to receive TACE or targeted therapy. The study had obtained approval from the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University. And written informed consent was obtained from all recruited patients.
Treatment Methods
All patients included in the study received treatment of TACE. The tip of the catheter was inserted into the artery branches for tumor-feeding according to tumor size, location, and arterial supply. Embolization was firstly performed using different kind of diameter microsphere, followed by an infusion of 20 mg of pharmorubicin, and finally embolizing trunk with absorbable gelatin sponge. The TC group was initially administered with oral anlotinib (12 mg) once each day (2-week on/1-week off) during 3 to 5 days after the first session. Patients would continue to take anlotinib before or after repeated TACE. If grade 1/ 2 adverse events (AEs) occurred, based on National Cancer Institute Common Terminology Criteria for Adverse Events, 22 the frequency and dose wouldn’t be adjusted, but the side effects must be dealt as soon as possible. If grade 3 AEs or above took place, the dose would be reduced to 8 mg once a day, or the frequency reduced to every 2 days until the AEs were eliminated or alleviated. If these AEs persisted, anlotinib therapy would be halted until they were alleviated or disappeared.
One treatment cycle was 4 weeks. Contrast-enhanced CT or MRI was examined every 4 weeks to assess treatment efficacy. Besides, ECOG scores, biochemical and serum α-fetoprotein measurements would be measured and recorded. TACE would be repeated according to the results of clinical judgment and residual lesions.
Efficacy and Safety Assessments
The modified Response Evaluation Criteria in Solid Tumors (RECIST 23 ) was used to explore the response to the treatments. The target lesions for each patient were independently evaluated by 2 radiologists and 1 interventional clinician. Any disagreement would be resolved to reach an agreement after reviewing the contrast-enhanced CT and/or MRI images.
Progression-free survival (PFS) was estimated according to the time duration between initial therapy and progression. Overall survival (OS) was defined as time length from initial therapy to death, or last hospital visit data. The objective response rate (ORR) was calculated as the percentage of both complete and partial response, maintained for at least 8 weeks among all cases. The disease-control rate (DCR) was the percentage of patients with stable disease, or complete/ partial response. PFS and OS (including survival rate at 3-month, 6-month, and 1-year) between TC group and TA group were compared. Besides, the overall response rate including ORR and DCR was evaluated as well.
Safety was evaluated by physical examination, vital signs, clinical laboratory results, and AEs.
Statistical Analysis
Student test was used to compare the continuous data, and Chi-square test was used for categorical variables. The results were presented with mean ± standard deviation (SD) or median (intervals). A life-table method was used to calculate PFS, with the Mantel-Cox test for further comparison. Log-rank test and Kaplan–Meier method was used to calculate the survival difference. All statistical tests were 2-sided and P value <0.05 were taken as statistically significant. Statistical analyses were conducted with SPSS 20.0.
Results
Patient Characteristics
Among all the 82 patients, the baseline characteristics in the 2 groups had no significant difference, as showing in Table 1. In this study, the median follow-up time was 13.76 months, ranging from 2 to 20 months. A total of 54 patients (65.9%) died during follow-up time.
Baseline Demographics, Disease Characteristics and Treatment.
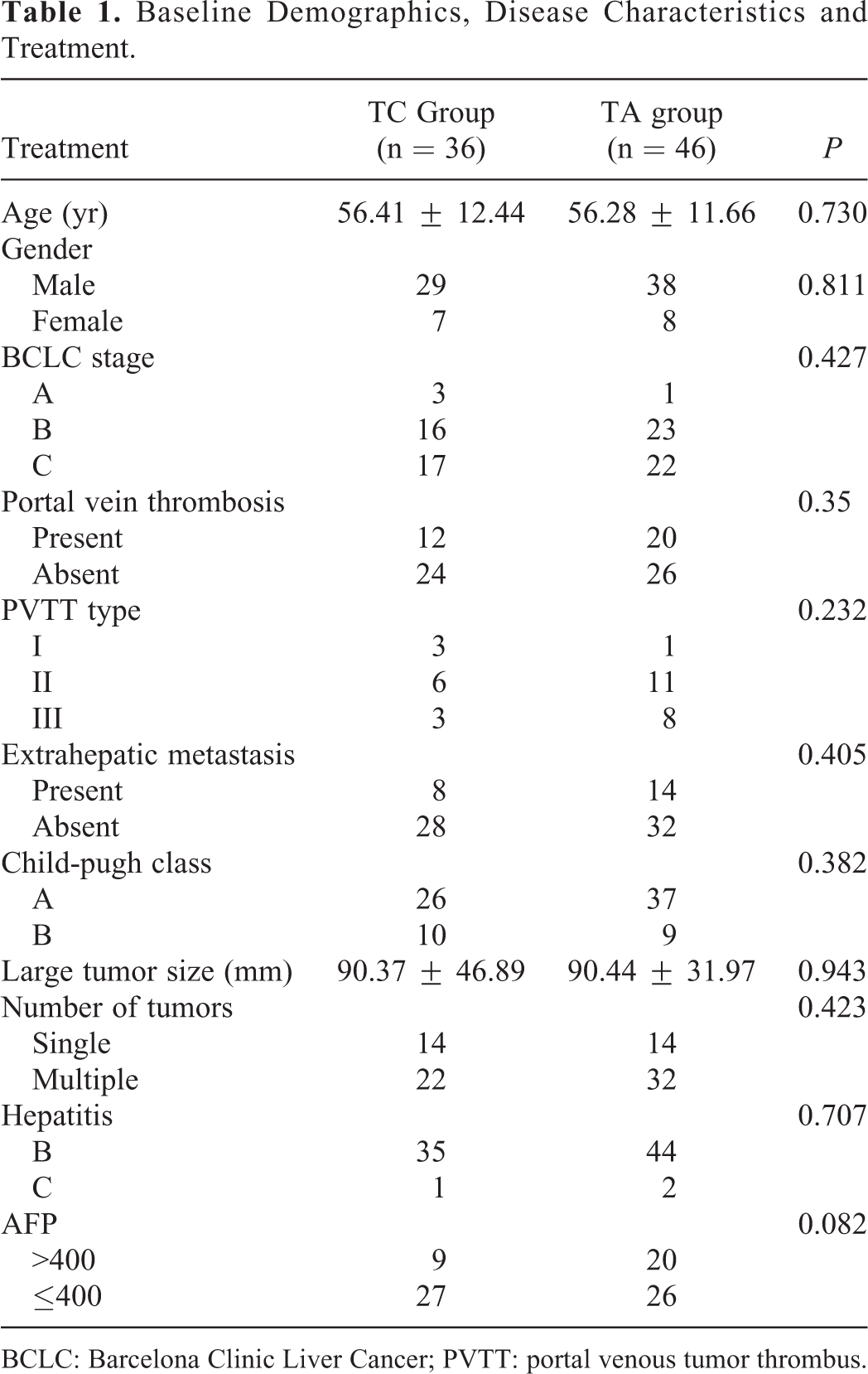
BCLC: Barcelona Clinic Liver Cancer; PVTT: portal venous tumor thrombus.
PFS and OS
Comparing with TA group, patients in TC group had a significant longer PFS (7.35 vs. 5.54 months, p = 0.035; Figure 1). Although no significant difference on 3-month survival rate (97.2% vs. 93.5%, p = 0.627; Table 2), the survival rates at both 6 months and 1 year in TC group were strongly higher than those in TA group (83.3% vs. 56.5%, p = 0.016; 66.7% vs. 19.6%, p < 0.01; Table 2).

Progression-survival in unresectable HCC patients treated with TACE combined and anlotinib (TC group) and TACE alone (TA group).
3 Month, 6 Month and 1 Year Month Survival Rate in TC and TA Group.
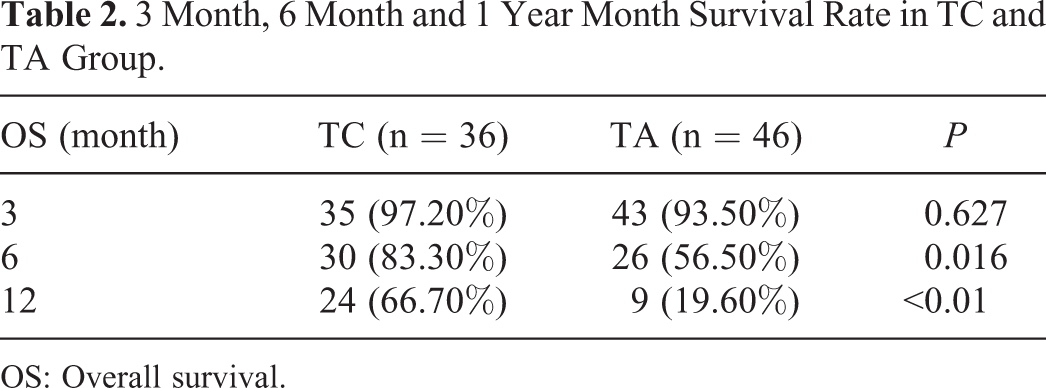
OS: Overall survival.
Overall Response to Treatment
Regarding to the overall response to treatments, complete response, partial response, stable disease, and progressive disease were 5 (13.9%), 23 (63.9%), 6 (16.6%), and 2 (5.6%), respectively in TC group, and 5 (10.9%), 10 (21.7%), 23 (50.0%), and 8 (17.4%) in TA group. In addition, ORR in TC group was significantly higher than TA group (77.8% vs. 32.6%, p < 0.01; Table 3). While, the 2 groups showed no statistical difference in DCR (94.4% vs. 82.6%, p = 0.17; Table 3).
Overall Response to Treatment in TC and TA Group.

CR: complete response; PR: partial response; SD: stable disease; PD: progressive disease;
DCR: disease control rate; ORR: objective response rate; TACE: transarterial chemoembolization.
Adverse Events (AEs)
AEs related to treatment in TC group were as followings: hand-foot-skin reaction (n = 17, 47.2%), hypertension (n = 10, 27.8%), erythra (n = 8, 22.2%), proteinuria (n = 5, 13.9%), hypothyroidism (n = 3, 8.3%), hypoproteinemia (n = 2, 5.6%), and pharyngolaryngeal pain (n = 1, 2.8%). Most AEs were regarded as grade 1 or 2. Grade 3 AEs occurred only in 2 patients. One was suffered with erythra, and another suffered with hand-foot-skin reaction. There was no grade 4 AEs occurred. All AEs were relieved after treatment or dose adjustment, and all participants continued the treatment and received follow-up evaluation. The most common AEs related to TACE were fever, mild epigastric pain, and nausea in TC group and TA group, respectively, all relieved at first week after appropriate treatments. The AEs had no statistic difference between the 2 groups.
Discussion
We found that comparing to using TACE alone, the combination therapies (TACE combined with anlotinib) were correlated with improved PFS and OS in unresectable HCC patients.
Although the management of HCC has been greatly improved in recent years, 24 curative therapies including surgery and liver transplantation can only be used in less than 30% of HCC patients. 25,26 As the change of concept and progress of treatment method, the first-line therapy for unresectable HCC includes TACE, targeted monotherapy or combination therapy. 27 -29 In recent years, TACE combined with targeted therapy are more extensively applied in clinical practice. As one systematic review reported, the ranges of OS achieved is 5.1 to 17 months using TACE alone, 30 and 7.5–27 months using a combination of TACE and sorafenib in unresectable HCC patients. Meta-analyses showed that compared with TACE mono-therapy, it combined with sorafenib was significantly associated with longer TTP for unresectable HCC.
There are 5 molecular-targeted agents (MTAs) for HCC, sorafenib and lenvatinib still served as the first-line agents, while the second-line agents include regorafenib, cabozantinib and ramucirumab. 31 However, considering the high cost of sorafenib or lenvatinib, it is therefore necessary to identify efficient and safe treatments for patients with advanced HCC in China.
Anlotinib is an innovative anticancer drug, which is regarded as more effective and safer. 20 Recent exploratory studies of anlotinib suggested that it was effective in a variety of tumors, with moderate AEs. However, no studies have evaluated the outcomes of using anlotinib combined with TACE in unresctable HCC patients. This study suggested that anlotinib plus TACE was effective in unresectable HCC patients, with PFS and 1-year survival rate of 7.35 months and 66.7%, respectively. And PFS and OS were longer than those with TACE alone.
Similar to other MTAs, anlotinib has many potential adverse reactions. However, there was no serious AEs reported in this study. The most frequent AEs observed were hand-foot-skin reaction and erythra, common for all TKIs. Other AEs, including proteinuria, hypothyroidism, hypoproteinemia and pharyngolaryngeal pain were less frequent, but caused discomforts. Most AEs in this study were regarded as grade 1 or 2, which was well-tolerable and no need for drug reduction and suspension. In addition, Grade 3 AEs reduced to grade 1 after drug reduction or discontinuation.
This study had some limitations. First, as a retrospective study, potential confounders might influence the results. In this study, the baseline characteristics were well-balanced. Second, the sample size was relatively small in the study. Further evidence with larger sample size is warranted. Third, the follow-up time is relatively short, and a large proportion of patients were alive until now. Thus, it was impossible to analyze the overall survival between the 2 groups.
Conclusion
In summary, the combination of TACE and anlotinib was effective and safe for unresectable HCC patients. Furthermore, the side effects of TACE, combined with anlotinib were no more severe than those with lenvatinib or sorafenib. Considering a cheaper cost, comparing to other MTAs, anlotinib may be more cost-effective to Chinese HCC patients. Thus, TACE combined with anlotinib might be used as an alternative treatment modality for unresectable HCC. Randomized controlled trials with large sample size are warranted to urther confirm the findings.
Footnotes
Authors’ Note
The study had obtained approval from the Ethics Committee of the First Affiliated Hospital of Sun Yat-sen University. {[2019]239}.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.