
Abstract
Keywords
Introduction
Globally, and in particular China, the prognosis of patients with hepatocellular carcinoma (HCC) remains depressed. It is currently one of the most frequent tumors in the world and the second commonest cause of cancer-related death. 1 Due to insufficient liver reserve and donor shortage, some curative methods, such as hepatectomy and liver transplantation, are only suitable for a small number of patients. 2 As a result, only <30% of HCC patients can benefit from curative therapies. 3 Currently, transarterial chemoembolization (TACE) as a palliative therapy has been recognized as the most commonly used treatment for unresectable HCC. 4 However, some tumor cells may still survive after a session of TACE, and low rates of complete response (CR) after TACE have been reported, ranging from 23% to 27%.5, 6 Hence, repeated TACE procedure is the most commonly used method for local or intrahepatic residual HCC. 7
However, the efficacy of TACE decreases significantly as the number of TACE procedures increases, with rates of progressive disease (PD) after the first, second, third, and fourth TACE procedures reported to be 18%, 21%, 25%, and 27%, respectively. 8 Based on this phenomenon, the Japan Society of Hepatology (JSH) first proposed the concept of TACE failure/refractoriness in 2010, 9 and updated it in 2014. 10 It should be noted, however, that the JSH standard appears to be problematic because new intrahepatic tumors are far from the target territory, and while new intrahepatic tumors represent PD, additional TACE therapy is not contraindicated. Thus, a new concept, termed “untreatable progression (UP)” was proposed to determine TACE discontinuation,1,11,12 which includes both major progression (such as extensive hepatic involvement, extrahepatic metastasis, or vascular invasion) and minor intrahepatic progression associated with impaired liver function and performance status. Currently, for those patients who have UP after TACE, treatment is challenging and there is still no consensus, which may create an incentive to try other therapeutic approaches.
Immune checkpoint inhibitors (ICIs) that reverse immune exhaustion have been shown to be effective in HCC, when used alone and in combination with TACE in the treatment of intermediate and advanced HCC.13–15 Recently, camrelizumab, an anti-programmed cell death protein 1 monoclonal antibody, was approved in China as a second-line treatment for unresectable HCC. Camrelizumab has been shown to be comparable to the efficacy of nivolumab and pembrolizumab in the treatment of advanced HCC. 16 Accordingly, we hypothesized that camrelizumab may be effective in treating UP HCC after TACE, but no studies have been reported so far. Meanwhile, tumors with a low mutation burden and fewer neoantigens are generally less immunogenic, so they have little response to immunotherapy. TACE has been reported to promote tumor-specific CD8+ T cell response by killing HCC cells and causing the release of tumor-associated antigens. 17 Thus, the application of camrelizumab after TACE treatment may attain promising outcomes in UP HCC. However, to our knowledge, no studies have been reported on the treatment of UP HCC with camrelizumab, therefore, this study reports the safety and efficacy of camrelizumab in the treatment of UP HCC patients.
Material and Methods
Patients
A retrospective analysis was conducted of all consecutive HCC patients who received TACE plus camrelizumab at our institution between May 2019 and January 2021. The criteria for patient selection included (1) patients aged > 18 years with HCC confirmed by pathological or clinical diagnosis according to European Association for the Study of the Liver criteria 1 ; (2) patients who received additional camrelizumab due to UP after initial TACE treatment1,11,12; (3) Child–Pugh class A or B without ascites; and (4) an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Exclusion criteria were (1) concurrent ablation, resection, radiotherapy, or systemic therapies for HCC; (2) discontinuation of camrelizumab due to serious adverse events (AEs); (3) patients with main portal vein obstruction; and (4) loss to follow up.
All patient details in this study have been de-identified. The retrospective single-center study was conducted in accordance with the principles of the Declaration of Helsinki and all procedures performed in this study were approved by the Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (UHCT-IEC-SOP-016-03-01). The need for informed consent was waived by the local ethics committee and the institutional review board of the Huazhong University of Science and Technology because clinical data were analyzed retrospectively and anonymously. The reporting of this study conforms to STROBE guidelines. 18
TACE Procedure
TACE was performed according to institutional standard protocol. 19 In summary, after superselective catheterization of tumor-feeding arteries with coaxial microcatheter (Progreat, Terumo), a solution of multiple chemotherapeutic agents (epirubicin 40-60 mg, cisplatin, oxaliplatin, or lobaplatin 50-100 mg, and 5-Fu or floxuridine 1.0 g) or single chemotherapeutic agent (epirubicin 40-60 mg) with ethiodized oil was subsequently injected. This was followed by injection of gelatin sponge particles (350-560 or 560-710 μm, Alicon). Embolization was performed under fluoroscopic guidance until there was stasis of arterial flow. Hepatic artery angiography was then subsequently performed to confirm success of the embolization procedure.
UP after TACE was defined as progression associated with a clinical profile that prevents retreatment, which includes at least one of the following situations: Ib—targeted tumor failed to achieve objective response after at least 2 initial TACE treatments; II—local tumor progression or new intrahepatic tumor did not achieve objective response after another TACE session; III—presence of significant progression, including substantial liver involvement, vascular invasion, or extrahepatic metastasis; and then IV—presence of hepatic dysfunction (Child–Pugh C) or ECOG performance status > 2 that contraindicates TACE therapy. 11
Camrelizumab Therapy
The administration of camrelizumab was initiated after UP in HCC patients. Camrelizumab was administered intravenously at a dose of 200 mg every 3 weeks. If patients developed serious AEs, the drug was interrupted or discontinued and symptomatic treatment such as glucocorticoids or immunosuppressant agents were administered, depending on the severity and the affected organs. For patients who required multiple TACE procedures, the camrelizumab was administered within 2 weeks after TACE.
Follow up and Evaluation
All patients were followed up until June 2021. Laboratory examinations, abdominal contrast-enhanced computed tomography (CT) or MRI) were performed every 6 to 8 weeks after initial camrelizumab treatment. Laboratory tests mainly included routine blood tests, cardiac, liver, and renal function tests. Follow-up CT or MRI at 2 to 3 and 6 months after initial camrelizumab treatment were compared with pretreatment imaging to determine objective response rate (ORR) and disease control rate (DCR) according to Modified Response Evaluation Criteria in Solid Tumors (mRECIST). 20 ORR was defined as a CR or partial response (PR). DCR represented CR, PR, or stable disease (SD).
Progression-free survival (PFS), defined as the time interval from initial camrelizumab treatment to the date of progression for patients who displayed radiological evidence of disease progression or the date of death or last follow up, was the primary endpoint of this study. AEs were recorded and assessed by the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. In addition, postembolization syndrome, such as fever, pain, nausea, and vomiting, is not considered as an AE in itself, but rather as an expected outcome of embolization therapy. 21
Statistical Analyses
All analyses were performed using SPSS software, Version 24.0 (IBM). Discrete variables were presented as numbers with percentages, and quantitative data were presented as mean ± standard deviation. PFS were calculated using Kaplan–Meier method. The 95% confidence interval (CI) was calculated for median PFS and hazard ratio (HR). Risk factors for PFS were evaluated with logistic regression analysis. All statistical tests were two-tailed and P < .05 indicated statistical significance.
Results
Patient Characteristics
A total of 89 HCC patients received additional camrelizumab due to UP after initial TACE treatment in our hospital between May 2019 and January 2021. Of those, 28 were excluded due to concurrent ablation, resection, radiotherapy, or systemic therapies, 11 were excluded due to camrelizumab discontinuation, and 9 patients were excluded because they were lost to follow up. Eventually, 41 patients were included in this study (Figure 1). Situations I, II, and III of UP occurred in 11, 13, and 17 patients, respectively. A total of 150 TACE sessions were performed before the addition of camrelizumab, with a median TACE procedure of 3 (range: 1-19) per patient. The overall patient characteristics are shown in Table 1. In addition, 15 patients (36.6%) died during the observation period of the study.

Flowchart of the patients who were included in this study.
Patient Demographics and Clinical Status at Camrelizumab Initiation (n = 41) and Univariate Analysis of Prognostic Factors for Progression-Free Survival (PFS).
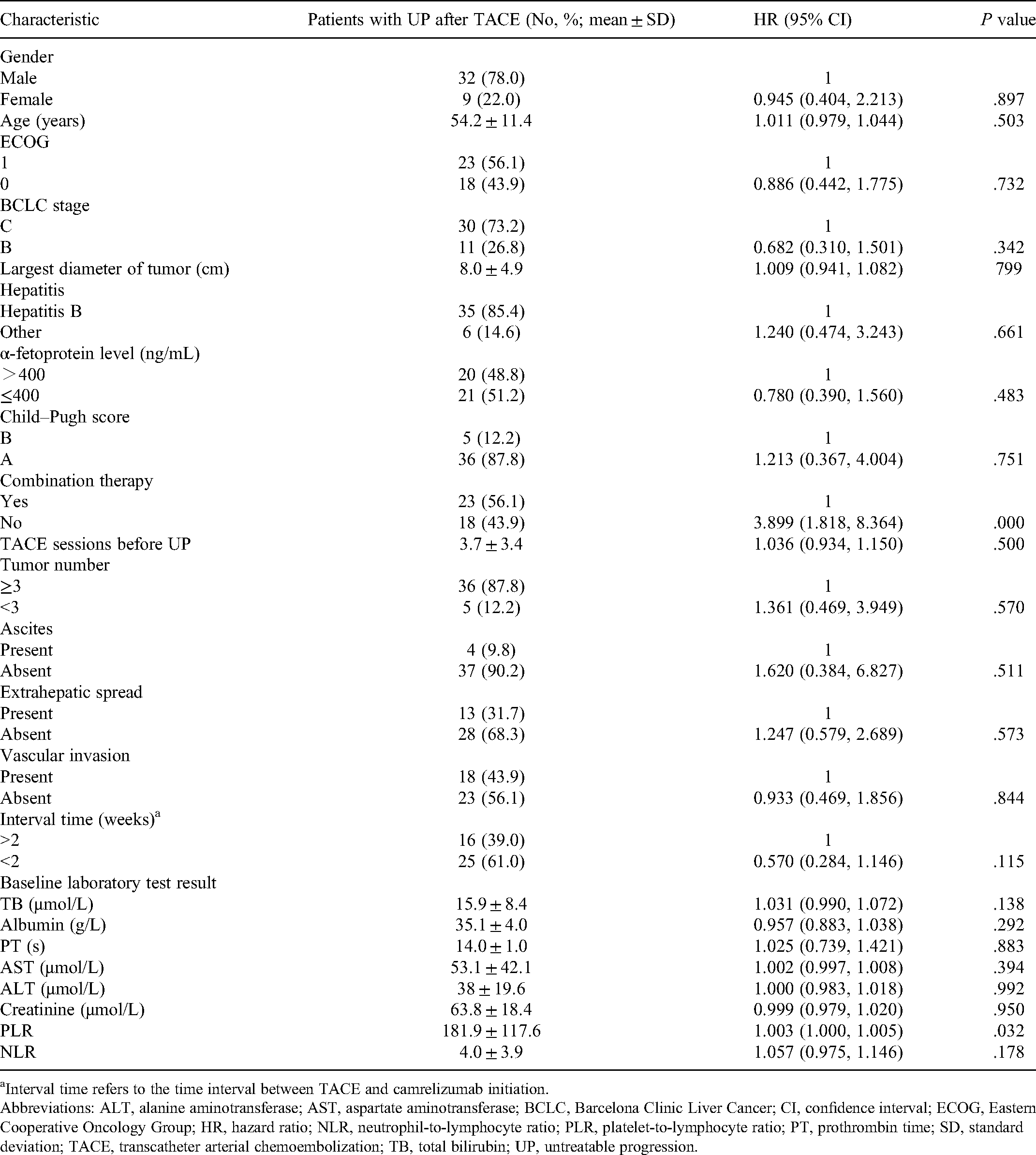
Interval time refers to the time interval between TACE and camrelizumab initiation.
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; PT, prothrombin time; SD, standard deviation; TACE, transcatheter arterial chemoembolization; TB, total bilirubin; UP, untreatable progression.
Addition of Camrelizumab to TACE
Forty-one patients received 280 camrelizumab therapy sessions, with a median of 5 sessions (range: 1-17) per patient. Twenty-three patients received camrelizumab combined with TACE (hereafter, camrelizumab–TACE), on whom 52 combined TACE procedures were performed, with a median of 2 procedures (range: 1-6) per patient. The remaining 18 patients received camrelizumab alone due to TACE contraindications.
Tumor Response
Imaging results 2-3 months after intervention indicated that 1 patient (2.4%) achieved CR, 9 patients (22.0%) achieved PR, and 15 patients (36.6%) achieved SD. Thus, the ORR is 24.4% and the DCR is 61.0%. Imaging results 6 months after intervention showed CR in 1 patient (2.4%), PR in 4 patients (9.8%), and SD in 19 patients (46.3%). Therefore, ORR was 12.2% and DCR was 58.5%.
PFS
The median follow-up period from camrelizumab initiation to the study’s endpoint was 7 months (range: 4-14 months). Of the 41 patients, 33 (80.5%) developed disease progression after addition of camrelizumab. The median PFS in this study was 6 months (95% CI: 3.8 months, 8.2 months) (Figure 2). Univariate analysis (Table 1) indicated that combination therapy and platelet-to-lymphocyte ratio (PLR) were significantly associated with PFS (P < .05). At multivariable analysis (Table 2), combination therapy (camrelizumab–TACE) was significantly associated with better PFS (P = .003).
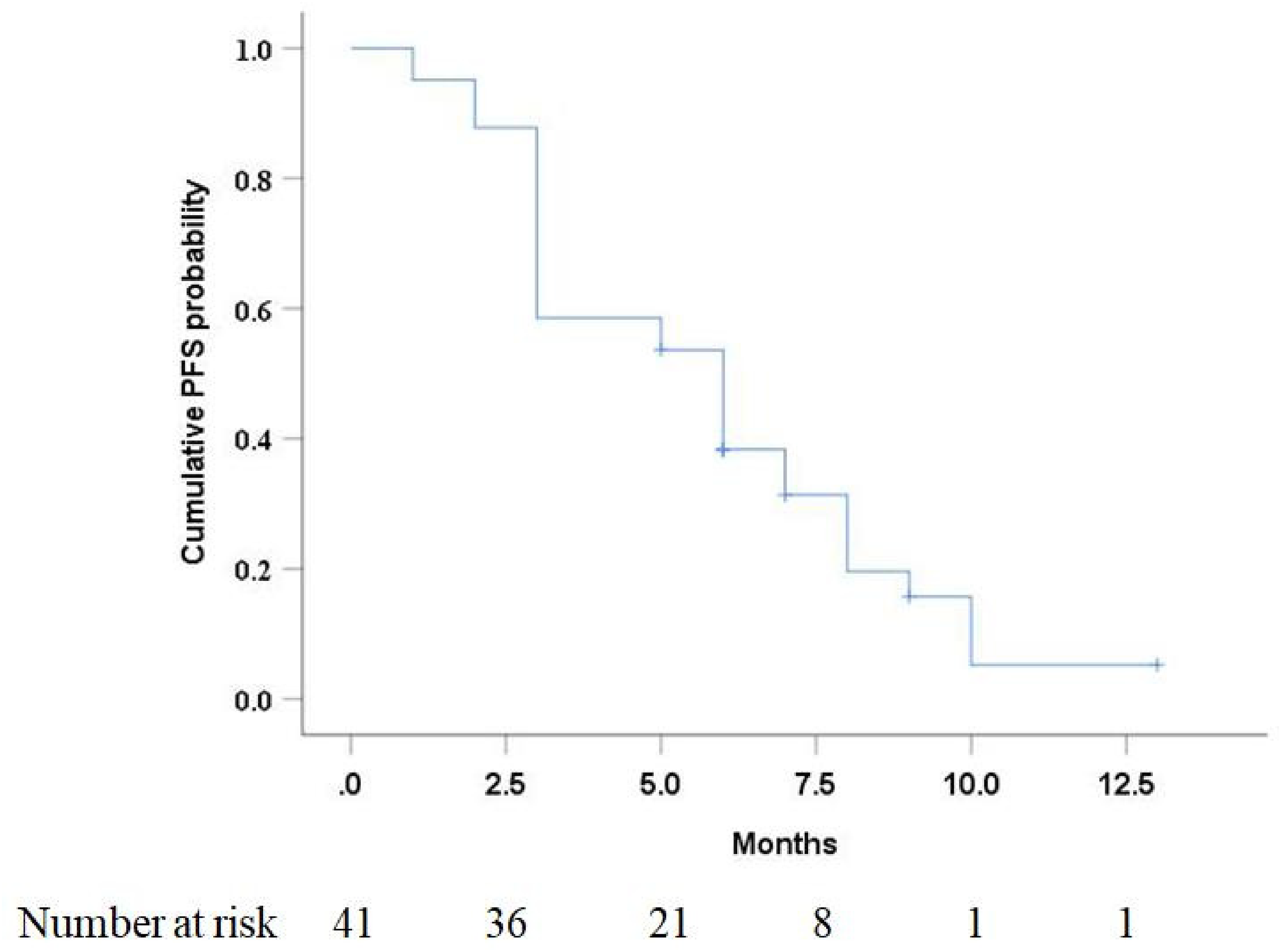
Kaplan–Meier curve of progression-free survival (PFS) in HCC patients with untreatable progression (UP) after TACE.
Multivariate Analysis of Prognostic Factors for Progression-Free Survival (PFS).

Abbreviations: CI, confidence interval; HR, hazard ratio; PLR, platelet-to-lymphocyte ratio.
AEs
Twenty-one (51.2%) patients developed postembolization syndrome, including fever (n = 18), abdominal pain (n = 15), nausea, and vomiting (n = 10) within 1 week after TACE. After symptomatic treatment during hospitalization, the symptoms of all patients were relieved or significantly improved. In addition, there were no TACE-related severe AEs such as liver abscess and biloma, and no allergic events occurred during camrelizumab injection.
During the follow-up period, 17 (41.5%) patients developed at least 1 type of AE after treatment with camrelizumab (Table 3), and no patients developed severe AEs (more than grade III). Grade I/II AEs included reactive cutaneous capillary endothelial proliferation (RCCEP) (n = 14), hypothyroidism (n = 6), asthenia (n = 2), rash (n = 1), myositis (n = 1), and pneumonitis (n = 1). Of note, 2 patients who developed pneumonia and myositis who received glucocorticoids and were temporarily interrupted from camrelizumab demonstrated significant improvement in symptoms, and then resumed camrelizumab therapy. No treatment-related mortalities occurred.
Adverse Events (AEs).

Abbreviations: CTCAE, Common Terminology Criteria for Adverse Events; RCCEP, reactive cutaneous capillary endothelial proliferation.
In addition, 3 patients were discontinued due to grade III AEs, including 2 patients who developed pneumonia and 1 patient who developed myocarditis.
Discussion
ICIs have made great progress in the field of HCC in recent years. The tumor microenvironment of HCC is infiltrated by different types of immune cells, including T cells, natural killer cells, etc. 22 Currently, the treatment of HCC patients with UP after TACE remains a crucial issue. Changes in T cell populations after TACE have been demonstrated, which provides impetus for the exploration of immunotherapy after TACE. 23 The present study indicated that additional camrelizumab therapy is effective and safe in the treatment of HCC patients with UP after initial TACE treatment.
Patients with HCC who develop UP after TACE treatment have a poor prognosis, and these patients are reported to be good candidates for tyrosine kinase inhibitors.24–26 Lee et al investigated 54 patients receiving sorafenib who met the criteria of TACE failure as defined by the European and Japanese International Guidelines and showed a median PFS of 3.2 months. 24 Similarly, another study 25 comparing sorafenib with hepatic arterial infusion of cisplatin in HCC patients who were refractory to TACE showed a median time to progression of 3.9 months for sorafenib and 2 months for cisplatin. In addition, the efficacy of lenvatinib in patients with intermediate-stage HCC refractory to TACE was reported by Shimose et al. 26 The median PFS in the lenvatinib group was 5.8 months, higher than that in the sorafenib group (3.2 months) and TACE group (2.4 months). However, the study only included patients with intermediate-stage HCC and lacked results for patients with advanced HCC. In this study, additional camrelizumab therapy achieved a median PFS of 6 months in patients with UP after TACE, which seems to imply that ICIs represent effective systemic therapy for patients with TACE failure.
In terms of tumor response, camrelizumab also had comparable outcomes for HCC with UP after TACE treatment. Previous studies have shown that nivolumab as the first-line and second-line treatments for advanced HCC patients has an ORR of 15% 27 and 20%, 13 respectively. Similarly, pembrolizumab as the first-line and second-line treatments for advanced HCC patients has an ORR of 17% 28 and 18.4%, 29 respectively. Meanwhile, the ORR of camrelizumab in advanced HCC patients who had failed chemotherapy or sorafenib treatment was 14.7%. 16 The results of this study showed that ORR and DCR were 24.4% and 61.0%, respectively, suggesting that camrelizumab therapy may achieve comparable tumor control in HCC patients with TACE failure.
In this study, multivariable analysis indicated that camrelizumab–TACE was an independent prognostic factor for PFS. Additional subgroup analysis demonstrated that the camrelizumab–TACE therapy significantly improved median PFS when compared with camrelizumab monotherapy. It is reported that TACE can promote tumor-specific CD8+ T cell response by killing HCC cells and causing the release of tumor-associated antigens. 17 As suggested by the theoretical advantages, both Zhan et al 15 and Marinelli et al 14 demonstrated the efficacy of transarterial embolization combined with ICIs in the treatment of HCC patients. Similarly, this study also confirmed that TACE combined with ICI was superior to ICI monotherapy. These outcomes should promote further prospective studies evaluating combination TACE and systemic immunotherapy for the treatment of HCC patients.
Recent studies have shown that the inflammation ratio of PLR may potentially serve as a quantitative biomarker for individual tumor characteristics.30,31 Schobert et al 32 investigated inflammatory biomarkers in patients with HCC treated with TACE and found that high baseline PLR predicted poorer tumor response and shorter PFS. Shen et al 33 and Fan et al 34 also reported that high PLR is associated with poorer overall survival (OS) and metastasis in HCC patients treated with TACE. In this study, although the univariate analysis showed that PLR was associated with PFS, multivariable analysis did not indicate that it was an independent prognostic factor affecting PFS. This may be related to the small sample size of this study. An additional study with larger sample size is warranted to validate risk factors to UP after TACE.
This study found that 39.6% of patients had AEs, but no patients of grade III or higher had AEs. Meanwhile, camrelizumab had a lower incidence of AEs in HCC patients with UP after TACE compared with sorafenib.25,35 Unlike nivolumab and pembrolizumab, RCCEP is more common after camrelizumab treatment. 36 RCCEP incidence after camrelizumab monotherapy has been reported in 76.7% to 97.3% in other tumors, but no grade III RCCEP was reported.29,37 Similar to the study by Qin et al, 16 the most common AE was RCCEP. However, the incidence of grade III or higher grade AEs with camrelizumab seemed to be lower than with other ICIs,14,15 suggesting that camrelizumab is safe for the treatment of HCC patients with UP after TACE.
The retrospective study had several limitations. First, the present study was conducted in a single institution with a small sample size, and therefore, a multicenter prospective randomized trial is needed. Second, most patients were still alive at the time of data collection and were followed up for a relatively short period of time and did not obtain the median OS for this study. Thus, it is necessary to explore the long-term efficacy on patients. Lastly, we did not include a control group of HCC patients with UP after TACE who received sorafenib or other forms of systemic therapies. Therefore, further comparative studies are needed to elucidate the clinical efficacy of camrelizumab in the treatment of HCC with UP.
Conclusions
The present study first reported camrelizumab in the treatment of HCC patients with UP after TACE, and the results indicated that camrelizumab has an acceptable safety profile and promising tumor control. Meanwhile, this study also demonstrated the superiority of camrelizumab–TACE verse camrelizumab monotherapy. The results of this study may prompt further prospective studies to evaluate the combination of TACE and ICIs in the treatment of HCC patients.
Footnotes
Abbreviations
Acknowledgement
The author(s) are very grateful to Ms. Tingting Qin for her help in the statistical analysis of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from National Nature Science Foundation of China (grant numbers 81771950, 81471765, and 81873919) and Fundamental Research Funds for the Central Universities (grant number 2021yjsCXCY101).
Ethics Approval
The retrospective single-center study was conducted in accordance with the principles of the Declaration of Helsinki and all procedures performed in this study were approved by the Ethics Committee of the local hospital (approval number UHCT-IEC-SOP-016-03-01). The need of informed consent was waived by the local ethics committee and the institutional review board of the Huazhong University of Science and Technology because clinical data were analyzed retrospectively and anonymously.