
Abstract
Background:
To investigate the pathologic complete response (pCR) rates of dual human epidermal growth factor receptor 2 (HER2) blockade in a neoadjuvant setting for HER2+ breast cancer.
Methods:
We searched randomized clinical trials (RCTs) using dual HER2 blockade in a neoadjuvant setting for HER2+ breast cancer in PubMed, the Cochrane Library, Embase and ClinicalTrials.gov up to July 5, 2020, and all included studies were assessed according to the Cochrane Collaboration tool for assessing the risk of bias of RCTs, and the statistical analyses were performed using STATA 14.0 software.
Results:
A total of 9 RCTs involving 2758 patients were included. Meta-analysis indicated that the pCR rates of lapatinib/pertuzumab/neratinib plus trastuzumab versus trastuzumab [relative risk (RR) = 1.31; 95% confidence interval (CI): 1.21-1.43; p < 0.001)] and lapatinib plus trastuzumab versus lapatinib (RR = 1.39; 95%CI: 1.25-1.53; p < 0.001) showed a significant statistical difference between dual HER2-blockade treatment and single-agent treatment in a neoadjuvant setting for HER2+ breast cancer. Additionally, there was no statistically significant difference in disease-free survival (HR = 0.72; 95% CI: 0.47-1.09; p = 0.123), incidence of serious adverse events (SAEs) (RR = 1.04; 95%CI: 0.81-1.33; p = 0.778) and cardiotoxicity(RR = 1.30; 95%CI: 0.81-2.08; p = 0.280), and the pCR rate was unaffected by hormone receptor status.
Conclusions:
The pCR rate of neoadjuvant dual-target therapy for HER2+ breast cancer was significantly higher than that of single-target therapy. Furthermore, the results indicated that the safety of dual-target therapy is similar to that of single-target therapy.
Introduction
Breast cancer is the most common malignant tumor in women worldwide, with 24 million new patients and 523,000 deaths annually. 1 Approximately 15% to 20% of breast cancers exhibit upregulated levels of HER2 2 (referred to as HER2+ breast cancer), a 185-kDa tyrosine kinase transmembrane receptor encoded by a gene located on chromosome 17q12-21.32. HER2 overexpression results in a highly invasive tumor and worse prognosis without appropriate treatment. For primary resectable HER2+ breast cancer, neoadjuvant anti-HER2 therapy has become a routine treatment, 3 with trastuzumab representing the first targeted anti-HER2 drug. 4 Other targeted anti-HER2 drugs include lapatinib, pertuzumab, neratinib, and so on. Lapatinib is a small-molecule tyrosine kinase inhibitor of the HER1 and HER2 receptors and that mainly inhibits signaling associated with downstream mitogen-activated protein kinase/extracellular signal-regulated kinase-1/2 and phosphoinositide 3-kinase/Akt pathways. Pertuzumab is a humanized monoclonal antibody that inhibits the formation of HER2–HER dimers. Trastuzumab is the cornerstone of HER2+ breast cancer anti-HER2 treatment, and despite significant effectiveness, there remain serious clinical problems, such as recurrence and metastasis and acquired resistance in HER2+ patients. 5 -11 In order to overcome resistance to trastuzumab, combined treatment with other anti-HER2-targeting drugs has become a new therapeutic strategy; however, the ability of neoadjuvant dual-blockade anti-HER2 therapy to produce significant clinical improvement remains controversial. 3
Here, we conducted a meta-analysis of neoadjuvant dual-blockade anti-HER2 drugs to comprehensively evaluate their clinical efficacy and safety in HER2+ breast cancer patients.
Materials and Methods
Search Strategy
We searched PubMed, the Cochrane Library, Embase and ClinicalTrials.gov up to July 5, 2020, using subject headings and random words. The search strategy included the following terms: breast cancer, receptor ErbB-2, trastuzumab, lapatinib, pertuzumab, neratinib and neoadjuvant chemotherapy. The search terms were linked with “AND” or “OR” respectively and followed the Cochrane Handbook by using a combination of subject terms and free words, with searches of the literature included.
Study Inclusion/Exclusion Criteria
Studies needed to meet the following inclusion criteria to be eligible for the meta-analysis: 1) randomized clinical trials; 2) studies of HER2+ breast cancer and neoadjuvant dual-blockade anti-HER2 therapy; 3) involvement of at least 2 treatment options; 4) inclusion of data related to pathologic complete response, progression-free survival, disease-free survival (DFS), overall survival, and safety. Exclusion criteria for literature included the following: 1) similar studies were repeatedly published; 2) studies did not include neoadjuvant therapy; 3) corresponding data could not be obtained directly or indirectly; 4) review articles, case reports, comments, or letters.
Quality Assessment
The quality of the literature was evaluated using the Cochrane bias risk-assessment tool, including use of the random-allocation method, allocation scheme hiding, the blind method, and assessment of the integrity of results data, selective report research results, and other sources of bias. Two investigators (Chaokun Wang, Jing Chen) independently assessed quality, and in the event of disagreement, decisions were made based on discussions or evaluation by a third investigator.
Data Extraction
Data extraction was performed independently by 2 individuals (Chaokun Wang, Jing Chen) and according to a pre-designed data-extraction sample table, with the results crosschecked. Disagreements were resolved through negotiation. Extracted data included study name and year, anti-HER2 treatment regimen, number of participants, hormone receptor status, total pCR rate, DFS, serious adverse events (SAEs), and cardiac adverse events.
Statistical Analysis
Meta-analysis was performed using STATA 14.0 software (Stata Corp, College Station, TX, USA). Heterogeneity between analytical studies was performed using the Cochrane Q test and the I2 statistic. In cases of no heterogeneity between results (p > 0.05; I2 < 50%), a fixed-effects model was used. 12 In cases where heterogeneity existed between results (p < 0.05; I2 > 50%), a random-effects model was used. In cases of statistical heterogeneity between results (p < 0.05; I2 > 50%), the source of heterogeneity was be explored, and subgroup or sensitivity analysis was performed, as necessary. Publication bias was examined by a funnel plot. A p < 0.05 was considered statistically significant.
Results
Included Studies
We selected a total of 805 articles databases through systematic searches and screening, initially identifying 697 articles after remove duplicates, with 78 articles identified by study titles and abstracts. Eight of these studies were reviews, with 53 articles not meeting the inclusion criteria. Seventeen articles 13 -29 were obtained following a review of the entire text, with one representing a meeting abstract (TRIO-US B07) 13 and the remaining RCTs. Through detailed reading, it was found that 6 literatures had the same study population, so they were excluded. A total of 11 13,15 -19,23,26 -29 papers were included in the study. The detailed process is shown in Figure 1.

Flowchart describing study selection for the meta-analysis.
Study Characteristics and Quality Assessment
Of the 11 articles included, the NeoALTTO study included 4 articles, of which the pCR rate was mainly reported in 2012, others studies mainly reported long-term survival, adverse events and secondary analysis, which were determined as different populations. Among the remaining 10 articles, the NBRST, NeoSphere and PEONY studies reported the results of pertuzumab plus trastuzumab dual HER2-blockade therapy versus single-targeted therapy. The NSABP FB-7 study reported the results of neratinib plus trastuzumab versus trastuzumab single-targeted therapy, and the remaining 7 studies involved lapatinib plus trastuzumab therapy single-target dual HER2-blockade therapy as compared with single-targeted therapy. Information regarding the included studies is shown in Table 1. Quality evaluation was performed according to the PRISMA scale. Because the TRIO-US B07 abstract was a summary of the meeting, bias evaluation was uncertain, whereas the results for the remaining studies indicated high-quality studies with low bias. The detailed evaluation results are shown in Figure 2.
Characteristics of the Studies Used for Meta-Analysis.

Abbreviations: DC: Docetaxel-Carboplatin; AC: Doxorubicin-Cyclophosphamide; FEC: Fluorouracil-Epirubicin-Cyclophosphamide; H, trastuzumab; L, lapatinib; P, pertuzumab; N, neratinib; HR+, hormone receptor positive; HR−, hormone receptor negative; pCR, pathologic complete response; tpCR total pathologic complete response; DFS, disease-free survival; NA, not available; SAE, serious adverse events.

Quality assessment of the included studies.
PCR After Different Anti-HER2 Therapy
The pCR results for lapatinib, pertuzumab or neratinib combined with trastuzumab as compared with trastuzumab treatment are shown in Figure 3. The results indicated that the RR value of the pCR of dual HER2-blockade therapy was 1.31 (95% confidence interval: 1.21-1.43; p < 0.001), which differed significantly from that of single-agent treatment.
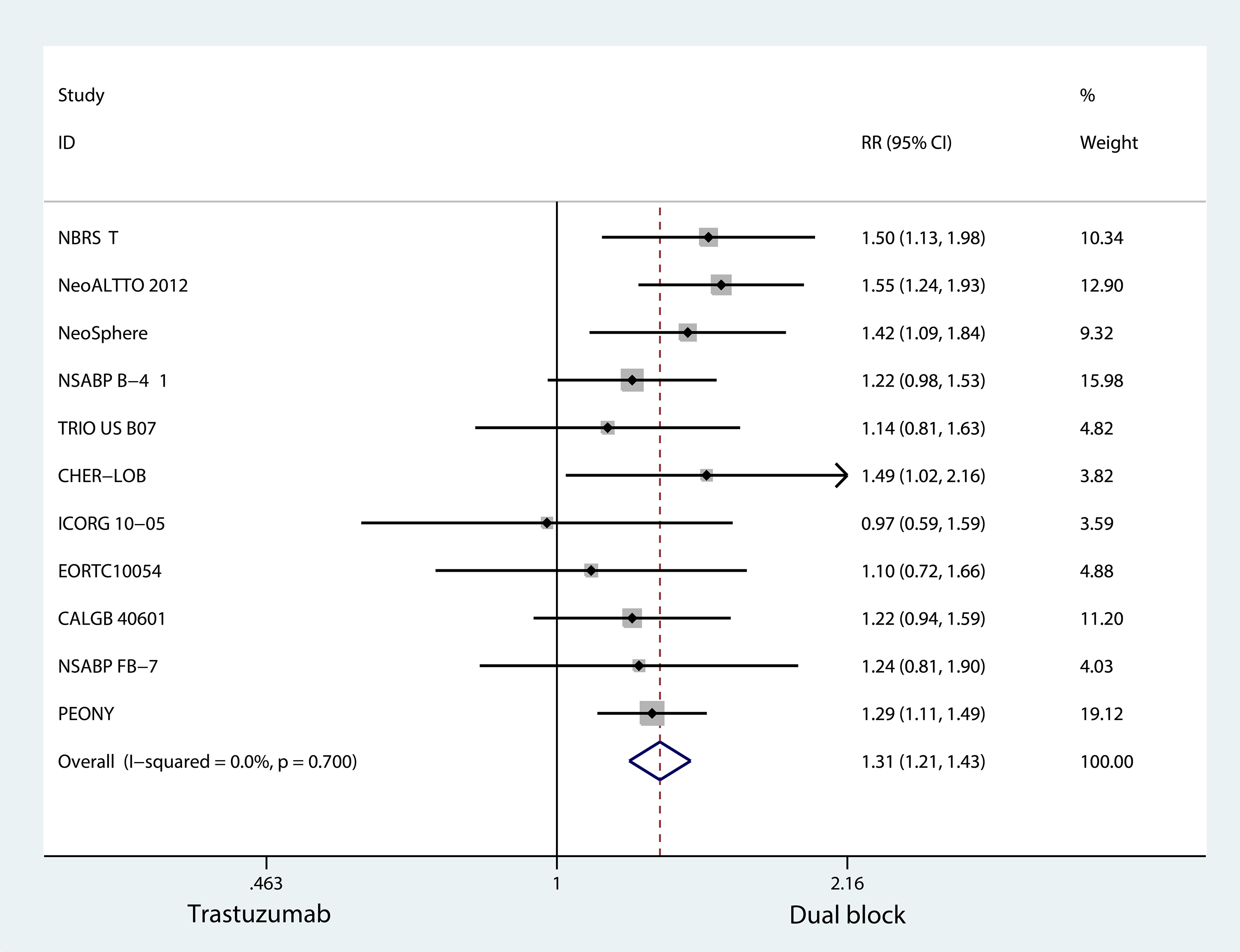
Forest plots of RR for dual block versus single-agent trastuzumab in HER2+ breast cancer women in the neoadjuvant.
The RR for pCR in the lapatinib combined with trastuzumab group relative to the lapatinib group was 1.39 (95%CI: 1.25-1.53; p < 0.001), which differed significantly from that of single-agent treatment (Figure 4).

Forest plots of RR for dual blockade versus single-agent lapatinib treatment in HER2+ breast cancer patients receiving neoadjuvant therapy.
Hazard Rates for DFS
Figure 5 shows the DFS results of lapatinib or pertuzumab combined with trastuzumab treatment as compared with trastuzumab treatment alone. The results suggested that the hazard ratio (HR) for DFS following dual HER2-blockade treatment was 0.72 (95% CI: 0.47-1.09; p = 0.123) as compared with that of trastuzumab treatment alone.

Forest plots of DFS for dual blockade versus single-agent trastuzumab treatment.
Analysis of Adverse Events
The forest plot of SAE outcomes for lapatinib or pertuzumab combined with trastuzumab dual-targeted therapy as compared with trastuzumab alone is shown in Figure 6A. The results showed that SAE incidence and resistance to treatment following dual targeted therapy had an RR value of 1.04 (95%CI: 0.81-1.33; p = 0.778). Figure 6B shows the forest plot for cardiotoxicity related to lapatinib or pertuzumab combined with trastuzumab treatment as compared with trastuzumab treatment alone. Due to the heterogeneity of the 6 included literatures (I2 = 65.1%, p = 0.014), the random effect model was adopted for analysis. The results showed an RR value for dual HER2-blockade therapy plus trastuzumab treatment of 1.30 (95%CI: 0.81-2.08; p = 0.280).

A, Forest plots of SAEs associated with dual blockade versus single-agent trastuzumab treatment. B, Forest plots of cardiotoxicity incidence associated with dual blockade versus single-agent trastuzumab treatment.
Subgroup Analysis
To clarify differences of pCR between targeted therapies involving lapatinib, pertuzumab or neratinib combined with trastuzumab and trastuzumab alone, we performed subgroup analysis between treatment groups (lapatinib + trastuzumab, pertuzumab + trastuzumab). The results showed that compared with trastuzumab treatment alone, the RR for dual HER2-blockade treatment of pCR with lapatinib was 1.30 (95%CI: 1.28-1.14; p < 0.001), whereas that with pertuzumab was 1.37 (95%CI: 1.21-1.55; p = 0.001) (Figure 7A). Additionally, we performed subgroup analysis to clarify the relationship between hormone receptor (HR) status and therapeutic effect, finding that HR+ status resulted in an RR value for pCR treatment using dual HER2-blockade therapy relative to trastuzumab treatment alone of 1.23 (95%CI: 1.09-1.38; p = 0.001), whereas in cases of HR− status, the RR value was 1.53 (95%CI: 1.34-1.76; p < 0.001). Similarly, for pCR treated with dual HER2-blockade therapy as compared with lapatinib treatment alone, HR+ status returned an RR value of 1.28 (95%CI: 1.11-1.49; p < 0.001), whereas that for HR− status was 1.65 (95%CI: 1.35-2.02; p = 0.001) (Figure 7B, C).

A, Subgroup analysis of dual blockade versus single-agent trastuzumab treatment. B, Subgroup analysis of dual blockade versus single-agent trastuzumab treatment according to HR status. C, Subgroup analysis of dual blockade versus single-agent lapatinib treatment according to HR status.
Publication Bias
To assess the publication bias in this meta-analysis, as shown in Figure 8, evaluation of publication bias revealed no significant publication bias among the included studies(p = 0.404).
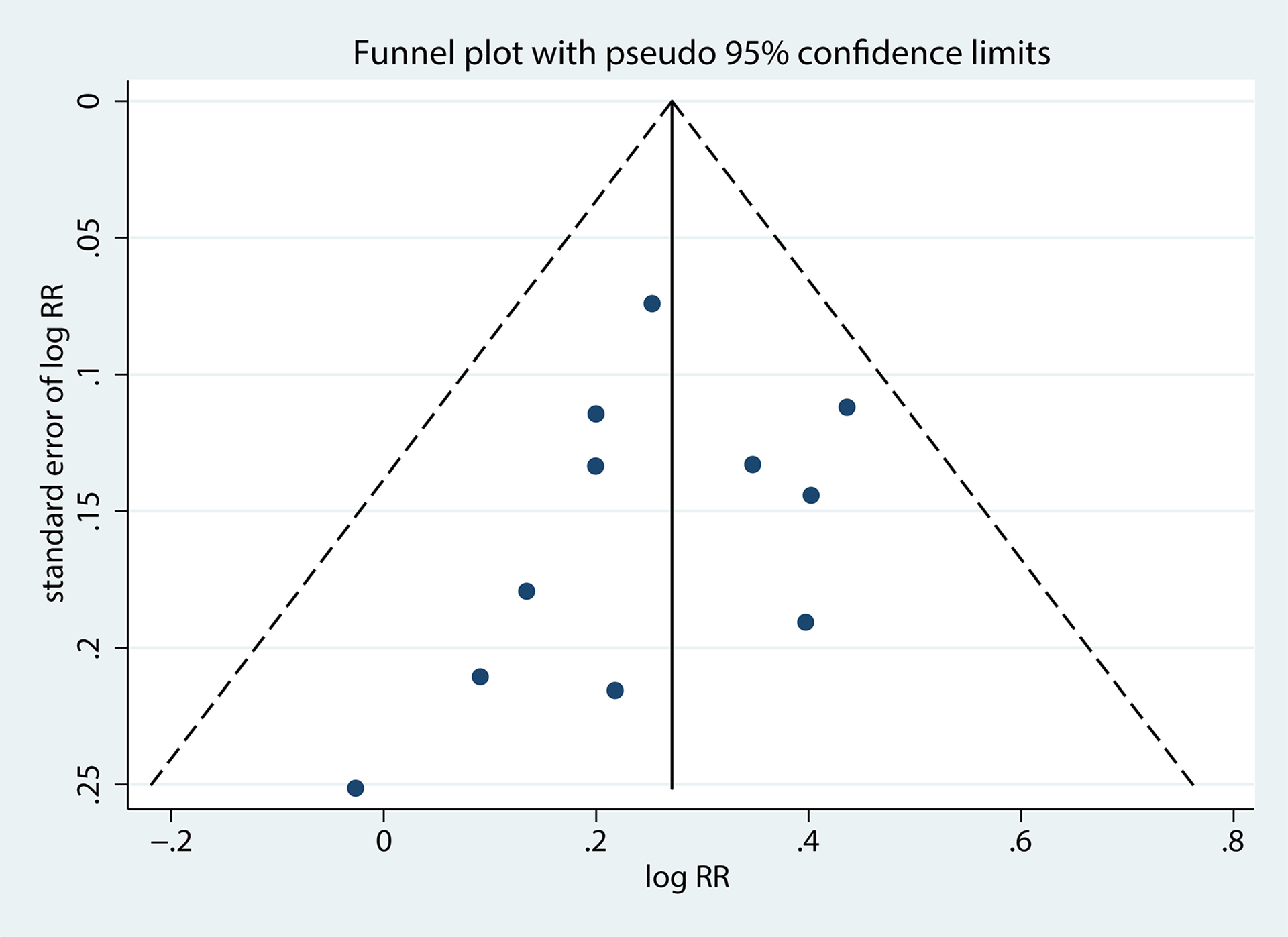
Funnel plot evaluating publication bias.
Discussion
HER2 is a tyrosine kinase transmembrane receptor and an important marker of tumor invasion and poor prognosis. As a therapeutic target, its status affects breast cancer classification, risk assessment, and treatment strategies. 30 Moreover, as a tyrosine kinase receptor, HER2/HER1 [also known as epidermal growth factor receptor (EGFR)] and HER3/HER4 can form dimers to play a key role in activating intracellular signaling pathways associated with breast cancer progression. Trastuzumab inhibits the cleavage of HER2 and specifically binds to the extracellular segment, thereby blocking the formation of HER2 homologous dimers, whereas pertuzumab prevents the formation of HER2/HER3 dimers by anchoring to HER2 domain two. The characteristics of different targets of these 2 drugs provide a complementary mechanism for dual-target therapy. Unlike trastuzumab, as a small-molecule EGFR tyrosine kinase inhibitor, lapatinib blocks ligand-induced heterodimeric signaling. These characteristics provide a molecular basis for dual HER2-blockade therapy. 31 Numerous studies have focused on dual HER2-blockade therapy in a neoadjuvant setting of breast cancer 32 -35 ; however, their results are inconsistent, especially in aspects of long-term survival and adverse drug reactions. Therefore, in the present study, we systematically searched and screened high-quality studies to evaluate the therapeutic effects, long-term survival status, and adverse reactions associated with dual HER2-blockade therapy relative to single-target therapy in neoadjuvant settings of breast cancer.
This meta-analysis suggested dual anti-HER2 therapy can improve the pCR rate in neoadjuvant chemotherapy for HER2+ breast cancer. However, in terms of long-term survival, there was no statistically significant difference in DFS (HR = 0.72; 95% CI: 0.47-1.09; p = 0.123), since in many of these included studies the primary outcome was pCR rate, survival analysis was not the main objective. Further investigations are needed to determine whether dual HER2 blockade therapy can improvement long-term survival benefits.
Of the 11 included studies, one was an abstract from the TRIO-US B07 meeting, and the rest were reports from high-quality RCTs. Subgroup analysis of combined-drug therapies revealed that compared with trastuzumab treatment alone, combined therapy with lapatinib or pertuzumab increased the pCR rate by 28% and 37%, respectively, suggesting that combined treatment with pertuzumab might be efficacious than that with lapatinib. However, this result was not statistically significant; therefore, further studies is needed.
Another key factor effecting clinical treatment strategies is the HR status. In clinical studies, it has been demonstrated that HR− breast cancer patients are more likely to benefit from dual HER2 blockade therapy. However, our findings are inconsistent with previous research, our results suggested that hormone receptor status and dual HER2 blockade therapy had no significant effect on the outcome. Many neoadjuvant clinical trials have demonstrated that dual HER2 blockade (trastuzumab plus neratinib, trastuzumab plus lapatinib, trastuzumab plus pertuzumab) increase the pathologic complete response rate. Nevertheless, the efficacy of different trials was not consistent. The reasons may comprise differences in pathologic complete response definition, tumor size, duration of anti-HER2 treatment, standard chemotherapy protocols and HR status. The percentage of HR+ patients varied in different trials, which may have affected the pathologic complete response rate. For instance, the percentage of HR+ and HR− patients in the NeoALTTO 19 and NeoSphere 23 trials were equivalent, however, in the CHER-LOB, 14 NSABP-B41, 26 and CALGB-40601 27 trials, more than 60% of patients were HR+. Furthermore, several studies have shown intratumoral heterogeneity was observed in HER2+ breast cancer, which can also affect the therapeutic efficacy of anti-HER2 and biologic characteristics of cancer. 36 These neoadjuvant trials have demonstrated the efficacy of dual HER2 blockade in HER2 + breast cancer. Previous studies showed that compared with single HER2 blockade, the pCR rate of dual HER2 blockade was statistically significantly improved in the range from 16% to 19%, which was not related to chemotherapy regimen. 37 This finding is consistent individual researches, regardless of the type of anti-HER2 treatment and chemotherapy, the pCR rate in the HR− subgroup was significantly increased. 14,19,23,26,27
In terms of safety, SAE incidence and cardiotoxicity following dual HER2-blockade therapy were 1.04 (95%CI: 0.81-1.33; p = 0.778) and 1.30 (95%CI: 0.81-2.08; p = 0.280), respectively, as compared with trastuzumab treatment alone, indicating that dual HER2-blockade therapy does not increase SAE incidence or cardiotoxicity relative to single-agent treatment, which increases our confidence in using dual-targeted therapy.
Here, we analyzed outcome indicators, including reported therapeutic effects, long-term survival, and adverse reactions, and found that dual HER2-blockade therapy is superior to trastuzumab or lapatinib single-agent therapy. However, this meta-analysis has several limitations. First, the number of studies included was relatively small, with one representing a summary of a meeting and only 2 related to dual HER2-blockade therapy involving trastuzumab. Moreover, the RCTs outlined in the included studies are still in progress, and follow-up reports will be used in future analyses.
Conclusions
In summary, this meta-analysis suggested that dual-target therapy can improve pCR rates relative to trastuzumab or lapatinib single-target therapy, with safety similar to that of single-agent therapy.
Footnotes
Abbreviations
Authors’ Note
This is a meta-analysis, the data source has published articles, so no ethical approval is required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.