
Abstract
Acute skin toxicity observed in radiotherapy treatment of head and neck cancer is a big concern. The purpose of this work is to evaluate the feasibility of a skin dose reduction in the treatment of nasopharyngeal carcinoma without compromising the overall plan quality. This research focused on comparison of the skin dose reduction that can be obtained for the main high conformal radiotherapy delivery techniques. Sixteen cases of early-stage nasopharyngeal carcinoma were included in this study. For each case, a dynamic intensity-modulated radiation therapy, a volumetric modulated arc therapy, and a helical tomotherapy treatment plans were performed with and without the skin as a sensitive structure in the inverse plan optimization. The dosimetric results obtained for the different treatment techniques and plan optimizations were compared. Dose–volume histogram cutoff points of D95%, D98%, and the homogeneity index were used for target comparison, while Dmean and Dmax/D1cc were used for the organs at risk. The skin volume receiving 5 Gy and then 10 to 70 Gy of radiation dosage registered at step of 10 Gy and Dmean were used for the skin dose comparison. One-way analysis of variance was used to assess the dosimetric results obtained for the different types of treatment plans and techniques investigated. A total of 96 treatment plans were analyzed. When the neck skin was considered in the treatment optimization process, the skin volume that received more than 30 Gy was reduced by 3.7% for dynamic intensity modulated, 4.1% for volumetric modulated arc, and 4.3% for dynamic intensity modulated, while the target dose coverage and organs at risk dosages remained unvaried (p > .05).
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a frequent malignancy in southern China, southeast Asia, and northern Africa. 1,2 Dynamic intensity-modulated radiation therapy (dIMRT), volumetric modulated arc therapy (VMAT), and helical tomotherapy (HT) have demonstrated their respective advantages and benefits yielded to radiotherapy 3 -5 when high-dose radiation and high conformal treatments are required. In particular, they have greatly improved the clinical effect of the overall treatment, with an amelioration of radiotherapy side reactions such as xerostomia and parotid swelling.
In NPC treatments, skin reactions remain a concern 6 -9 as they can seriously affect the patients’ quality of life. Their acute effect is observed within days after irradiation and results from damage to the epidermis (0.03-0.3 mm thick). 10,11 Late effects occur months later, mediated through damage to the dermis (1-3 mm thick). 12 In clinical radiation therapy, most patients experience different degrees of skin reactions. Erythema is common after a skin dose of about 30 Gy; dry desquamation may appear after doses of about 40 Gy to the skin, and desquamation occurs when doses to the skin exceed 50 Gy. 13 The skin reactions can be painful and may necessitate the interruption of treatment for several days, thereby affecting the overall treatment efficacy.
Treatment planning is an important step in treatment optimization. In inverse planning, the complex and nonuniform beam intensities are created by an optimization algorithm through an iteration process devised according to the dose constraints of the targets, critical organs, and other avoidance structures in the treatment region. Consequently, the contouring for targets and critical organs will significantly affect the dose distributions in an inverse planning process. Different studies investigated the aspect of skin dose reduction. By taking the skin into consideration as a sensitive structure with a dose limit during planning, it was possible to reduce the skin dose to a tolerable level. 6,7 The purpose of this study was to compare the main high conformal radiotherapy techniques for NPC with regard to the sparing effect on the skin of the neck and evaluate the feasibility to achieve a significant neck skin dose reduction without affecting the overall plan quality.
Materials and Methods
This retrospective study included 16 early-stage patients with NPC admitted and treated in our hospital from January to October 2017. The study was reviewed and approved by the Ethics Committee of Sichuan Cancer Hospital. Patients were immobilized using head-neck-shoulder masks made of 3-mm-thick perforated thermoplastic, with the neck supported on a head support secured to a carbon fiber board (Med-Tech Laboratories, Guangzhou, China). Intravenous contrast-enhanced computed tomography (CT) scans were acquired with 3-mm slices from the vertex to 5 cm below the sternoclavicular notch with a 16-slice Brilliance Big Bore CT (Philips Medical Systems, Cleveland, Ohio). Magnetic resonance images were rigidly registered with the CT images for tumor delineation. Experienced radiation oncologists of the head and neck department had drawn the targets and the organs at risk (OARs) following international guidelines. 14 -19 The planning target volumes (PTVs) were obtained with an isotropic expansion of 5 mm from the corresponding clinical target volume, except in the proximity of the critical OARs where the margin was reduced to 0 to 3 mm. Planning OAR volumes were generated with a 2-mm setup margin for OARs (brain stem, optic nerves, lens) and a 3-mm for the spinal cord. The choice of margins has been widely investigated in literature and can lead to differences between the delivered and planned doses. 20,21
The neck skin tissue was generated by a 3-mm contraction of the outer contour of the neck. The primary tumor received 70 Gy at 2.12 Gy/fraction and simultaneously the high-risk regional lymph nodes received 66 Gy at 2.0 Gy/fraction and the low-risk regions and the neck nodal region received 54 Gy at 1.64 Gy/fraction. The PTV of the above targets was named PTV70, PTV66, and PTV54, respectively. The patients underwent 33 radiotherapy fractions; cone beam computed tomography (CBCT) was performed at the first therapy session and then twice a week. The couch was moved into the correct position after the CBCT alignment process; however, the maximum displacements of up to ±3 mm on at least one of the x, y, or z directions were accepted following the procedures adopted in our department. A new CT scan was scheduled after the 15th therapy fraction for an eventual adapted plan. The above image control scheme was adopted in the clinical practice and can offer objective information to support radiation oncologist in making decision about adaptive actions. 22 A 6 MV photon beam produced by a Varian 21EX linear accelerator (Palo Alto, California) mounting a millennium 120 leaf multileaf collimator and by an HT (Tomo, H-helical, Accuray, California) was used for the radiotherapy treatments. The dIMRT, VMAT, and HT were used as delivery techniques. For each patient, 6 treatment plans were implemented overall. First, 3 standard plans, 1 for each modality, were optimized following standard dose constraints 23,24 ; we will refer these as standard plan group (SPG). Second, 3 new plans (NPs) were created using the same target volume and OARs of the SPG, but with the skin of the neck considered as a critical structure; these plans were associated with the new plan group (NPG). Overall, 48 treatment plans for each group were compared. Plan optimization was based on dose–volume objectives for PTVs and on OAR constraints commonly used in clinical practice. 25 We aimed to formulate a final plan delivering the prescribed dose to at least 95% of the tumor volume, while ensuring that the OAR doses remained as low as was achievable. In the NPG, neck skin tissue constraints were defined with dose–volume histogram (DVH) cutoff points at 10, 30, and 50 Gy (V10Gy < 53%; V30Gy < 8%, and V50Gy < 1%). Either VMAT or dIMRT treatment plans were carried out with the Eclipse (Varian, California) treatment planning system (TPS; version 7.1) using an anisotropic analytic algorithm with a 2.5-mm calculation grid size. The VMAT plans were performed with 2 coplanar full arcs (181°-179° and 179°-181°) and a slight rotation of the collimators (10°-20°) to minimize the tongue-and-groove effect. The dIMRT plans consisted of 7 beams of 153°, 102°, 51°, 0°, 309°, 258°, and 207° gantry angles. The HT plans (Tomotherapy workstation, version 4.2, Accuray, California) were performed using a convolution algorithm and 0.39 × 0.39 × 0.39 dose grid calculation. The planning parameters commonly used in our clinical practice were selected; in particular, they consisted of 2.5 cm field width, modulation factor of 3.5, and pitch of 0.43.
The DVH of the treatment plans with the resulting OAR cutoff points and percentage target coverage was used to compare the differences between the doses obtained in the different modalities and with the plan optimized with or without the neck skin as a sensitive structure (SPG vs NPG). We defined Dx% as the dose (in Gy) received by x% of the volume, Vy as the volume (in percentage) that receives y Gy, and D1 cm3 as the dose in Gy received by 1 cc of volume. D95%, D98%, and HI were used for target comparison, while Dmean, D1cc, and Dmax were used for the OARs. The uniformity of dose distribution in the target volume was analyzed with the homogeneity index (HI) following ICRU 83. 26 Homogeneity index is defined with this formula: HI = D2 − D98/D50, where D2 is the minimum dose to 2% of the target volume (indicating the “maximum dose”), D98 is the minimum dose to the 98% of the target volume (indicating the “minimum dose”), and D50 is the dose received by 50% of the target. The reason for choosing D2 and D98 to represent the maximum and minimum doses, respectively, is that the calculation of true minimum or maximum dose is sensitive to the dose calculation parameters, such as grid size and grid placement, and the high-dose gradient is common in high modulated delivery techniques. 25 An HI of 0 indicates that the absorbed dose distribution is almost homogeneous. The skin volume receiving 5 Gy and then 10 to 70 Gy registered at step of 10 Gy was used for skin dose comparison. The data processing and statistical analysis were performed with the software SPSS 19.0. One-way analysis of variance was used for the comparison of the 3 techniques. Fisher least significant differences was used to analyze post hoc multiple comparisons. Student t test was used to compare the results obtained for SPG and NPG. A P value less than .05 was considered statistically significant.
The accuracy of the neck skin dose reduction calculated by the TPSs was assessed with metal oxide field effect transistors (MOSFET) in vivo measurements. Computed tomography scans of an anthropomorphic phantom setup with a thermoplastic mask were acquired. Three points A, B, and C in the III, IV, and V lymphatic drainage areas were highlighted on the surface of the neck skin and were used for the dose reduction comparison. Targets and OARs were contoured on MIM and transmitted to Eclipse and Tomotherapy TPSs. The neck skin tissue included 3 mm from the skin surface. For each treatment modality (dIMRT, VMAT, and HT), 2 treatments plans were performed: a standard plan following the goals and constraints already defined and an NP taking into consideration the neck skin as a sensitive structure during inverse planning optimization. The dose reduction at the A, B, and C points obtained with the NP, computed by the TPSs, and measured using MOSFET was used for the comparison.
Results
The results obtained for the target coverage for SPG and NPG and for the 3 delivery modalities are reported in Table 1. The mean value and the standard deviation obtained for the DVH cutoff points highlight that for every delivery technique, treatments within NPG and SPG achieved the clinical dosimetric demands. The target coverage obtained for PTV70 and PTV54 and the homogeneity achieved in all the targets in Tomo highlight a significant difference (P < .05) when compared with that for dIMRT and VMAT, while for PTV66, the results were almost the same. The dosimetric results obtained for the OARs for the different delivery techniques and for the 2 plan optimization groups are reported in Table 2.
Results of the Main Target Volume Dosimetric Parameters Obtained for the Different Treatment Delivery Techniques and Optimization Procedures (SPG vs NPG).a

Abbreviations: dIMRT, dynamic intensity-modulated radiation therapy; HI, homogeneity index; HT, helical tomotherapy; NPG, new planning group; SPG, standard planning group; VMAT, volumetric modulated arc therapy.
a F and P are 1-way analysis of variance parameters.
Results of the Main OARs Dosimetric Parameters Obtained for the Different Treatment Delivery Techniques and Optimization Procedures (SPG vs NPG).

Abbreviations: dIMRT, dynamic intensity-modulated radiation therapy; HT, helical tomotherapy; NPG, new planning group; OAR, organs at risk; SPG, standard planning group; VMAT, volumetric modulated arc therapy.
a Statistical difference.
The comparison performed shows that HT, with respect to dIMRT and VMAT, is better able to spare OARs, particularly in the brain stem, parotid glands, oropharynx, and spinal cord (P < .05), while the maximum dose to the lenses and optic nerve obtained with VMAT was significantly lower than those of dIMRT and HT.
The trend of the dosimetric difference between the delivery techniques as for OARs as for the targets, obtained within the SPG, was maintained within the NPG. The P values obtained following the Student t test are reported in Table 3.
P Value Results Following a Student t Test Analysis Comparing the Dosimetric Results of SPG and NPG.
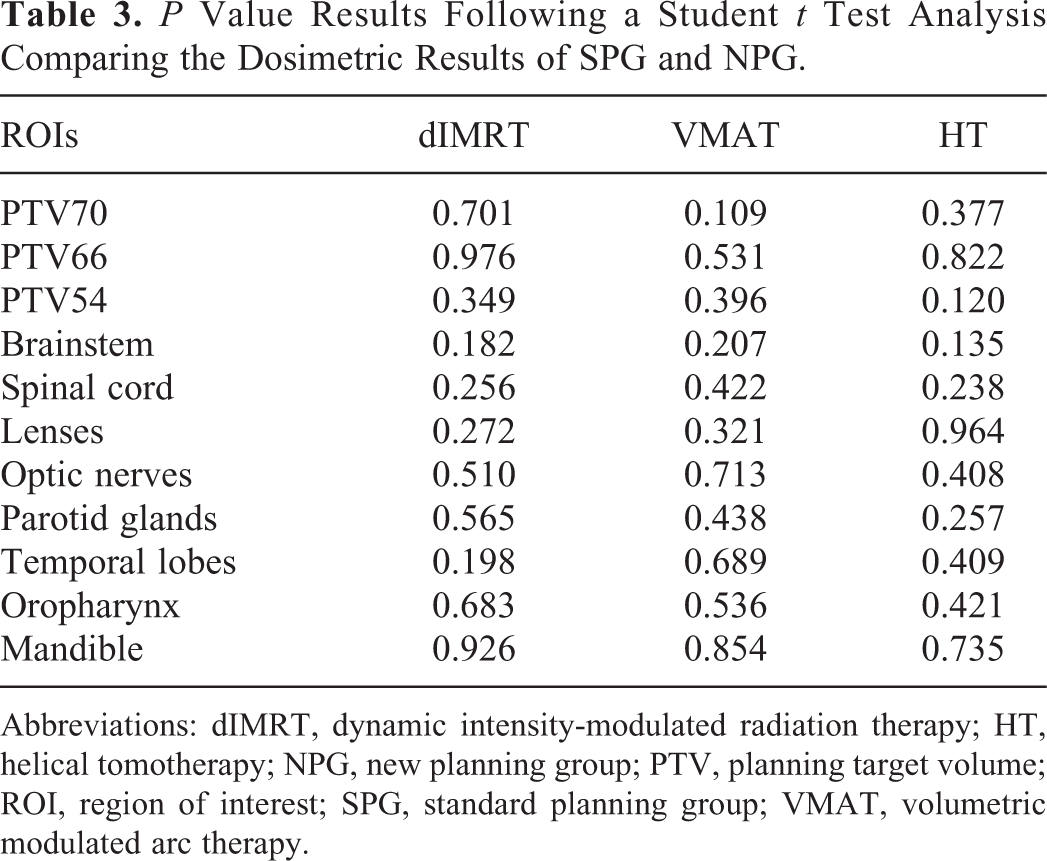
Abbreviations: dIMRT, dynamic intensity-modulated radiation therapy; HT, helical tomotherapy; NPG, new planning group; PTV, planning target volume; ROI, region of interest; SPG, standard planning group; VMAT, volumetric modulated arc therapy.
For the neck skin, the main DVH dosimetric cutoff points obtained are reported in Table 4. The HT showed higher neck skin dose for every DVH cutoff point analyzed (P < .05). The reduction of the neck skin dose obtained for NPG versus SPG is shown in Table 5. If the neck skin was contoured as a sensitive structure in the optimization process, the volume of the neck skin receiving more than 30 Gy was reduced by 4.3%, 3.7%, and 4.1%, for HT, dIMRT, and VMAT, respectively.
Neck Skin DVH Cutoff Points Obtained for the Plans Optimized Without and With (SPG vs NPG) the Neck Skin as a Sensitive Structure and for the Different Delivery Techniques.
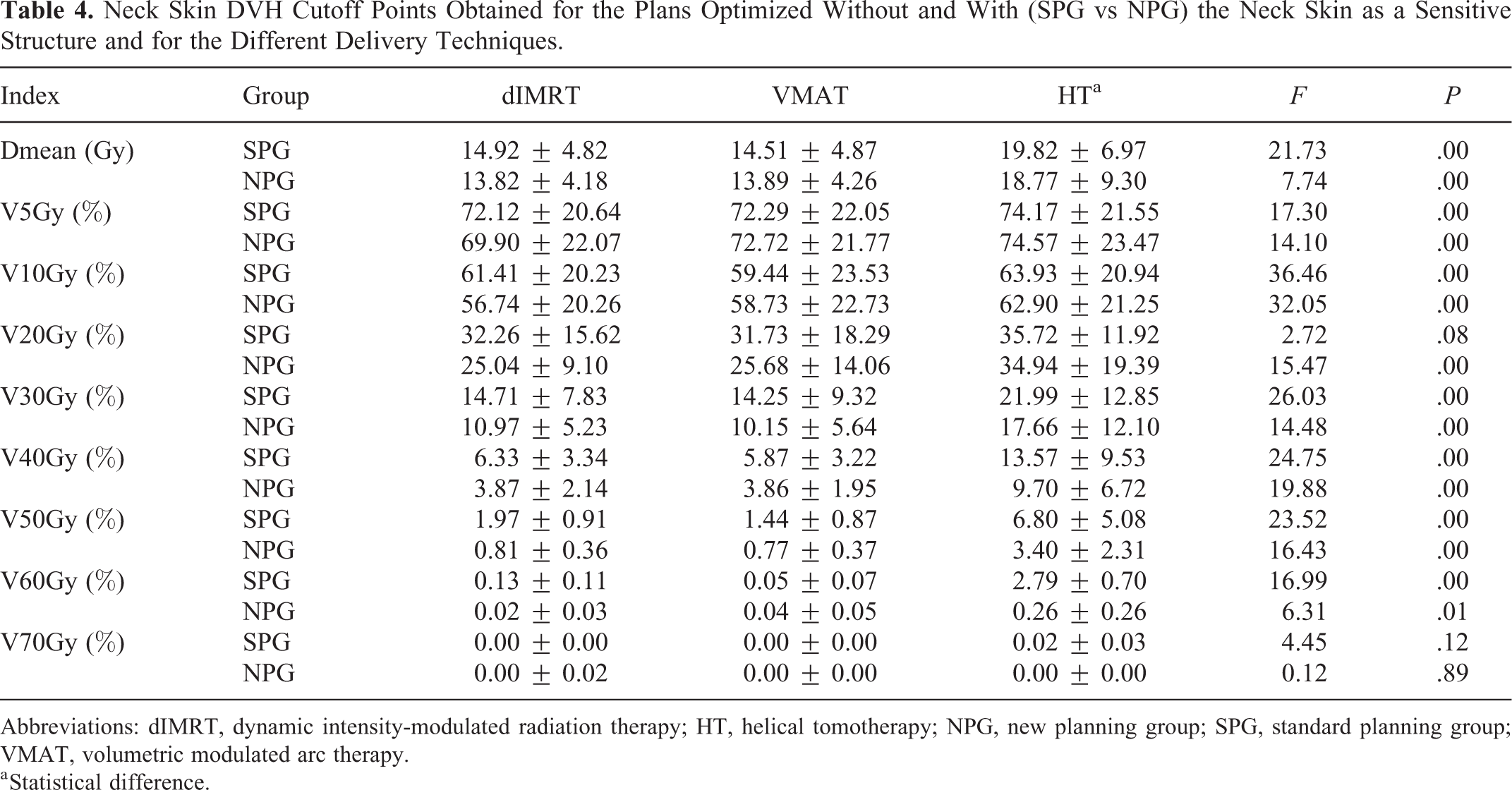
Abbreviations: dIMRT, dynamic intensity-modulated radiation therapy; HT, helical tomotherapy; NPG, new planning group; SPG, standard planning group; VMAT, volumetric modulated arc therapy.
a Statistical difference.
Reduction of the Neck Skin Dose Obtained When the Neck Skin Is Considered a Sensitive Structure.a

Abbreviations: dIMRT, dynamic intensity-modulated radiation therapy; HT, helical tomotherapy; VMAT, volumetric modulated arc therapy.
a Only the differences with a significant statistical value (P < .05) were reported.
The calculated skin dose reduction on the 3 points of the anthropomorphic phantom for the HT, dIMRT, and VMAT TPSs were within 1.1%, 1.1%, and 1.2%, respectively, when compared to dose reduction obtained with MOSFET measurements.
Discussion
All the plans in SPG, as in the NPG, reached the clinical requirements for the targets’ dose coverage with respect to the sparing of OARs. The difference found between the delivery techniques in the target coverage in case of the OARs sparing has the same trend (Table 3) as in the SPG and NPG and is generally aligned with the results of previous studies. For dose homogeneity, it was generally reported that HT was better 27 than the high-intensity-modulated techniques. In comparison with dIMRT and VMAT, HT performed better in sparing OARs, particularly in the brain stem, spinal cord, parotid glands, and oropharynx. Rotational therapy generally favored parotid gland sparing, owing to the wider range of angles for beam entry, thereby allowing avoidance of the organ. A number of articles 3,27,28 advocated the advantage of HT in parotid gland and oropharynx sparing, compared with dIMRT and VMAT. This was in line with the result of this study. Lower dose values were achieved with VMAT for the lenses compared to those with dIMRT and HT. 3,29 This phenomenon may have occurred, because in the HT plans, a field width of 2.5 cm and pitch of 0.43 were used, making the contiguous OARs and targets exposed in the same field. Therefore, the results of HT in the optical nerve were greater than those of dIMRT and VMAT. The use of dynamic jaws in HT could enable a reduction of the dose to optic nerves. 30,31 For the mandible, it was generally reported that HT was better than the high-intensity-modulated techniques. 32 The close proximity of the nasopharyngeal tumor of the mandible to the target is one of the reasons for its lower dose in HT treatments where a high conformity of the dose around the target is achievable. In our study, we found the dose to be slightly worse in HT, though statistical significance was not reached.
Of the 3 delivery techniques, dIMRT and VMAT resulted in the lowest skin dose, with HT resulting in the highest. 33 The trend was maintained in the NPG. In Figure 1, the mean neck skin DVH was reported for the 3 techniques for the SPG and NPG. For every technique, an important neck skin dose reduction was obtained when the treatment plan was performed considering the skin dose as a sensitive structure. In particular, skin doses exhibited a greater difference in the high-dose regions.
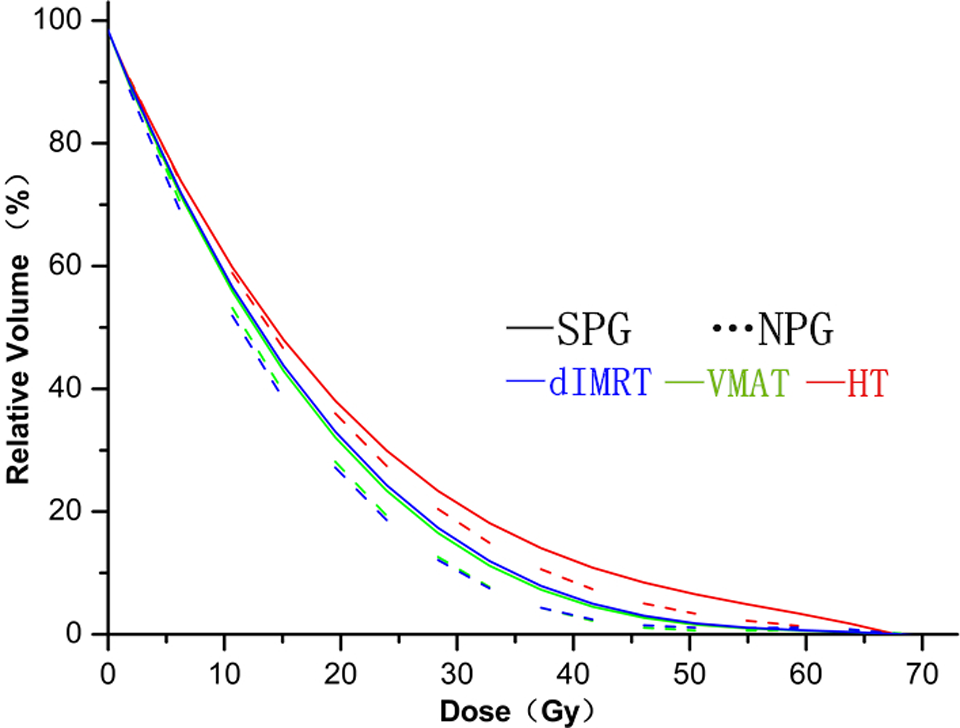
Mean value of the neck skin dose–volume histograms for the different delivery techniques (dIMRT, VMAT, and HT) and optimization groups (SPG and NPG). dIMRT indicates dynamic intensity-modulated radiation therapy; HT, helical tomotherapy; NPG, new planning group; SPG, standard planning group; VMAT, volumetric modulated arc therapy.
To increase the treatment delivery dose rate, HT systems do not have a flattening filter. As such, the dose distributions near the surface of the patient’s body may be considerably different from other forms of intensity-modulated delivery. Tangential fields would direct greater dose to the skin compared to vertical fields. A reduction of the value for the modulation factor (set up to 3.4 in the clinical routine 34 ) could provide a degradation of the integral dose for the OARs placed peripherally (as for neck skin), while increasing the dose in the OARs placed near the PTV (parotides, oral cavity). 35 The method in which the physicians contoured the drainage field of the lymph system and the lymph nodes may be one reason for the skin dose. The overlaps between the irradiated target (left and right lymph nodes and the drainage field of the lymph system) and the neck skin for the on-skin dose have a certain impact. 8 This phenomenon may be related to the pathological stages of the cases in our studies. There was a smaller area at the anatomical crossroads between the drainage field of the lymph system and the skin for early-stage NPC. In case of advanced NPC, the results may be different.
In addition to the planning techniques and the processing method of the OARs, the main factors influencing the skin dose were the bolus effect of the mask, skin sensitivity to the X-rays, the way in which the physicians contoured the drainage field of the lymph system and the lymph nodes, the changes in the patient anatomy brought on by respiratory motion, and pathological changes. The study analyzed and compared the neck skin dose obtained using a 3-mm shrinkage margin from the outer contour of the neck. However, what should be the adequate shrinkage margin in order to correctly affect the superficial dose 7,8 is still an open question. Moreover, the steep dose gradient and the complicated distributions of the contaminating electrons, along with the accuracy of dose calculation in the buildup region, still need to be verified. These modulations may lead to high doses to the superficial regions if the TPS underestimates the dose in the buildup region. The results of our research must be contextualized within the insightful limitation of this study. The study involved a limited number of treatment plans coming from a single institution; therefore, it can be considered a small study. The intention of the authors is to proceed with the study validating the results obtained in a multi-institutional research project.
Conclusion
The effect of skin injury for early-stage NPC treated with high conformal delivery techniques can be significantly reduced if the skin of the neck is included as a sensitive structure in the inverse planning optimization. The reduction of the skin dose can be obtained without compromising the overall plan quality. In case of HT for which the skin dose levels are basically higher than those for dIMRT and VMAT, a tolerable level can be achieved.
Footnotes
Authors’ Note
The study received the approval of the Sichuan Cancer Hospital Ethics Committee, in accordance with the ICH-GCP principle and related regulation/guidelines (approval number SCCHEC-02-2018-004, approval date January 12, 2018).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.