
Abstract
There are strong evidences showing the promising oncologic results of stereotactic body radiotherapy for liver tumors. This study aims to investigate the feasibility, plan quality, and delivery efficiency of image-guided volumetric modulated arc therapy-based voluntary deep exhale breath-holding technique in the stereotactic body radiotherapy for liver tumors. Treatment was planned using volumetric modulated arc therapy with 2 modified partial arc and replanned using intensity modulated radiation therapy technique for comparison. Dosimetric parameters were calculated for plan quality assessment. Quality assurance studies included both point and multiple planar dose verifications. Daily cone beam computed tomography imaging was used to measure and correct positional errors for target volumes and critical structures immediately prior to and during treatment delivery. Total monitor units and delivery times were also evaluated. No significant dosimetric difference was found between volumetric-modulated arc therapy and conventional intensity modulated radiation therapy plans. Both techniques were able to minimize doses to organs at risk including normal liver, kidneys, spinal cord, and stomach. However, the average monitor units with volumetric-modulated arc therapy were significantly lower (29.2%) than those with intensity modulated radiation therapy (P = .012). The average beam-on time in volumetric-modulated arc therapy plans was 22.2% shorter than that in intensity modulated radiation therapy plans. In conclusion, it is feasible to utilize volumetric modulated arc therapy in the treatment planning of stereotactic body radiotherapy for liver tumors under breath control mode. In comparison to conventional intensity modulated radiation therapy plans, volumetric modulated arc therapy plans are of high efficiency with less monitor units, shorter beam-on time, tolerable intrafractional errors as well as better dosimetrics, meriting further investigations, and clinical evaluations.
Keywords
Introduction
Stereotactic body radiotherapy (SBRT) utilizes special patient immobilization devices, strict treatment planning, and precise image guidance to deliver high biological equivalent dose to targets over 1 to 5 fractions in selected patients who had liver lesions that were of maximal size less than 5 cm, unresectable, not amenable to radiofrequency ablation, with limited alteration in liver function, and good performance status, that is, Zubrod Performance Status 0 to 2. 1 –5 There are strong evidences shown that SBRT could be an effective treatment option for certain patients having hepatocellular carcinoma (HCC) or liver metastases. 6 – 11 The local control rate is satisfactory, and toxicity profiles are tolerable.
The implementation of SBRT can be via multiple techniques, including 3-dimensional conformal radiotherapy techniques (3D-CRTs), intensity modulated radiation therapy (IMRT), and modern volumetric modulated arc therapy (VMAT). As the most common technique, 3D-CRT utilizes multiple beams with coplanar and noncoplanar arrangements. 12 –14 Thomas et al 15 demonstrated that inversely optimized IMRT plans were dosimetrically superior to 3D-CRT plans at the expense of more beam utilization and longer delivery time. Owing that liver tumors move with respiratory motion, precise delivery of the treatment is challenging. Various respiratory motion management strategies, for instance respiratory gating technique and breath-holding maneuver, have been proposed to reduce motion-related errors during treatment delivery. 16 –18 Among them, the breath-holding maneuver has been widely used and adopted in clinical practices. Wunderink et al 19 reported that respiration-related tumor motion could be reduced to less than 5 mm with breath holding. However, due to a limited delivery time window, breath-holding-assisted SBRT demands high delivery efficiency.
More recently, VMAT delivery techniques have been developed for clinical use, including RapidArc (Varian Medical Systems, Palo Alto, California) and VMAT (Elekta AB, Stockholm, Sweden). A typical one arc VMAT treatment can be completed in less than 2 minutes with gantry continuously rotating around patients and variable instantaneous dose rate (DR), MLC leaf positions, and gantry rotational speed for dose distribution optimization. 20,21 Apparently, VMAT is particularly favorable in the aspect of shortening beam-on time, especially for hypofractionated SBRT treatment. 22 This study aimed to evaluate treatment plan quality and delivery efficiency of VMAT with comparison to IMRT for breath-holding SBRT in patients with liver cancer.
Materials and Methods
Patient Data
This retrospective study was based on 9 patients with liver tumors, including 5 HCCs and 4 metastases from colorectal carcinomas, at Fudan University Huadong Hospital between 2012 and 2013. Patient characteristics are presented in Table 1. Liver SBRT was conducted via VMAT using a Varian linear accelerator (Trilogy; Varian) with Millennium 120 MLC. All patients were closely followed up at 1 and 4 months posttreatment for radiation-induced liver disease (RILD) and any other treatment-related discomforts.
Patient Characteristics.

Abbreviation: HCC, hepatocellular carcinoma.
Treatment Planning
For this study, IMRT-based plans were retrospectively generated for each case following the same prescription and constraints to the actual VMAT-based plans for comparison. For computed tomography (CT) simulation, patients were immobilized with the Alpha Cradle device and 3 series of CT images were acquired with a slice thickness of 2.5 mm in voluntary deep exhale breath hold (vDEBH), which was more reproducible than inhale, in consistency with Radiation Therapy Oncology Group (RTOG) 1112 trial. 23 The vDEBH scan were acquired using audiocoaching (recorded voice, both during CT scan and during irradiation, asking the patient to “quietly breath in, breath out, breath in, breath out, take a deep exhale, and hold your breath”) and verified using breathing signals from the real-time position management (RPM) respiratory gating system (Varian Medical Systems). The gross tumor volumes (GTVs) were contoured on each exhale breath hold CT image series by a radiation oncologist with expertise in liver tumors. The GTV contours from 3 vDEBH CT image series were superimposed to generate the internal target volume (ITV), and the planning target volume (PTV) was defined as the ITV + 5 mm, accounting for daily immobilization uncertainty. Normal structures and organs at risk (OARs), including normal liver (defined as the total liver volume minus GTV), kidneys, spinal cord, and stomach, were contoured by a dosimetrist and confirmed by the radiation oncologist. All patients received prescription of 50 Gy in 5 fractions (10 Gy per fraction) over 2 weeks.
All treatment plans were generated in the Eclipse planning system (version 8.6; Varian Medical Systems). For each patient, 2 plans were generated: one using coplanar conventional IMRT technique and the other using VMAT technique. The dose distribution was calculated with a heterogeneous dose calculation algorithm (the Eclipse anisotropic analytical algorithm) with a dose calculation grid 3 of 2.5 mm in VMAT and IMRT treatment plans. The same CT data set was used for both analyses.
In the VMAT plan, 2 partial arc arrangements were utilized to adapt the location of the tumor and normal tissues. Some portions of the arc were blocked in order to minimize doses to normal structures. The initial step of VMAT planning was to determine the partial arc range based on the PTV location. Next, an area of shielding within the arc was designed to exclude beams toward prioritized normal structures. In the IMRT plan for comparison, a dynamic sliding window method with fixed gantry beams was used. In all, 6 to 9 separated beams were arranged initially, and beam orientations were adjusted to minimize the irradiated volume of the critical normal structures from beam’s eye view (Figure 1). Unless specifically setting a limit on the number of segments, the sliding window generated the segments as it needed. Total segments varied from 40 to 150, and fixed DR of 600 monitor unit (MU)/min was used in IMRT plans.

Comparison of beam arrangement in axial views and color-wash dose distribution for 2 partial arc volumetric modulated arc therapy (VMAT) plan (A and C) and 7 coplanar fixed beams intensity modulated radiation therapy (IMRT) plan (B and D). Planning target volume (PTV) was contoured in red line.
Same isocenters were used in VMAT and IMRT plans. All fields or arcs were simultaneously optimized to generate desired dose distributions on all targets. Both plans were optimized with the same dose volume objectives, constraints, and prioritizations of organs.
Image-Guidance Treatment Delivery
During treatment delivery, cone beam CT (CBCT) guidance was applied for target position correction and validation. Two sets of CBCT images were acquired, one set immediately after the patient setup (representing interfractional error) and the other one prior to the delivery of the second arc (representing intrafractional error). The alignment between CBCT and planning CT was based on skin markers and/or anatomical landmarks, such as large liver vessels and surface features of the liver. The image match results should be approved by the radiation oncologist for treatment implementation. For the entire population of patients, group systematic errors and random errors were calculated to assess the interfractional and intrafractional reproducibility of target positions at 3 coordinates.
Dosimetric Evaluation Parameters
Plan evaluation was based on dose volume histogram (DVH) analysis for the normal liver (liver minus PTV), right and left kidneys, the spinal cord, small bowels, stomach, and the target (PTV). Serial normal tissues for small bowel and stomach were evaluated by the maximum dose (Dmax), defined as the maximum dose encompassing 5 cm3 of the OARs volume. 24 Besides that, the maximum point dose (Dmax) of spinal cord was also compared. Parallel tissues, including liver and kidneys, were evaluated by quantification of mean and maximum dose. 25 In addition, doses to 20% and 30% of normal liver volume receiving 15 and 21 Gy were calculated and compared.
Dose was prescribed to the peripheral isodose line covering the PTV. Maximum dose to the PTV Dmax defined at 1 cm3 of volume, minimum dose to the PTV (Dmin, defined as minimum dose to 98.0% of the PTV volume), and mean PTV dose (Dmean) were calculated based on recommendations issued by ICRU 83. 24 Maximum dose within PTV <150% was permitted and if multiple PTVs existed, <150% of the maximal PTV prescription dose was permitted for all PTVs as well and the PTVs for each patient was, at minimum, covered by the 90% prescription isodose line.
Quality Assurance
Beam verification and quality assurance (QA) were performed prior to treatment delivery. Quality assurance for each VMAT plan was conducted using a Matrixx dosimetry device (IBA Dosimetry, Germany) and an ion chamber (IC-10). Ion chamber measurements were carried out at the isocenter with a compact Farmer chamber in a solid water phantom to compare the measured doses to the calculated results from the treatment planning system. Dose distributions on sagittal and coronal planes were measured in the isocenter plane with the Matrixx device facing the gantry angles at 0° and 270°, respectively. Matrixx dosimetry data were analyzed in the relative mode with Gamma parameters of 3% to 3 mm with 5% tolerance. 26
Statistical Analysis
The differences between VMAT and IMRT plans were assessed using the Wilcoxon matched-pairs signed-rank test considering that there was a one-to-one pairing between the IMRT plan and the VMAT plan (same CT data set was used for both plans) for the small group sample. SPSS software (SPSS, Inc, Chicago, Illinois) was used for the statistical calculation, and analysis and a 2-tailed P ≤ .05 were defined as statistical significance.
Results
Target Coverage
The average volume of GTV for these 9 patients was 40.2 cm3. The average and standard deviation volume of PTVs were 115.8 ± 78.9 cm3 (Table 2), and the PTV for each patient was, at minimum, covered by the 90% prescription isodose line in both IMRT and VMAT plans. There was no statistically significant difference between both techniques with respect to the maximum, minimum, and mean doses delivered to the PTV (Table 2). Additionally, the volume receiving at least 95% of the prescribed dose using either IMRT or VMAT was compared and no statistical difference was found.
Comparisons of Standard Dosimetrics, QA, and Delivery Parameters Between VMAT and IMRT Plans.

Abbreviations: IMRT, intensity modulated radiation therapy; MU, monitor unit; PTV, planning target volume; QA, quality assurance; SD, standard deviation; VMAT, volumetric modulated arc therapy.
Organ-At-Risk Dose Sparing
Serial organs
On average, max dose values delivered to the spinal cord were 1068 cGy in the VMAT plans and 1046 cGy in the IMRT plans (P = .859), as shown in Table 2 and Figure 2, respectively. The Dmax values delivered to the stomach were 1995 cGy in the VMAT plans and 2505 cGy in the IMRT plans (P = .128).

Comparison of DVHs for representative normal organs in both volumetric modulated arc therapy (VMAT) and intensity modulated radiation therapy (IMRT) plans (DVH data averaged on all patients). A, Liver; B, stomach; C, left kidney; and D, right kidney. DVH indicates dose volume histogram.
Parallel organs
The mean dose of normal liver was 1172 cGy in the VMAT plans and 1125 cGy in the IMRT plans (P = .086). The volumes receiving dose higher than 15 and 21 Gy were 431 and 254 mL in the VMAT plans, with comparison to 420 and 254 mL in the IMRT plans, respectively. Contralateral kidneys received less dose with IMRT techniques than VMAT techniques in terms of Dmin (50.6 vs 117 cGy, p = 0.038), with no significant Dmax measurements. On the contrary, VMAT techniques outperformed IMRT techniques in Dmax for ipsilateral kidneys. The maximum doses to the ipsilateral kidneys were 1318 cGy in the VMAT plans and 1782 cGy in the IMRT plans with marginal statistical significance (P = .049; Table 2 and Figure 2). However, no significant difference was found in Dmin to the ipsilateral kidneys, 279 cGy in the VMAT plans versus 337 cGy in the IMRT plans (P = .327).
Daily Online Set-Up Verification and Interfraction Motion Verification
Daily CBCT was performed for corrections of interfractional setup errors and intrafractional motion (Figure 3). In this study, the systematic errors for interfractional position setup were 0.34 ± 0.26 cm in vertical direction, 0.70 ± 0.56 cm in longitudinal direction, and 0.22 ± 0.19 cm in lateral direction; and the random errors were 0.31, 0.48, and 0.15 cm, respectively. The systematic errors for intrafractional position validation between the first and second arc were 0.10 ± 0.13, 0.07 ± 0.14, and 0.07 ± 0.09 cm with random errors of 0.11, 0.12, and 0.10 cm in vertical, longitudinal, and lateral directions, respectively (Figure 4). With comparison to the institutional IMRT-based treatment data, the interfractional setup errors were at the same level, but the intrafractional motion was reduced approximately by 20%, most likely contributed by reduced beam-on time and table time.

Interfractional and intrafractional positional correction can be performed with online match of voluntary exhale breath-hold CBCT image and planning CT image. A, Transverse view; B, coronal view; red line, the diaphragmatic dome in planning CT; and yellow line, the diaphragmatic dome in CBCT. CBCT indicates cone beam computed tomography; CT, computed tomography
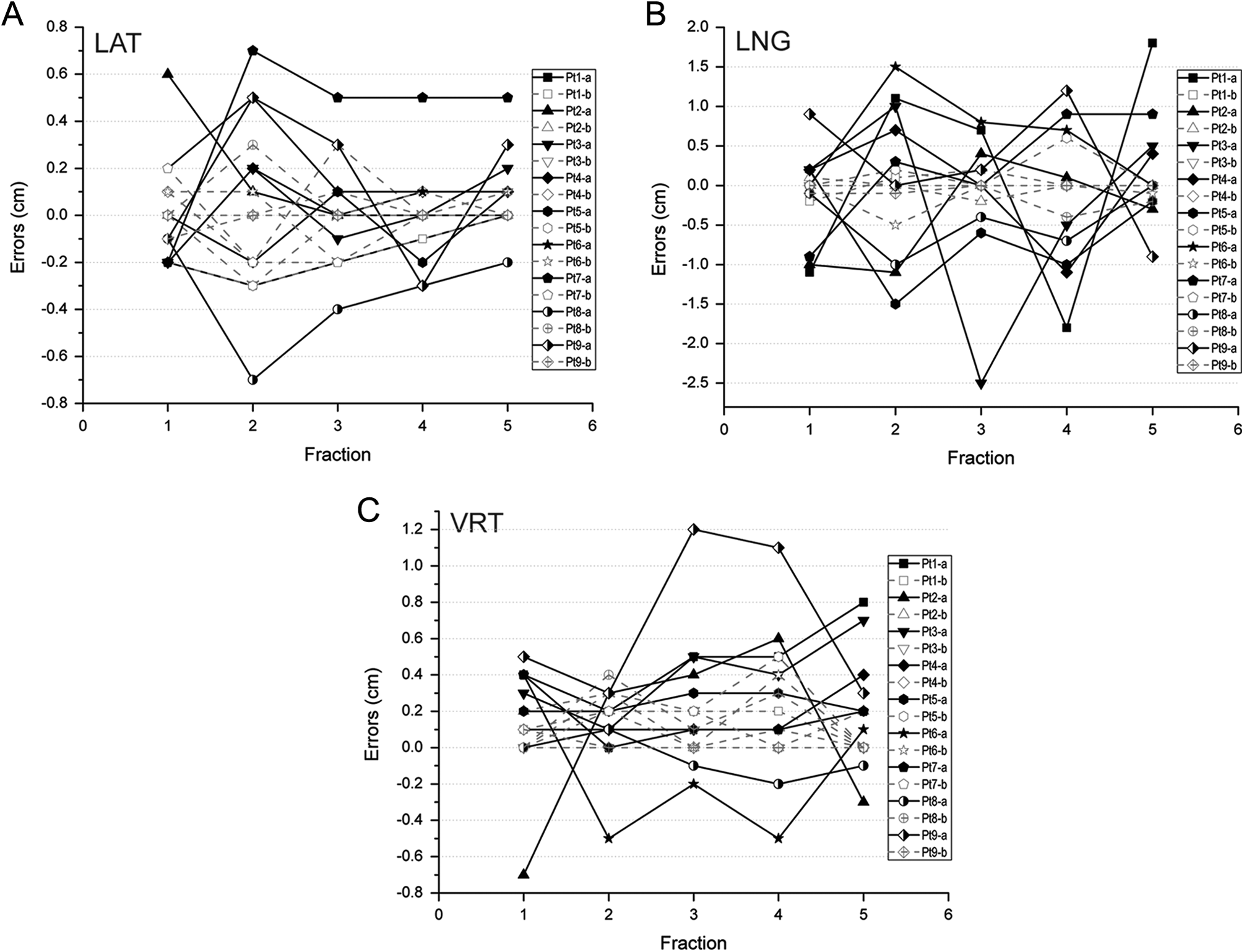
The correlation of daily online setup verification and interfraction motion verification of all the patients. A, Longitudinal direction; B, lateral direction; and C, vertical direction. Note for labels: -a, interfractional error (solid lines) and -b, intrafractional error (dash lines). For instance, Pt1-a and Pt1-b indicate the interfractional and intrafractional errors observed in patient 1, and so on.
Monitor Unit and Delivery Time
The average total MUs were 2599 (range, 1890-3061) for VMAT plans and 3671 (range, 2952-5685) for the IMRT plans. Compared to IMRT, VMAT techniques dramatically reduced MU numbers by 29.2% on average (P = .012). The mean delivery times and standard deviations were 4.76 ± 0.37 minutes for the VMAT plans, a reduction of delivery time by 22.2%, in comparison to IMRT, 6.12 ± 1.48 minutes (p = 0.017). It should be noted that the delivery time reported in this study was the beam-on time, not including time spent in procedures of set-up and image guidance.
Dose Verification and QA
Using the institutional criteria of 3%/3 mm DTA and a 5% threshold in the Gamma analysis, the average minimal pass rates of 97.2% and 93.2% were observed in the VMAT plans and IMRT plans. Using a solid water phantom and an IC-10 ion chamber, the average absolute point dose discrepancies between the calculated and measured doses were 1.4% for VMAT plans and 0.7% for IMRT plans.
Discussion and Conclusion
In this study, we investigated the feasibility and efficiency of VMAT technique in vDEBH SBRT treatment of liver tumors in comparison to the conventional IMRT technique. Our results showed that VMAT technique could achieve comparable target coverage and acceptable plan quality with higher efficiency, characterized by reduced beam-on time and intrafractional motion. In the radiation therapy of hepatic tumors, it is critical to minimize the mean dose received by normal liver, since researchers have indicated that the RILD correlates with the mean radiation dose received by normal liver tissue. 27,28 A maximum volume of 700 mL receiving a total dose of less than 15 Gy has been used as the normal liver constraint. 29 In this study, the mean doses delivered to the normal liver were comparable between the VMAT plans (1172 cGy) and the IMRT plans (1126 cGy). Within a median follow-up period of 1.6 years, no RILD occurred in all patients.
Kidneys obey both parallel and serial architecture model of radiobiology. The DVH-derived low-dose volume of the contralateral kidney was smaller in IMRT plans than in VMAT plans, as well as mean dose (50.6 cGy in IMRT vs 117 cGy in VMAT). Although there were no significant difference in the maximum doses of stomach, the IMRT approach was slightly better in the DVH distribution numerically.
This study demonstrated that the VMAT-based plans had some advantages over conventional IMRT for the SBRT treatment of liver tumors, including a substantial reduction in delivery time (22.2%) and concomitant reduction in total MU required for delivery (29.2%). Both VMAT-based and IMRT-based SBRT require strict patient setup, imaging guidance, and target position validation during treatment delivery, which are time-consuming and could induce treatment-related uncertainty. It is of great benefit to minimize patient on-table time including beam-on time. The VMAT technique has the advantages of reducing the number of treatment breaks during each beam delivery, resulting in shorter overall treatment time and improved patient compliance. More importantly, short beam-on time makes the breath-holding maneuver feasible. Less MUs with VMAT technique would decrease total body scatter dose and subsequent toxicities, such as hematological adverse events. Moreover, faster delivery using VMAT has the potential to minimize patient/organ motion during the entire treatment, reflected by the intrafractional motion.
Reproducible patient positioning is favorable for minimizing interfractional setup errors, while robust immobilization with comfort is vital for controlling intrafractional motion, which is extremely important for time-consuming procedures, especially SBRT. Interfractional setup errors could be corrected using image guidance. However, intrafractional motion was subject to multiple factors, including respiratory motions, intestinal peristalsis, and patient involuntary motion on the table. Therefore, in this study, image guidance plus vDEBH help correct part of intrafractional motion. To some extent, intrafractional motion could compromise the planned dosimetry for both VMAT and IMRT. 30,31 The VMAT technique utilizes 2 partial arcs (considering MLC leaf motion, gantry rotation speed, and DR fluctuation) to achieve the combination of optimization flexibility and time efficiency. The delivery time with VMAT is much less than that with conventional IMRT, mainly due to elimination of in-between beam motion time required in IMRT. Both techniques have comparable dose distributions and dose conformity in the treatment plans for liver SBRT cases.
Respiratory motion could also affect the actual dose distribution during radiotherapy. Some studies have indicated that dosimetric variations introduced by respiratory motion are, in general, significant in abdominal tumors. 32 –34 It has been proven that minimizing target motion subject to respiratory motion would be beneficial in the treatment of intrahepatic cancers by producing more accurate target volume delineation compared to a free breathing planning CT study. 35 Respiratory motion management strategies include breath-holding maneuver, real-time tumor tracking technique commonly used in Cyberknife system, and respiration gating extensively seen in linear accelerator system. 36,37 As strongly suggested in RTOG 1112 trial, the breath control mode of vDEBH assisted with RPM is more reproducible than inhale, hence used for patients with liver cancer in this study. This breath-holding technique becomes more viable with the use of faster delivery VMAT technique, which reduced delivery time and potentially increases the feasibility of the clinical utility of breath-hold techniques during treatment.
In conclusion, this study demonstrated that VMAT technique could be applied to SBRT treatment of liver tumors with comparable dosimetric features with comparison to conventional IMRT technique. Considering shorter beam-on time required than IMRT, VMAT could be more treatment efficient and readily integrated with respiratory motion management procedures, such as breath-holding maneuver to reduce doses to critical structures. Our results should be cautioned for interpretation due to limited patients. Long-term treatment outcome (survivals) and adverse events (the occurrence of hepatitis or cirrhosis) are the ultimate end points in evaluating the efficacy between VMAT technique and IMRT technique. Due to the short observation period in this study, related data currently are not available which is another limitation that should be taken into consideration at interpretation of our results. Long-term follow-up will be continued and prospective clinical trials are planned to further investigate the advantage of VMAT over IMRT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (No. 81472794).