
Abstract
Background:
Noncoding RNAs are crucial regulators acting as either tumor suppressor genes or oncogenes in human cancer progression. The aberrant expression of noncoding RNAs has been confirmed in different kinds of cancers. Hepatocellular carcinoma is one of the most common malignant tumors worldwide, characterized by insidious onset, great malignancy, and high rates of recurrence and metastasis. Due to lack of early predictive markers, numerous patients are diagnosed in the late stages. As therapeutic options for advanced patients are quite limited, great efforts have been made to screen patients at early stages. A previous study reported that small nucleolar RNA host gene 18 played crucial role in glioma. However, its functions and roles in hepatocellular carcinoma are unknown.
Purpose:
To explore its functional role and diagnostic value in hepatocellular carcinoma, we investigated its expression level.
Methods:
We performed real-time quantitative polymerase chain reaction in tumor tissues and adjacent noncancerous tissues derived from patients with hepatocellular carcinoma as well as in plasma, including samples from the healthy control, patients with hepatitis B, cirrhosis, and hepatocellular carcinoma.
Results:
Small nucleolar RNA host gene 18 was downregulated in liver tissues compared to paired adjacent noncancerous tissues (P < .0001). Meanwhile, plasma small nucleolar RNA host gene 18 showed a relatively high sensitivity and specificity (75.61% and 73.49%) for distinguishing patients with hepatocellular carcinoma whose α-fetoprotein levels were below 200 ng/mL from the healthy controls.
Conclusion:
Our study suggested that small nucleolar RNA host gene 18 might act as a tumor suppressor gene in hepatocellular carcinoma and potentially a diagnostic indicator to distinguish hepatocellular carcinoma from the healthy control and cirrhosis.
Introduction
Hepatocellular carcinoma (HCC) accounts for the most common form of primary liver cancer 1 and ranks the second most common cause of deaths related to cancers. 2 Viral infection, alcoholic cirrhosis, and fatty liver are the common risk factors for HCC. 3 Chronic inflammatory conditions of the biliary tree, genetic disorders, and carcinogens can also increase the risk of developing into HCC. 4 It is widely accepted that the development of HCC is a multistep process. Over the past 2 decades, the incidence of HCC is increasing at a rate second to thyroid disease in the United States. 5 -7 Notably, HCC represents a serious health crisis worldwide. Currently, the diagnosis of HCC mostly relies on imaging studies and laboratory tests. Ultrasonography, computed tomography scanning, and magnetic resonance imaging are the widely used imaging methods in the diagnosis, treatment assessment, and prognosis prediction of HCC. With respect to laboratory tests, α-fetoprotein (AFP) is the most frequently used marker. Disappointingly, due to the absence of sensitive imaging methods and biomarkers, the patients with HCC are mostly detected at advanced stages. In addition, HCC is inclined to recur and metastasize, so the 5-year survival rate remains far from satisfactory. 8 Therefore, it is in an urgent need to explore the potential mechanisms underlying liver cancer and find out sensitive biomarkers to screen out high-risk patients.
The development of high-throughput RNA sequencing technology makes it possible to discover noncoding RNA genes in great numbers. In fact, the numbers of noncoding RNA genes are much more greater than the coding transcripts. 9 Noncoding RNAs include classical ribosomal RNA, small nucleolar RNA, small nuclear RNA, transfer RNA, and the most-studied microRNA and long noncoding RNA. 10 Instead of being “junk RNA,” accumulating evidence indicates that noncoding RNAs are of great significance in the physiological and pathological processes. 11 Although noncoding RNAs are unable to code proteins, they play critical roles in cellular processes such as proliferation, differentiation, apoptosis, via pre and posttranscriptional regulation. 12 Increasing studies have reported that noncoding RNAs are deregulated in cancers, which suggests that noncoding RNAs are strongly related to the development and progression of cancers. 13
A recent study showed that upregulation of small nucleolar RNA host gene 18 (SNHG18) could promote radio resistance of glioma by repressing Semaphorin 5A, 14 demonstrating that SNHG18 was related to cancer development. Possible mechanism was that SNHG18 could interact with microRNA-binding sites and thus downregulate the expression of Semaphorin 5A. Noncoding RNAs could act as competing endogenous RNAs (ceRNAs), called ceRNA regulation mode, which was confirmed in various cancers. 15 Until now, little is known about the relationship between SNHG18 and HCC. In our study, we aim to explore the expression pattern of SNHG18 in the tissues of HCC and in the plasma of related diseases and further evaluate whether it can be a screening biomarker for HCC.
Materials and Methods
Tissue and Plasma Samples
We collected 71 paired HCC tissues in the Zhongnan Hospital of Wuhan University from April 2016 to July 2017. All patients had been pathologically diagnosed as HCC, none of who had previously undergone radiotherapy or chemotherapy treatment. Blood samples were obtained from the Zhongnan Hospital of Wuhan University, including 4 groups: 80 preoperative samples of HCC, 83 samples of cirrhosis, 60 samples of chronic hepatitis B, and 83 healthy control (samples collected from the Physical Examination Center of the Zhongnan Hospital of Wuhan University). All healthy controls were excluded from hepatitis, hepatic diseases, or aberrant indicators related to the liver function. We collected blood samples into the EDTA anticoagulant tubes. All blood samples were centrifuged at 2000g for 5 minutes at 4°C to separate the blood cells. The supernatants were then transferred to microcentrifuge tubes and centrifuged at 12 000g for 5 minutes at 4°C to completely remove cell debris. Tissue and plasma samples were stored at −80°C until use.
RNA Extraction and Reverse Transcription
The total tissue RNA was extracted by Trizol reagent (Invitrogen, California). Separate extraction kit (Biotake, Beijing, China) was used to extract the RNA of plasma according to the manufacturer’s instruction. We used NanoDrop ND2000 (Thermo, California) to quantify the concentration and purity of extracted RNA. Complementary DNA was synthesized using PrimeScript RT reagent Kit with genomic DNA Eraser (Takara, Japan).
Real-Time Quantitative Polymerase Chain Reaction Analysis
To quantify the expression levels of SNHG18, real-time quantitative polymerase chain reaction (RT-qPCR) assay was performed on the Bio-Rad CFX96 (Bio-Rad Laboratories, Inc., Hercules, CA, USA) using SYBR-Green I Premix EXTaq. The cycling program for amplification was set for initial stage at 95°C for 5 minutes, followed by 40 cycles of 95°C for 30 seconds, 61.4°C for 30 seconds, and 72°C for 30 seconds. The glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used to normalize the results of RT-qPCR. The synthesized primers were as follows: SNHG18 (forward: 5′-GACCTGGACCTCACCTAA-3′ and reverse: 5′-GCTGCTTCCTTGAACTTG-3′); GAPDH (forward: 5′-AGAAGGCTGGGGCTCATTTG-3′ and reverse: 5′-GCAGGAGGCATTGCTGATGAT-3′). All reactions were run in duplicate. Relative gene expression levels were calculated in −log2Δ C t.
Statistical Analysis
All statistical analyses were carried out using the SPSS version 23.0 (SPSS, Inc Chicago, Illinois) and GraphPad Prism 6.0 (GraphPad Software, La Jolla, California). The Shapiro-Wilk test was used to check whether the data were normally distributed. Normal distribution data were presented as mean ± standard deviation (mean ± SD). Nonnormal distribution data were described by quartiles. The differences between normally distributed numeric variables within the 2 groups were evaluated by Student’s t test, meanwhile nonnormally distributed numeric variables were analyzed by Mann-Whitney U test. If the variance was homogeneous, 1-way ANOVA was used for the comparison among multiple groups, whereas nonnormally distributed variables were evaluated by Kruskal-Wallis variance analysis. χ 2 test was adopted to analyze the categorical variables. P < .05 was considered to be statistically significant.
Results
Correlation Between SNHG18 and Clinical Variables
The main demographic and clinical characteristics of the patients included are shown in Table 1. No statistical significance was found in gender, age, smoking, alcoholism, cirrhosis, hepatitis B virus (HBV) DNA, and other biochemistry indexes. However, SNHG18 levels were correlated with the tumor size and levels of serum AFP in the tissues.
Association of SNHG18 Expression With Clinical Parameters in HCC.

Abbreviations: AFP, α-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; TNM, tumor node metastasis.
Data are mean ± SD.
a P < .05.
The Expression Level of SNHG18 was Significantly Downregulated in HCC Tissue Specimens
The expression level of SNHG18 was measured by RT-qPCR in 71 paired clinical HCC tissues and adjacent normal liver tissues. Expression of SNHG18 relative to GAPDH in tumor tissues was significantly downregulated compared with nontumor tissues (P < .0001; Figure 1A and B). Furthermore, the expression levels of SNHG18 were correlated with the tumor sizes (P = .028) and levels of the serum AFP (P = .025; Figure 1C and D).

SNHG18 expression in hepatocellular carcinoma tissues and adjacent normal liver tissues. A and B, SNHG18 expression levels in tumor tissues were significantly lower than in nontumor tissues (P < .0001). C, SNHG18 expression levels were associated with the tumor size (P = .028). D, SNHG18 expression levels were associated with the levels of α-fetoprotein (P = .025). *P < .05, ***P < .001.
The Expression Level of SNHG18 in Plasma Among Subgroups
The main demographic and clinical characteristics of studied patients were shown in Table 2. No difference was observed in important risk factors including gender, age, smoking, and alcoholism in the 4 groups. There was a significant difference in the AFP, alanine aminotransferase, and aspartate aminotransferase among the groups.
Characteristics of the Studied Subjects.

Abbreviations: AFP, α-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase.
a χ2 test.
b Median (25 percentiles, 75 percentiles), some data are missing.
c Kruskal-Wallis.
To observe the diagnostic value of SNHG18 as biomarkers, we detected the expression level of SNHG18 in plasma by RT-qPCR. The results indicated that the expression of SNHG18 in HCC was lower than in healthy controls and patients with cirrhosis (HCC vs cirrhosis: P < .001; HCC vs the control: P < .001). When comparing the expression level of hepatitis B, cirrhosis, and the healthy control, the former was lower than the latter two. However, no significance was found between patients with HCC and patients with hepatitis B and cirrhosis and healthy controls (Figure 2). The proportion of each group according to the quartiles of the SNHG18 expression level is shown in Table 3.
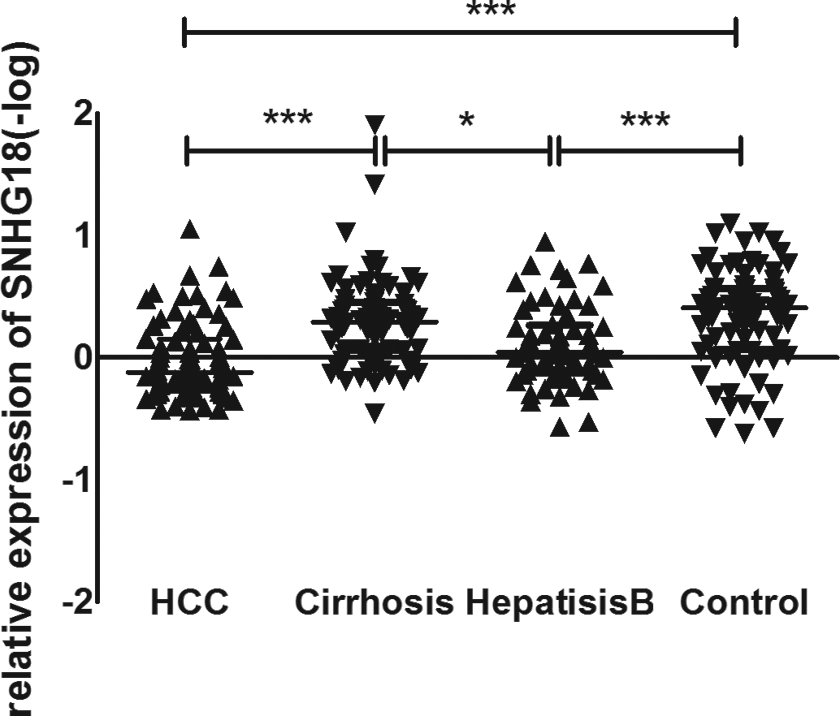
SNHG18 levels in plasma among subgroups. The data are analyzed using Kruskal-Wallis variance analysis. *P < .05, ***P < .001.
The Proportion of Each Group According to the Quartiles of the SNHG18 Expression Level.a
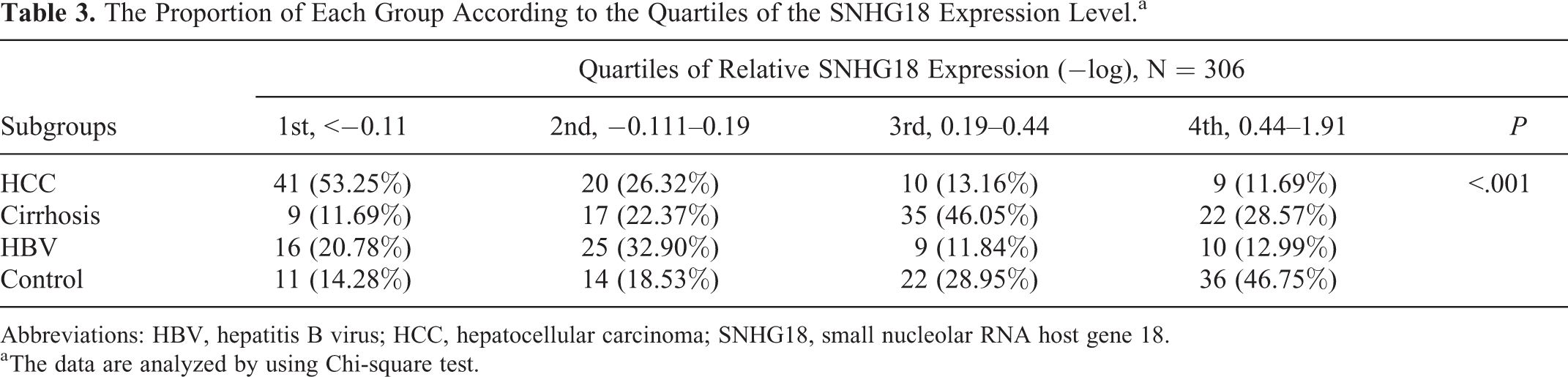
Abbreviations: HBV, hepatitis B virus; HCC, hepatocellular carcinoma; SNHG18, small nucleolar RNA host gene 18.
a The data are analyzed by using Chi-square test.
Diagnostic Value of SNHG18 in Plasma
To assess whether plasma SNHG18 could be used as a potential diagnostic marker for HCC, receiver–operating characteristic curve (ROC) was constructed by 5 models: HCC versus the healthy control, HCC with AFP levels below 200 ng/mL versus the healthy control, HCC versus cirrhosis, HCC with AFP below 200 ng/mL versus cirrhosis with AFP also below 200 ng/mL, and hepatitis B versus the healthy control (Figure 3).

Receiver–operating characteristic curves. A, Hepatocellular carcinoma (HCC) versus the healthy control; B, HCC with the α-fetoprotein levels less than 200 ng/mL versus the healthy control with the AFP levels also less than 200 ng/mL; C, HCC versus cirrhosis; D, HCC whose AFP levels below 200 ng/mL versus cirrhosis whose AFP Levels also below 200 ng/mL; E, Hepatitis B versus the healthy control.
From Table 4, we could know that the area under curve (AUC) of SNHG18 was greater than that of AFP. In addition, SNHG18 showed a relatively high AUC in distinguishing HCC with AFP levels below 200 ng/mL from the healthy controls (AUC = 0.7459, 95% CI: 0.6530-0.8427) and from patients with cirrhosis whose AFP levels were also <200 ng/mL (AUC = 0.7527, 95% CI: 0.6482-0.8573). The sensitivity of SNHG18 would be improved if we combined AFP with SNHG18 for those whose AFP levels were below the diagnostic standard. So, it was necessary to combine SNHG18 with AFP to screen out patients with HCC.
Comparisons of the AUC of AFP, SNHG18, and Combining AFP with SNHG18 for Subgroups.
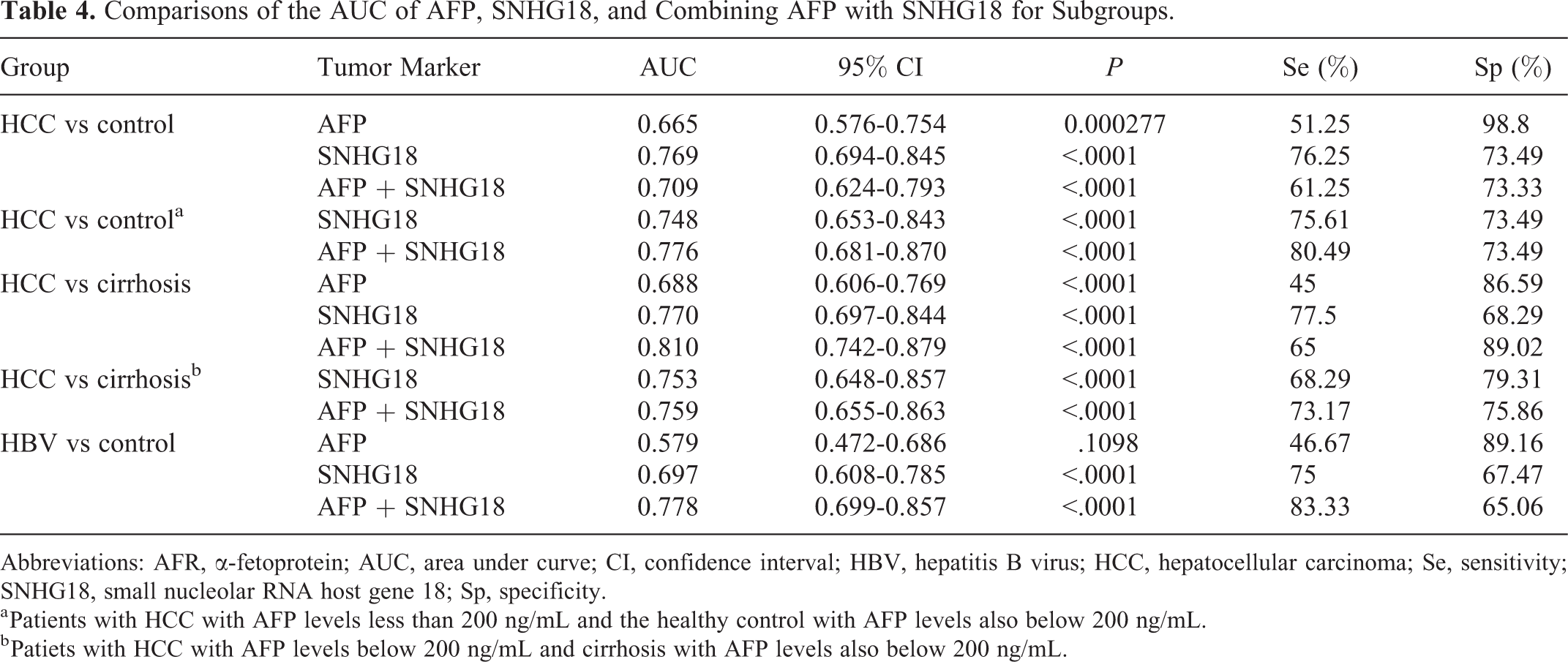
Abbreviations: AFR, α-fetoprotein; AUC, area under curve; CI, confidence interval; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; Se, sensitivity; SNHG18, small nucleolar RNA host gene 18; Sp, specificity.
a Patients with HCC with AFP levels less than 200 ng/mL and the healthy control with AFP levels also below 200 ng/mL.
b Patiets with HCC with AFP levels below 200 ng/mL and cirrhosis with AFP levels also below 200 ng/mL.
Discussion
Noncoding RNAs are frequently reported to be aberrant in various kind of cancers, which can be involved in apoptosis, proliferation, metastasis, angiogenesis, and other processes. 2 Therefore, understanding the relationship between noncoding RNAs and the development of cancer can lay the foundation to discover novel approaches to diagnosis and therapy of tumors. Hepatocellular carcinoma is the most common type of solid tumors worldwide with high invasiveness and poor prognosis. Once related symptoms appear, the patients are mostly in the late stages. 16 For last 40 years, AFP has been used to screen HCC, whose sensitivity and specificity were 39% to 65% and 76% to 94%, respectively. 17,18 Additionally, data suggested that AFP would be seldomly elevated for tumorous mass <2 cm in diameter. 19 Thus, the utility of AFP to detect HCC at early stages has been challenged. Hence, exploring novel biomarkers for differentiating HCC from other liver diseases at early stage is urgently needed. Over the past decade, considerable studies were undertaken to explore the biomarker for HCC. Amounts of attention were focused on noncoding RNAs. In 2016, Zheng et al 14 revealed that the expression of SNHG18 was abnormal in the glioma tissue specimens. Furthermore, high expression of SNHG18 was associated with the progression of primary glioma. Little is known about the role of SNHG18 in HCC. Therefore, it is potentially prospective to explore the value of SNHG18 in HCC.
In the present study, we investigated the clinical and diagnostic value of SNHG18 in patients with HCC for the first time and found that SNHG18 was significantly downregulated in HCC tissues compared to the corresponding noncancerous tissues. Our results also indicated that the levels of SNHG18 were related to the levels of AFP and tumor sizes. By detecting the expression pattern of SNHG18 in plasma, levels of SNHG18 in HCC group were found lower than that of both healthy control and the cirrhosis, consistent with the results in tissues. It was widely known that the development of HCC was a multifactor, multistep, and complex process. 20,21 Unfortunately, despite remarkable difference was found between patients with HCC and patients with cirrhosis, there was no statistical difference between patients with hepatitis B and patients with HCC and cirrhosis and the healthy controls. We may find significant difference by enlarging sample size. Therefore, further researches are necessary. Our present study supports that SNHG18 can help to screen out patients with HCC from the healthy controls and patients with cirrhosis.
Increasing studies in the field of diagnosis and treatment of HCC suggested that circulating noncoding RNAs derived from tumor tissues might be relevant to the tumor and could have the potential value to be used for early diagnosis or survival prediction for HCC. 22 -27 More importantly, the detection of circulating noncoding RNAs in body fluids was considered as a nonintrusive procedure with limited side effects. We assessed the expression of SNHG18 in plasma to analyze the diagnostic value for the first time. The area under the ROC indicated that SNHG18 was helpful for differentiating patients with HCC from the healthy control, with AUC of 0.7694. Itis widely accepted that HBV and cirrhosis constituted important risk factors for developing into HCC. 28 The AUC of SNHG18 for differentiating HCC from cirrhosis was 0.7702. These data showed that SNHG18 could be a good marker in screening HCC. Importantly, it could yield a relatively high sensitivity and specificity to combine SNHG18 with AFP in distinguishing HCC with AFP levels below 200 ng/mL from the healthy controls (80.49% and 73.49%) and patients with cirrhosis (73.17% and 75.86%) whose AFP levels were also <200 ng/mL. This might be useful for diagnosing patients with HCC whose levels of AFP were lower than the standard. However, the limitation of our research was that the sample size was relatively small. Further researches are necessary to verify our results.
A deeper understanding of the mechanism of noncoding RNA in HCC would be helpful to determine new diagnostic markers and therapeutic intervention. Katrin Panzitt et al found that noncoding RNA HULC (highly upregulated in liver cancer) could mediate epithelial–mesenchymal transition (EMT) by upregulating epithelial markers (E-cadherin and β-catenin) and downregulating mesenchymal markers (Vimentin and N-cadherin) in HCC. 29 Thus, HULC could induce HCC cells to activate EMT and then promote tumor progression and metastasis. Caner stem cells (CSCs) were a population of cancer cells, characterized by the properties of self-renewal and differentiation, which had the great potential to form tumors. 30 Studies pointed out that up to 40% of HCC developed from clonal populations originated from hepatic CSCs. 31 Wang et al suggested that noncoding RNA plasmacytoma variant translocation could contribute to the CSC phenotype of liver cancer cells. 32 Lan et al revealed that SNHG12 functioned as an endogenous sponge for miR-199a/b-5p to regulate the expression of MLK3 and affect the nuclear factor κB pathway, through which SNHG12 was associated with tumor progression and metastasis. 15 Regarding SNHG18, it has been documented that upregulation of SNHG18 promoted radio resistance of glioma by repressing SEMA5A protein. 14 In human glioma, Zheng et al and Li et al also reported that SEMA5A protein could inhibit human cell motility and radio resistance of glioma. 14,33 Sadanandam et al previously suggested that SEMA5A protein was constitutively expressed in pancreatic tumors but not in normal pancreas. In addition, high Sema5A expression enhanced tumor cell invasion and aggregation. 34 The studies above suggested that SEMA5A protein could function as disparate roles in different cancer types. Further researches are necessary to explore the functional role of SNHG18 and its connection to SEMA5A protein in HCC. Potentially, SNHG18 can regulate the expression of various proteins via cis or trans regulation mode. The rapid development of RNA sequencing technology provides us an opportunity to explore the relationship between SNHG18 and target proteins in HCC. Additional studies involved in the molecular mechanism are urgently needed.
Footnotes
Authors’ Note
Xue-Fang Liu and Khaing Zar contributed equally to this work.
Ethical approval
All tissue and plasma samples were collected after patients signed their informed consent according to institutional ethical guidelines. This study was approved by the Ethics Committee of Zhongnan Hospital of Wuhan University (Ethical Approval No. 2013059).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Zhongnan Hospital of Wuhan University Science, Technology and Innovation Seed Fund (Project znpy2016046) and National Basic Research Program of China (973 Program) (2012CB720605).