
Abstract
Esophageal squamous cell carcinoma is the sixth most lethal cancer worldwide and the fourth most lethal cancer in China. Tissue-specific transplantation antigen P35B codifies the enzyme GDP-
Introduction
Esophageal carcinoma (EC) remains one of the major cancers worldwide and ranks fourth in terms of cancer incidence in China, 1 –3 where the major histologic type is esophageal squamous cell carcinoma (ESCC). 2 Although there is a steady development in surgical treatment and chemotherapy, the 5-year survival rate of patients with ESCC is still low because most patients with ESCC are diagnosed in the mid-late stage of the disease. 2 Therefore, biomarkers for early diagnosis and detection are much required for ESCC.
The formation of cancer cells is often accompanied by changes in the cytomembrane glycoprotein structure.
4
These glycoproteins or glycosylated structures are often secreted or broken down from the cell membrane; some of them have been used as tumor markers for cancer detection and evaluation of treatment efficacy, such as sialyl Lewis X-I antigen, α-fetoprotein (AFP), and carbohydrate antigen-19-9.
5,6
These studies highlight a requirement for GDP-
Previously, we showed missense mutation frequency of TSTA3 gene was 2% in ESCC. 13 TSTA3 gene is located in a chromosomal locus (8q24.3) that frequently amplifies in ESCC. 14 These findings suggested that TSTA3 gene is closely related to the progression of ESCC. However, the expression and mechanism of TSTA3 in ESCC is unclear. In the present study, we have revealed that increased TSTA3 protein expression was associated with clinical stage and lymph node (LN) metastasis in patients with ESCC. More importantly, increased TSTA3 expression could independently predict poor prognosis for patients with ESCC. Our results indicated that abnormal expression of TSTA3 may contribute toward ESCC progression, and TSTA3 may act as a potential novel biomarker for prognosis of patients with ESCC.
Materials and Methods
Patients and Tissue Specimen
All the 104 ESCC tissues used in the current study were collected during our previous study 13 from patients untreated with neoadjuvant therapy at least for 3 years prior to surgery. The tissues were embedded in paraffin to generate tissue chips for large-scale immunohistochemical (IHC) analysis. Overall survival (OS) was defined as the time interval from primary surgery until death due to any cause or terminal time of follow-up without any death events. Clinical staging of ESCC was determined according to the American Joint Commission on Cancer/International Union Against Cancer TNM-staging system, 7th Edition (2010). Details of clinicopathological features such as histological grade, LN involvement, clinical stage, and TSTA3 of IHC-defined classifications are summarized in Supplementary Table S1.The study was approved by the Shanxi Medical University (approval no 2009029). The informed consent was obtained from all participants.
IHC Analysis
The expression of TSTA3 in tumor tissues was examined by IHC staining. The IHC staining was performed using the Envision Labelled Peroxidase System (Maixin, Fuzhou, China). Briefly, sections were incubated with 1:400 diluted anti-TSTA3 (rabbit polyclonal antibody, ab190002; Abcam, Cambridge, UK) for 14 hours at 4°C. After washing with phosphate-buffered saline, the thrombotic microangiopathies were incubated with the 1:20 diluted secondary antibody (MaxVision HRP-Polymer anti-rabbit IHC kit, KIT-5920; Maixin, Fuzhou, China) at 37°C for 20 minutes, followed by detection using the DAB detection kit (Maixin, Fuzhou, China). After being counterstained with hematoxylin and bluing reagent, all section images were scanned at 100×. Cytoplasmic expression of the TSTA3 protein was determined using fully automatic digital pathological scanning apparatus (Aperio, Vista, CA, USA) and analyzed using Image Scope software v12.0 (Aperio, Vista, CA, USA). Histoscore (H-Score) was calculated by a semiquantitative assessment of both the staining intensity and the percentage of positive cells.
Statistical Analysis
The receiver–operating characteristic (ROC) curve was used to get the optimized cutoff value of TSTA3 protein, which divided the patients into 2 groups: the TSTA3high group and TSTA3low group, respectively. Correlation analysis of TSTA3 expression and clinical pathologic factors was performed with a χ2 test. Survival analysis was carried out using Kaplan-Meier analysis and log-rank test. Univariate and multivariate survival analyses were carried out by a Cox proportional hazards (PHs) regression model after PH-assumption tests. All calculations were performed with SPSS 18.0 for Windows statistical software package (SPSS Inc, Chicago, Illinois). P values <.05 were considered statistically significant.
Results
Expression of TSTA3 Protein in ESCC Tumor Tissues
First, TSTA3 protein levels were measured in 104 primary tumor tissues. The results of IHC showed that TSTA3 was expressed in the cytoplasm of ESCC tissues (Figure 1). The H-Score of TSTA3 protein ranged from 66.3158 to 297.3680 in ESCC tumor tissues, and the median was 184.926.

Expression of TSTA3 in ESCC tumor tissues. TSTA3 indicates tissue-specific transplantation antigen P35B; ESCC, esophageal squamous cell carcinoma.
Relationships Between TSTA3 Expression and Clinicopathological Characteristics in Patients With ESCC
According to the ROC curve analyses (area under curve = 0.709, P = .00037, 95% confidence interval (CI), 0.600-0.818; Figure 2A), all cancer samples were divided into 2 groups: TSTA3low (H-Score <195.2735) and TSTA3high (H-Score ≥195.2735).
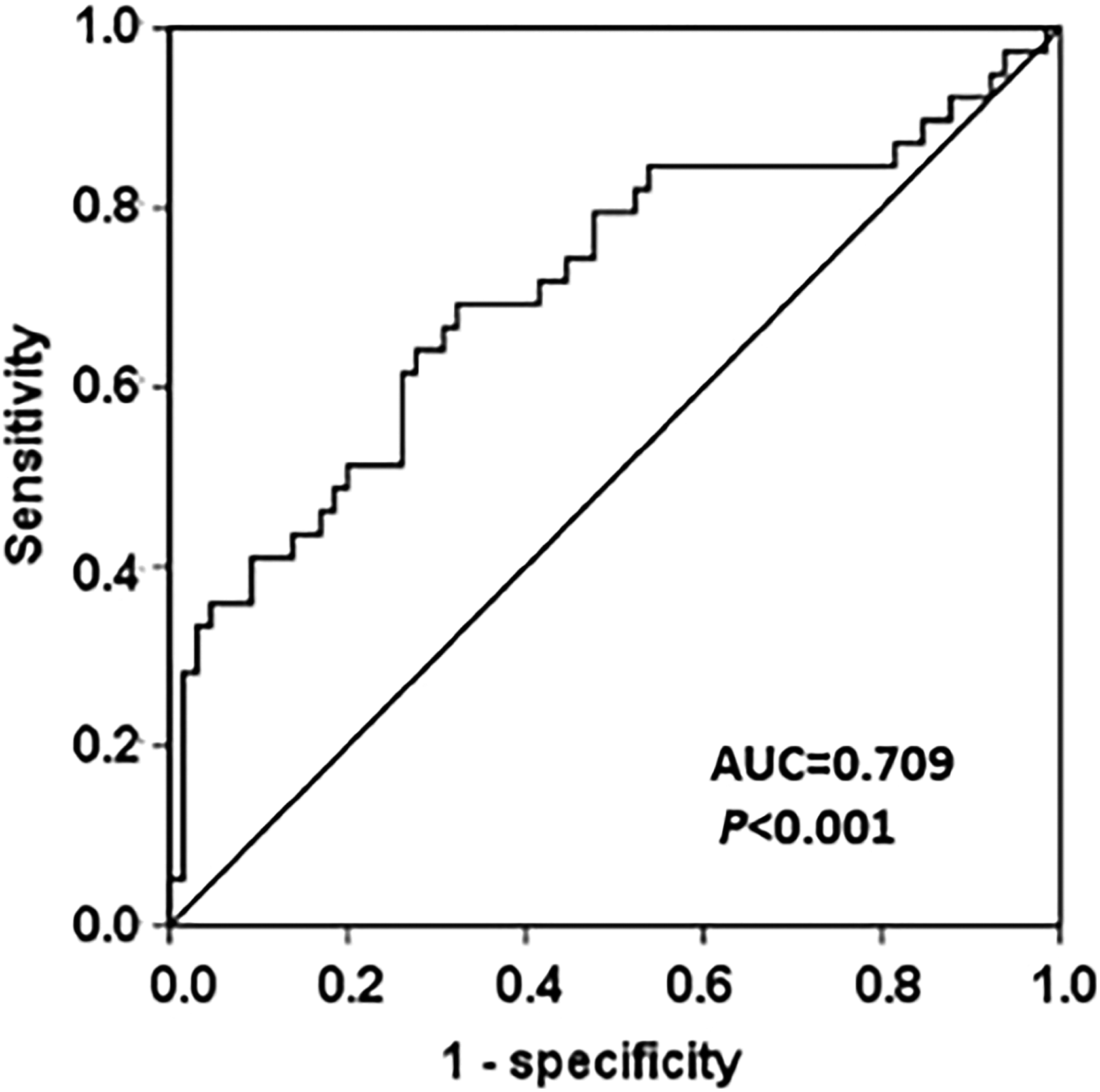
ROC curve analyses of TSTA3 expression in ESCC. The ROC curve analyses showed that the optimum cutoff value was 195.2735 (AUC = 0.703, P = .00037, 95% CI, 0.600-0.818). ROC indicates receiver operating characteristic; TSTA3, tissue-specific transplantation antigen P35B; ESCC, esophageal squamous cell carcinoma; AUC, area under curve; CI, confidence interval.
The TSTA3 protein expression level was associated with age (P = .017, χ2 = 5.983), alcohol history (P = .007, χ2 = 9.817), clinical stage (P = .010, χ2 = 6.996), and LN metastasis (P = .043, χ2 = 4.876; Table 1). No obvious correlations were seen in patients of different gender, histological grade, smoking history, or esophageal site (Table 1). Although the correlation was not statistically significant, TSTA3 protein expression levels tended to have a correlation with invasion depth (T1+T2 vs T3, P = .055, χ2 = 4.131; Table 1).
Association of TSTA3 Levels With Clinicopathological Factors in Patients With ESCC.
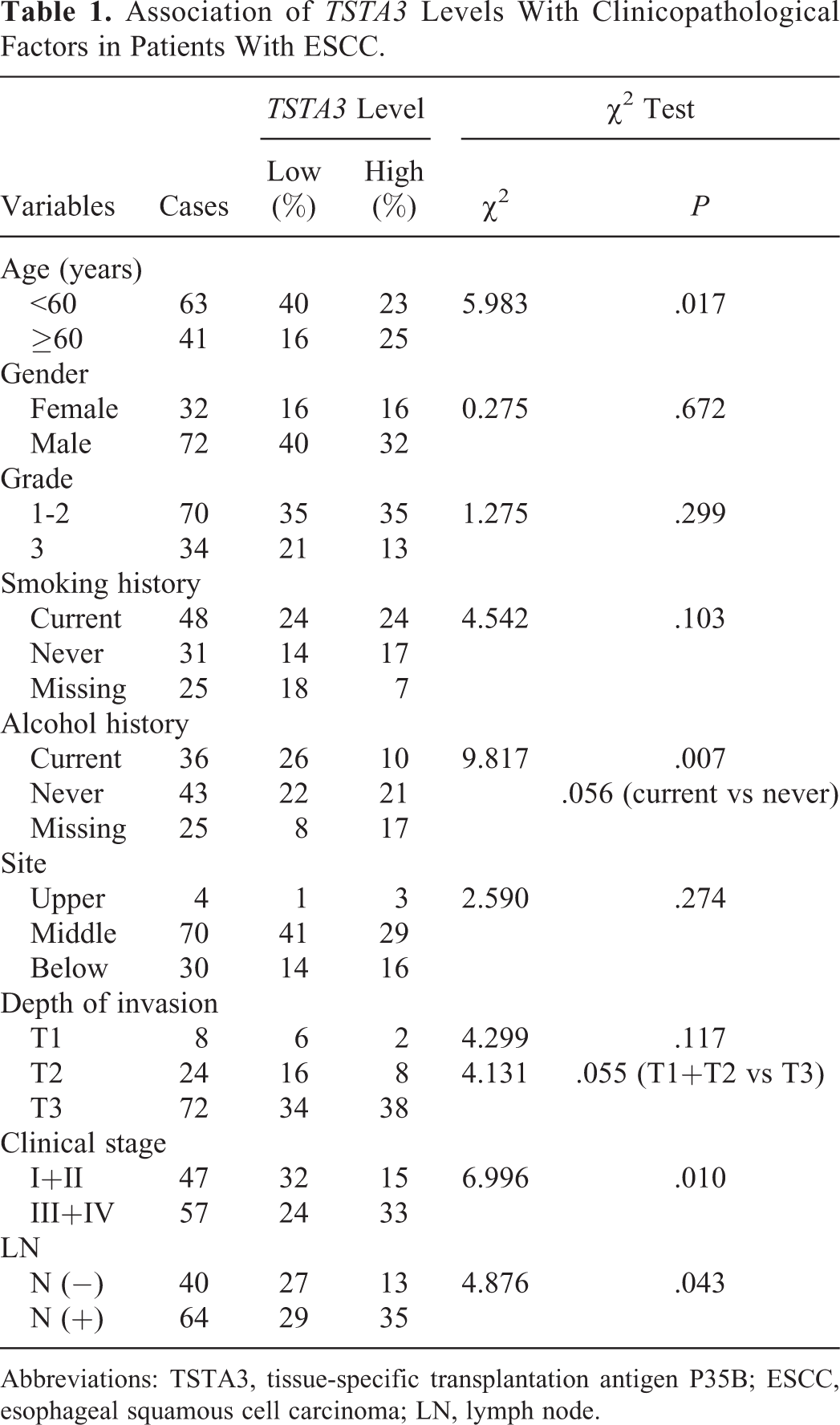
Abbreviations: TSTA3, tissue-specific transplantation antigen P35B; ESCC, esophageal squamous cell carcinoma; LN, lymph node.
Prediction of OS Based on the TSTA3 Protein Levels
The OS of TSTA3low patients ranged from 34 to 55 months, and the median was 45 months. The OS of TSTA3high ranged from 26 to 41 months, and the median was 33 months. Kaplan-Meier analysis showed the patients in the TSTA3low group had a longer survival time than those in the TSTA3high group (P = .048; Figure 3A). The same trend was observed in the patients with ESCC without alcohol history (P = .048; Figure 3B), with grade 3 (P = .020; Figure 3D), and with the lower EC (P = .038; Figure 3E). Such trend was more remarkable only in male patients (P = .017; Figure 3C).

Kaplan-Meier survival curves of patients with ESCC with different TSTA3 protein expression. A, Cumulative OS in the overall study population. B, Cumulative OS in patients without alcohol history. C, Cumulative OS of patients in the female and male groups. D, Cumulative OS in patients with ESCC with grades 1-2 and 3. E, Cumulative OS in patients with ESCC with carcinoma in the upper, middle, and below sites of the esophagus. ESCC indicates esophageal squamous cell carcinoma; TSTA3, tissue-specific transplantation antigen P35B; OS, overall survival.
Cumulative OS of patients in some groups such as old patients (≥60 years, P = .059; Figure 4A), with LN metastasis (P = .064; Figure 4B), or with esophageal full thickness invaded (P = .068, Figure 4C) tended to be affected by the expression of TSTA3. However, there was no difference between the patients with high TSTA3 and the ones with low TSTA3 in clinical stage I+II or III+IV (P = .374 and P = .133, respectively; Figure 4D). Although these trends were not statistically significant, and further study with larger cohort is needed to confirm the findings.

Kaplan-Meier survival curves of patients with ESCC with different TSTA3 protein expression in the different age, LN status, and invasive depth groups. A, Cumulative OS of patients in the age <60 years group and in the age ≥60 years group. B, Cumulative OS in patients with ESCC with or without LN metastasis. C, Cumulative OS in patients with ESCC with T2 and T3 of tumor invasive depth. D, Cumulative OS in patients with ESCC with different clinical stages. ESCC indicates esophageal squamous cell carcinoma; TSTA3, tissue-specific transplantation antigen P35B; LN, lymph node; OS, overall survival.
Univariate and Multivariate Analysis to Determine the Prognostic Value of TSTA3 Protein Levels
To evaluate the predictive value of the TSTA3 expression for OS status in patients with ESCC, univariate and multivariate Cox PH regression models were performed (Table 2) after PH-assumption tests (Supplementary Table S2). The univariate analysis results showed the association between OS and TSTA3 protein levels in patients with ESCC, and the PH of TSTA3high was not statistically significant (hazard ratio [HR] = 1.967; 95% Cl, 0.987-3.923; P = .055). In multivariate analysis with an entered stepwise Cox PH regression model, interferences of other significant factors in Kaplan-Meier survival analysis were eliminated, and the PH of TSTA3high was statistically significant (P = .012). The results showed that TSTA3high was a significant risk prognostic factor for patients with ESCC. The risk of death in TSTA3high patients was HR = 2.816-fold (95% CI, 1.253-6.329) and higher than the TSTA3low patients. According to the study of Lo et al 15 on the difference between univariate and multivariate analysis, TSTA3 protein levels may independently predict poor prognosis for patients with ESCC.
Univariate and Multivariate Cox Models for the Association Between Survival and Clinicopathological Factors in Patients With ESCC.

Abbreviations: ESCC, esophageal squamous cell carcinoma; HR, hazard ratio; CI, confidence interval; TSTA3, tissue-specific transplantation antigen P35B.
Discussion
Esophageal squamous cell carcinoma is one of the major malignancies with poor prognosis because it lacks specific early diagnostic and prognostic markers. Our present study found that the TSTA3 protein expression level was associated with the clinical stage and LN metastasis status. The TSTA3low patients also had a longer survival time than those with a high level of TSTA3, and TSTA3 maybe serve as a potential prognosis marker of ESCC.
The TSTA3, also known as FX, is an NADPH-binding protein 16 and plays a key role in the course of glycosylation. 7 Glycosylation is necessary for regulation of the function of cells and proteins and plays important roles in a variety of biological functions, including cell–cell and cell–substrate interactions, adhesion, cell immunogenicity, and cell signaling. Aberrations of glycosylation are involved in a number of diseases, such as tumorigenesis 17 and chronic inflammation. 18 Fucosylation is one of the most common glycosylation modifications on glycoproteins and glycolipids, and abnormal fucosylation is closely related to the tumor. 19,20 In head and neck, breast, and colorectal cancers, as one of the core-fucosylated-proteins, annexin I can modulate adhesion functions of cancer cells by controlling intracellular calcium release, 21 annexin II can interact with matrix proteins and specific protease to regulate prothrombin activation, cell movement, and adhesion. 22 –24 Expression change in fucosylated glycoproteins has been observed in liver cancer cell lines with discrepant migration abilities. 25 Fucosylation associated with tumor immune escape and deficiency in GMDs can lead colon cancer cells to escape from natural killer cell-mediated tumor surveillance through downregulation of fucosylation. 26,27
As one of the key enzymes in fucosylation, TSTA3 participates in the metabolism of mannose and directly produces metabolites—GDP-
Since most focus glycoproteins are secreted proteins or cell membrane protein on the surface, abnormal glycoproteins on the tumor cells which break away from the primary tumor site or release to blood could be used as a tumor marker. SialylLewisX, with high expression in breast cancer, ovarian cancer, liver cancer, and colorectal cancer, has been proved to be a tumor-associated antigen. 32 –35 Engineering anti-Lewis-Y hu3S193 and IGN311 antibodies have been tested as passive immunotherapy approaches of epithelial cancers and may be applied clinically. 36,37 Core-fucosylated AFP (AFP - L3) compared to AFP has a more specific value of the diagnosis of liver cancer. 20,38 Serum-fucosylated haptoglobin with high levels is considered as a novel prognostic biomarker for malignant tumors, such as ovarian cancer, lung cancer, breast cancer, and pancreatic cancer. 39 –41 Our study also showed TSTA3low patients had a longer survival time than those with a high level of TSTA3, and TSTA3 might be a potential molecular predictor of prognosis in patients with ESCC.
In conclusion, TSTA3 protein levels were correlated with clinical stage and LN metastasis in ESCC and could potentially predict poor prognosis for patients with ESCC independently. As a promising candidate for predicting poor prognosis in ESCC, further research is needed to clarify the mechanism of carcinogenesis and identify the potential clinic applications of TSTA3.
Supplemental Material
Supplemental Material, Table_S1_Information_of_104_ESCC_patients - High TSTA3 Expression as a Candidate Biomarker for Poor Prognosis of Patients With ESCC
Supplemental Material, Table_S1_Information_of_104_ESCC_patients for High TSTA3 Expression as a Candidate Biomarker for Poor Prognosis of Patients With ESCC by Jie Yang, Pengzhou Kong, Jian Yang, Zhiwu Jia, Xiaoling Hu, Zianyi Wang, Heyang Cui, Yanghui Bi, Yu Qian, Hongyi Li, Fang Wang, Bin Yang, Ting Yan, Yanchun Ma, Ling Zhang, Caixia Cheng, Bin Song, Yaoping Li, Enwei Xu, Haiyan Liu, Wei Gao, Juan Wang, Yiqian Liu, Yuanfang Zhai, Lu Chang, Yi Wang, Yingchun Zhang, Ruyi Shi, Jing Liu, Qi Wang, Xiaolong Cheng, and Yongping Cui in Technology in Cancer Research & Treatment
Supplemental Material
Supplemental Material, Table_S2_PH-assumption_tests_of_different_variables - High TSTA3 Expression as a Candidate Biomarker for Poor Prognosis of Patients With ESCC
Supplemental Material, Table_S2_PH-assumption_tests_of_different_variables for High TSTA3 Expression as a Candidate Biomarker for Poor Prognosis of Patients With ESCC by Jie Yang, Pengzhou Kong, Jian Yang, Zhiwu Jia, Xiaoling Hu, Zianyi Wang, Heyang Cui, Yanghui Bi, Yu Qian, Hongyi Li, Fang Wang, Bin Yang, Ting Yan, Yanchun Ma, Ling Zhang, Caixia Cheng, Bin Song, Yaoping Li, Enwei Xu, Haiyan Liu, Wei Gao, Juan Wang, Yiqian Liu, Yuanfang Zhai, Lu Chang, Yi Wang, Yingchun Zhang, Ruyi Shi, Jing Liu, Qi Wang, Xiaolong Cheng, and Yongping Cui in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Authors’ Note
Jie Yang, Pengzhou Kong, Jian Yang, Zhiwu Jia, Xiaoling Hu, and Zianyi Wang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the National Natural Science Foundation of China (81330063 to YC, 81672768 to XC, 81773150 to LZ, 81502135 to PK, and 81602458 to CC), the Key Project of Chinese Ministry of Education (213005A to YC), the Specialized Research Fund for the Doctoral Program of Higher Education (20121417110001 to YC), a Research Project Supported by Shanxi Scholarship Council of China (2015-Key3, 2013-053 to YC), the Innovative Team in Science & Technology of Shanxi (201605D131045-16 to YC), the Program for the Outstanding Innovative Teams of Higher Learning Institutions of Shanxi (OIT 2014, 2015 to YC), and the Key Project of Research and Development Plan of Shanxi (201603D321048 to YC), the Youth Research Fund of Shanxi Medical University (Q02201203 to LZ).
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.