
Abstract
Accurate measurement of blood pressure is very important as high blood pressure is a major cause of cardiovascular disease. Most non-invasive blood pressure measurement systems depend on a blood pressure cuff mostly made of fabrics but these differ widely in geometry and mechanical properties. To investigate the effect of differences in cuff construction on the arterial pressure, a numerical model using DICOM data obtained from magnetic resonance imaging scan is presented. The model arm was loaded with experimentally obtained interface pressures for eight different types of cuffs made of coated woven and non-woven fabrics. Variations of up to 27 mmHg in estimated systolic and up to 17 mmHg diastolic BP were found. Data were collected at inflation pressures between 80 and 130 mmHg to reflect the normal range of human systolic and diastolic blood pressure. Pressure transmission from the arm to the arterial surface was less than 90% under all the blood pressure cuffs except one with a rubber bladder which showed a 95% transmission ratio. The results from this study demonstrate wide variations in the arterial pressure values between cuffs of different types and cuffs supplied by a single manufacturer. It is crucial that a blood pressure cuff applies a known value of pressure around the arm. This study shows that blood pressure measurements may be critically affected by the fabric types used to construct blood pressure cuffs, leading to potentially serious errors in the assessment of cardiovascular risk.
Keywords
Introduction
Pulse rate and blood pressure (BP) are amongst the most frequently measured physiological parameters in clinical practice. Hypertension is the leading treatable cause of death world-wide (7.6 million deaths annually = about 13.5% of global total) [1].
Although direct measurement of intra-arterial BP is more accurate, indirect BP measurement is universally preferred for the sake of safety, convenience and simplicity [2], especially since the introduction of the sphygmomanometric method by Scipione Riva-Rocci in 1896 and use of sounds generated over the brachial artery observed during deflation by Korotkoff in 1905.
In non-invasive (indirect) assessment, blood pressure is estimated assuming that the pressure inside the cuff is the same as that applied to the underlying arterial wall. A sphygmomanometer cuff is inflated above systolic BP after wrapping around the limb and then deflated. Manometric pressure at which blood flow resumes during the cuff deflation is considered the same as arterial systolic BP. The only known pressure registered by the manometer is that in the inflated bladder, which is enclosed between the cuff layers. The pressures exerted on the arm surface and onto the arterial wall usually remain unknown in non-invasive BP measurement. Ideally the pressure transmitted from cuff inner walls to arterial wall should be of same value so that the pressure registered by the manometer during BP measurement indicates arterial-wall pressure. However, this is not the case because the pressure inside the cuff does not directly transmit to the artery. It passes through the cuff inner layer to the arm tissues and then to the artery. Shaw and Murray found that the pressure magnitude decreases with increasing depth of the soft tissues [3]. The visco-elastic characteristic of the arm tissue causes spatial as well as temporal variation of the pressure magnitude. Previous studies have reported that systolic blood pressure (SBP) and diastolic blood pressure (DBP) had been estimated inaccurately by indirect techniques using inflatable cuffs [4–9].
Despite the fact that the BP cuff has been used for many decades, there is no standard method for its construction which varies between and within manufacturers. Currently, a wide variety of BP cuffs are available commercially which differ in terms of design and material properties. This study was carried out to compare performance based on such differences. To avoid the potential discomfort and complications of direct determination of BP under different cuff types by arterial cannulation [10,11] we chose to simulate the process of BP measurement using finite element analysis (FEA) with a geometrically accurate upper arm. It is now possible to predict pressure distribution underneath BP cuffs of different types; after measuring geometric and mechanical properties of fabrics used for cuff construction. The pressure distribution around the arterial wall and within the arm can also be estimated with this technique which is not easily achieved by in vivo experimentation.
The irregularity in geometry of a human body part affects the pressure transfer and stress distribution [12,13]. The mathematical models previously proposed by Cristalli, Ursino and Kim et al. contributed to reducing errors associated with indirect techniques of BP measurement [14–16]. However, their models were deficient in geometric accuracy of the upper limb and simulated the arm as an axisymmetric cylinder except one model that studied pressure transferred in the arm developed by using the Visible Human dataset [17]. This investigation reported that the pressure transmission ratio was only 80%, from surface of the arm to the brachial artery and in this same model the pressure applied over the arm was only 100 mmHg.
Studies were carried out on BP measurement using different cuff types on a metal cylinder and on an anthropomorphic upper arm using FEA on Abaqus which also reported differences in interface pressure (IP) and arterial pressure upon change in cuff fabric properties [18,19].
Geometric accuracy, arterial pressure fluctuation from SBP to DBP at the same frequency as that of human artery, and arm surface loading followed by unloading as with BP measurement using inflatable cuffs were not included in the previous models but have been incorporated in the models proposed in this study. DICOM data were obtained from an MRI scan of the upper arm for development of geometric accurate upper arm using ScanIP [20]. Eight different types of cuffs were selected which differ in terms of fabric used for their construction. Blood pressure measurement was simulated in Abaqus [21] as per British Hypertension Society guidelines [22]. The arterial pressure under eight different cuff types were predicted in the proposed models. For more accuracy, cuff fabric properties, pressure at the interface of cuffs and upper arm were measured experimentally; and applied in the development of the models. Arterial pressures predicted under each cuff type were analysed to investigate the effect of change in cuff fabric construction on BP measurement.
Method
In this study, experimental and numerical investigations are conjoined for the prediction of arterial pressure under the cuffs of different types.
A detailed FEA was conducted in Abaqus [21] using geometrically accurate upper arm model. The parameters of the simulation were kept similar to the actual method of BP measurement to get reliable results and help to identify the errors associated with the construction of sphygmomanometric cuffs. The brachial artery was loaded with pressure fluctuating between 80 and 130 mmHg. In order to achieve reliable results from the numerical model, the pressure inside the cuff was not applied on the arm surface; instead the pressure was found experimentally at the interface of a healthy volunteer’s upper arm and eight different cuff types selected for this study. Oxford Pressure Monitor (OPM) sensors were employed to measure interface pressure (IP). These values were used to load the external arm surface in simulation. After post-processing of the results, the predicted arterial pressure against the external pressure (interface pressure) was analysed under each cuff type during cuff deflation because in auscultation, BP is measured during cuff deflation.
Pressure transmission ratio was also calculated for selected cuffs. The models were able to provide the pressure transmission ratio for eight different types of cuffs.
Development of the numerical model
Following steps were involved in simulating the process of BP measurement:
Step 1: Measurement of geometric and mechanical properties of different cuff types
The BP cuffs selected for this study can be classified in different manners, with and without an inner bladder.
A single cuff with bladder is an assembly of an external sleeve containing an inflatable bladder. The sleeve is an outer shell to accommodate the cuff bladder inside. It is mostly constructed from a plain woven fabric made up of nylon or polyester. The sleeve functions to keep the bladder in situ and to facilitate the closure of the cuff around the limb. The inflatable bladder is the major part of BP cuff. Most cuff sleeves (whether bladdered or bladderless) are constructed from a woven textile fabric but the bladder enclosed is of same material as that of sleeve or of rubber. Cuffs 2, 3 and 4 were of this type (details in Table 1). Specifications of the selected cuffs.

To maintain anonymity of the cuff manufacturers, a random identity (ID) number was assigned to each cuff. The selected cuffs are most commonly used in UK hospitals and clinical practices, and were from two manufacturers – Cuffs 1 to 4 from Manufacturer 1 and Cuffs 5 to 8 from Manufacturer 2. The specifications and ID of the cuffs are listed in Table 1. The only difference between Cuffs 2 and 3 was that the length of the bladder, Cuff 3 was approximately 6 cm longer than that of Cuff 2. The materials and width of both cuffs were the same. Cuffs 6 and 8 were similar to Cuffs 5 and 7 respectively however the sleeve length of the Cuffs 6 and 8 was approximately 12 cm longer than Cuff 5 and Cuff 7, respectively. Cuff sizes were selected to ensure compliance with guidelines whereby the cuff bladder went around 80–100% of the volunteer’s arm circumference.
Cuffs are made of different types of fabrics which are anisotropic in nature and are subjected to wide variety of deformation like creasing and wrinkling upon application of force. The biomechanical functional performance of these cuffs depends on their fabrics’ mechanical properties which can be determined from the constituting yarns and internal structural features [23]. The objective of geometric and mechanical testing was to evaluate different mechanical properties of the cuff fabrics. In previous models, mechanical properties of the cuff were determined by wrapping those either around arm or metal cylinder [5,14,24,25]. In this investigation, mechanical properties of the cuff fabrics were determined independent of the underlying material. If the variation in the properties exists, it is important to find the effect of that variation on sub-cuff pressures.
The mechanical properties of the cuff fabrics were found experimentally using standard test methods [18,19] and are listed in Table 1.
Step 2: Interface pressure measurement
For external loading of the upper arm for simulation models, IP was applied instead of inside cuff pressure. For this purpose, IP was measured at four locations 90° apart (W, X, Y and Z) (see Figure 1) around the upper limb and half way between acromion and antecubital fossa of the volunteer using calibrated OPM sensors under cuffs selected for this study. Arm surface in the simulation model was accordingly divided into four parts and the measured interface pressure was applied. Pressure application locations and sensor positions are indicated by highlighted areas and arrows respectively in Figure 1. Three cuffs were selected for each type and were wrapped around the arm so that the artery indicator was over the brachial artery.
Arm loading corresponding to positions W, X, Y and Z.
Step 3: Geometrical modelling of human upper limb
Average arterial and cuff interface pressure values (mmHg) under the selected cuffs.
In order to make an anatomically accurate arm model, a DICOM data set was generated from MRI scanning of the upper arm of the same volunteer with a circumference of 32 cm.
The slices of the upper arm needed further processing before conducting FEA in Abaqus. Each slice had images of bone, skin, tissues, vessels and fat layer. For analysis, the parts of interest are needed to be separated from the slices to develop a 3D model. This process is crucial as material properties, load, boundary conditions and mesh are to be assigned separately to every part. The following assumptions were made for this purpose:
The arm model developed for the simulation was simplified and comprised the tissues, brachial artery and humerus only. Muscle, skin, adipose tissue and nerve bundles were treated as a combined tissue layer.
ScanIP® was used to process DICOM data which converts DICOM data into 3D volumes/elements which were imported into Abaqus.
Step 4: Finite element analysis using Abaqus
Model description
By developing a numerical model of the upper arm using a real human data set, it was possible to predict arterial pressure under different types of cuff. Non-invasive BP measurement was simulated by loading the arm with measured IP values (as listed in Table 2 and indicated in Figure 1) and then unloaded to zero pressure. Pressure distribution around artery was obtained during arm unloading (depressurising) at cuff pressures corresponding to normal BP values. The arterial pressures at systolic and diastolic were estimated assuming linear pressure variation (gradient/slope) against the IP measured from 155 mmHg cuff pressure to 0 mmHg cuff pressure. Pressure transmission ratio was calculated from the arm surface to the arterial surface under every cuff. The parts of the upper arm imported to Abaqus were tissues and humerus only. The brachial artery was constructed as a hollow cylinder using Abaqus part tools by taking dimensions from previously published literature [26].
Material properties
Mechanical properties of different parts of human upper limb.

The tissue and brachial artery were modelled as solid deformable elements whilst the humerus was rigid.
The focus of the study was on the pressure acting around the artery. After assembling the parts, the surface-to-surface contact was created between the tissues and brachial artery outer surfaces. A tie constraint was applied between the muscle (slave) and the humerus (master) surfaces as muscles are attached to humerus in a real upper arm.
The surface of the arm was divided into four sub surfaces as shown in Figure 1 which is indicated by four arrows. This was done to apply pressure as per values listed in Table 2. The arm and the artery were loaded simultaneously. The arm was loaded to the IP listed in Table 2 and then unloaded to zero. The artery was loaded with pre-specified stable sinusoidal brachial artery pressure of 125/85 mmHg which is under the normal BP range according to the BHS guidelines.
The actual area of interest was the arterial circumference which was also a reference point of mesh saturation. All the parts were meshed with tetrahedral elements. After meshing the parts, a 3D stress approximation and a non-linear static general analysis was performed. Auto stabilisation was implemented for the contact control during the analysis.
Results
To see the pressure variation around the artery under different loading conditions, three nodes (A, B, C) were selected as shown in Figure 2(b). The arterial pressures is plotted for all eight cuffs for the whole duration of unloading (releasing) of cuff pressure (Figure 3). Arterial pressures at the interface of tissue and artery at nodes A, B and C were averaged and listed in Table 2 along with standard deviation.
(a) Upper arm after meshing; (b) loading (pressurising) of upper arm with node location for plotting arterial pressure in Figure 3. Pressure around artery under the cuffs (unloading time is the time during which arm was depressurised).
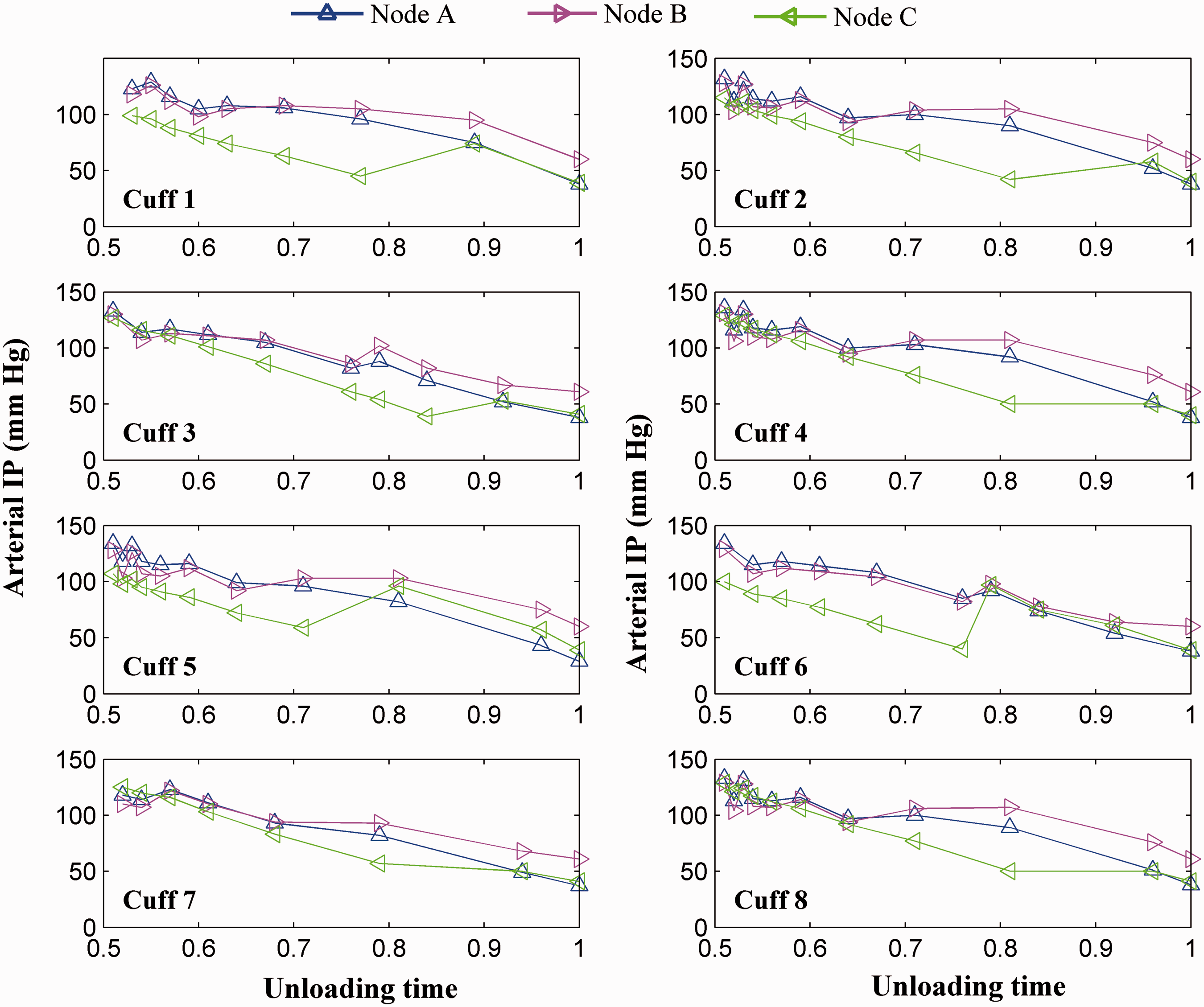
The pressure predicted at the three selected nodes show pressure variation around the artery. Although the geometry of the arm is identical under all cuffs, the variations in IP measurements and mechanical properties of the cuff types led to the variable pressure transfer from the tissues to the artery under the cuffs selected for this study. To find the variations in BP values under different types of cuff, pressures of the three selected nodes over the artery were averaged and plotted in Figure 4:
Full load (FL): Cuffs were inflated to 155 mmHg Systolic Pressure (SYS): Cuffs were deflated and had 81% of the FL pressure Diastolic Pressure (DIA): Cuffs were further deflated and had 55% of the FL pressure
Arterial pressure under different cuff types corresponding to Full load (FL), Systolic pressure (SYS) and Diastolic pressure (DIA).

Grouping of cuffs as per range of SBP and DBP (BHS guidelines).

SBP: systolic blood pressure; DBP: diastolic blood pressure.
The highest average value of SBP is found under Cuff 4 which is 122 mmHg whilst the lowest average value of SBP is found under Cuff 1 which is 95 mmHg. Cuff 4 is a cuff with a rubber bladder whilst Cuff 1 is a bladderless cuff. The results indicate that using the selected cuffs SBP could vary by up to 27 mmHg and DBP by 17 mmHg.
In the present simulation, the transmission ratio was calculated under the eight different cuffs at four unloading times (Figure 5). The pressure transmission ratio is the ratio of the pressure (average) on the surface of the upper arm to the pressure transmitted to the artery during cuff unloading (depressurizing) and varies between 76% and 88% for SBP.
Pressure transmission ratio.
The pressure transmission ratio for DBP is further augmented and goes above 99%, except under Cuffs 3 and 6. A transmission ratio above 100% indicates the artery is fully opened underneath the cuffs. Transmission ratios less than 100% indicate that the artery is open or partially open.
Discussion
The accuracy of cuff based BP measurement has always been a topic of debate but has usually been assumed to be within acceptable limits. Previous models have ascertained that the pressure distribution inside the arm varies with mechanical properties of the skin and muscular tissues and brachial haemodynamic [5,26]. Inaccuracies related to the inflatable cuffs have been largely attributed to cuff size and the observer’s auditory acuity [4,10,28–31]. However, the current study reveals that differences in cuff fabric construction, related geometric and mechanical properties have strong effects on pressure distribution underneath the cuff and thus potentially on BP measurement.
A more detailed simulation model of the non-invasive measurement of the BP using DICOM data (obtained from MRI scanning) is developed for the prediction of arterial pressures (SBP and DBP) under different types of cuffs. The mechanism of BP measurement using cuffs during auscultation was simulated as recommended in BHS guidelines. The artery was loaded (pressurised) with pre-specified stable sinusoidal brachial artery pressure of 125/85 mmHg. For a more realistic representation, instead of applying the recorded pressure inside the cuff, the model was subjected to experimentally derived IPs between the eight cuffs and the arm of a single volunteer. The results of the simulation reveal that pressure output around the artery under different cuffs is neither identical nor uniform around it. Cuff construction and the associated material properties have direct effects on the registered BP values.
Nodal pressure variations
Nodal pressures provide information about the pressure distribution around the artery under selected cuffs (Figure 3). Consider pressure variation from the start of unloading to the DBP, i.e. to 73%: the nodal pressure shows the pressure around the artery is non-uniform and varies under cuff to cuff. The pressure at node C is less than the pressure at nodes A and B in all cuffs till Diastolic pressure (DIA). Node A is in the centre of the arm and is supposed to be under the artery index to get maximum cuff pressure. Under Cuff 1, the pressure at node B was higher than node A. Such a cuff is unable to apply high pressure over the artery. The pressure variations are wide amongst the nodes in the same cuff. The spread of nodal pressures is narrow and the pressure distribution is uniform around the artery under Cuff 4, followed by Cuff 7 and Cuff 8.
The reason of the non-uniform pressure distribution around the artery is the result of non-uniform pressure distribution around the arm by the selected cuffs as shown in Table 2. Cuff 4 is constructed of woven fabric enclosing rubber bladder whilst Cuff 7 and Cuff 8 are also of woven fabric however bladderless. Pressure distribution in woven fabric cuffs is more uniform compared to the cuff constructed of non-woven fabric cuffs; owning to the difference in construction of woven and non-woven fabrics. Another reason is the irregular shape of the arm which may also affect the pressure inside the tissues. However, the first reason is more valid otherwise the nodal pressure would be identical under every cuff investigated.
Effect of geometric and mechanical properties
The effect of the cuff properties solely on the BP measurement can be easily understood with the aid of the simulation models presented in this study. The simulation demonstrates a strong relationship between the elastic modulus of the cuff fabric and the predicted arterial pressures (pressure at the interface of the arm tissues and the main brachial arterial wall). The highest predicted systolic arterial wall pressure (122 mmHg) was found with Cuff 4 and the lowest (95 mmHg) with Cuff 1. The difference of arterial pressure (27 mmHg) would dangerously misclassify the BP level.
Considering two-piece (bladdered) cuffs (four layers of fabrics), the maximum difference was observed to be 14 mmHg between Cuff 4 and Cuff 2. The size and sleeve material of both cuffs are alike. The only difference is the first one has a rubber bladder whilst the second has a fabric bladder. Amongst one piece (bladderless) cuffs, the maximum difference was 19 mmHg. The highest pressure was from Cuff 7 which had Young’s modulus of 154 MPa whilst the lowest pressure was from Cuff 1 with Young’s modulus of 220 MPa. Cuff 5 had the lowest modulus (100 MPa) but predicted an arterial pressure in between Cuff 1 and Cuff 7. A comparison was made between two similarly woven cuffs in order to find a relation between the cuff fabric elastic modulus and the pressure distribution. Cuff 7 had a higher arterial pressure than Cuff 1 but the elastic modulus of Cuff 7 was 43% less than Cuff 1. With an increase in elastic modulus, the arterial pressure reduces. The differences in elastic modulus of cuff fabric give rise to differences in arterial pressure measurement.
For diastolic arterial pressure, the maximum difference was 17 mmHg between a rubber bladdered cuff (Cuff 4) and bladderless cuff constructed of non-woven fabric (Cuff 5). The mechanical properties of cuff fabric vary greatly as rubber is highly elastic whilst non-woven fabric cuffs are stiff and less compliant than woven fabric. The minimum difference of arterial pressure between the bladdered cuffs was 5 mmHg. Measurement of DBP above a margin of 5 mmHg than normal may classify a person as hypertensive [32]. It may misclassify a normotensive person as a hypertensive or vice versa, potentially leading to complications associated with erroneous BP measurement [33,34]. It is to be noted that only eight cuffs were investigated in this study whilst there are numerous types of cuff available and used worldwide. Variations in the geometric and mechanical properties of the cuff fabric impart large variations in estimated intra-arterial pressure. It is highly desirable to design new fabric type and materials for BP cuffs which are capable of exerting uniform pressure over the brachial artery.
Low pressure transmission underneath the cuffs
The magnitude of the pressure acting centripetally decreases as it passes from the cuff inner layer in to the arm tissues. As the pressure goes deeper inside the tissues and reaches to the arterial wall, the pressure reduces even further from the IP until the diastolic point. To quantify this, the pressure transmission ratios were calculated for each cuff (see Figure 5). This shows that the pressure acting over the arterial wall is less than the corresponding pressure applied over the surface of arm and that the magnitude of the pressure acting over the artery is not identical for different cuffs. Although the geometry and mechanical properties of the arm were unchanged under every cuff, the effect of the mechanical properties and construction of the cuff fabric is quite pronounced. Cuff having woven fabric sleeve enclosing a rubber bladder has the highest value of transmission ratio.
For indirect BP measurement to be accurate, the transmission ratio should be 100% or a known fraction of the pressure inside the cuff, as this pressure measured by a manometer or otherwise is assumed as the BP of an individual. It was found in this study that inside cuff pressure is significantly greater than pressure predicted over the artery during BP measurement as previously described [3].
Non-uniform pressure around arm
The IP distribution around the arm is non-uniform as found experimentally (Table 2). The pressure transfer under the cuff depends on the elastic modulus of the fabric. As shown in Figure 6, cuff fabrics get wrinkles during loading and this pattern of wrinkling varies from cuff to cuff. Cuff 5 (non-woven, Figure 6a) is stiffer than the other cuffs. It shows wrinkles only in the inner layer whilst the outer layer is fully stretched. Two other cuffs that are shown were constructed of woven fabric – Cuff 7 and Cuff 8 in Figure 6(b) and 6(c) respectively – exhibited deformation in both layers. The difference in cuff layers wrinkling/deformation affects the pressure distribution underneath. There are regions under the cuffs which are not in contact with the arm; hence there is a possibility of low pressure transmission. This emphasises the need to re-engineer cuff fabric to apply the required pressure more uniformly over the region of the arm bearing the brachial artery.
Distortion during loading. (a) Cuff 5. (b) Cuff 7. (c) Cuff 8.
Conclusions
This research addresses an area which has been overlooked in the past. The effect of geometric and mechanical properties of different blood pressure (BP) cuffs on estimation of arterial BP is shown through simulation of BP measurement on a geometrically accurate human upper limb. By using the simulation model, it was possible to demonstrate the variation in arterial pressure under different cuff types (constructed of fabrics having different geometric and mechanical properties) and provide a more detailed picture of pressure distribution around the artery than those used in previous studies. This suggests a possible means to improve sphygmomanometric cuff design.
Cuff manufacturers should consider assessing pressure transmission ratios for better BP measurement either assessed manually or using automatic devices. Since hypertension is a major world-wide problem affecting millions of people, its accurate estimation is imperative and needs further attention. The methods of measurement, equipment and the size of the cuffs have already been standardised but the cuff fabric construction and the material of the cuffs which are the cornerstone of accurate BP measurement have been neglected. Validation of our numerical analyses would require invasive intra-arterial pressure to be measured. The numerical model can also be improved by incorporating nonlinear material properties of the cuff and “fluid–structure interaction”.
Footnotes
Acknowledgements
We are thankful to the Magnetic Resonance Imaging Facility (MRIF) of Wellcome Trust Clinical Research Facility (part of the School of Cancer and Enabling Sciences, University of Manchester) for help in obtaining the MRI scan data; and Dr. David Jimenez Cruz for his help in developing the geometric model using DICOM data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are thankful to NED University of Engineering & Technology, Karachi, Pakistan for funding this research project through Higher Education Commission of Pakistan.