
Abstract
The use of passive coatings could be a new solution to improve the cleaning potential of interior textiles in hospitals. In these years, the scepticism toward the use of antibacterial textiles in the health care sector is emerging, and in the Nordic countries, the implementation success is confined. From this perspective, the purpose of this paper is therefore to address focus on alternative passive coatings that without actively killing the bacteria provide a hydrophobic and easy-to-clean textile surface. The paper relates to an in-situ study evaluating the effect and cleaning potential of SiO2-coated textiles compared to traditional textiles and a hard plastic surface as a reference material. Through the study, arranged at an outpatient lung department at Hospital Vendsyssel, Denmark, five different surface materials were installed on hospital chair armrests and sampled with microbiological contact plates through a three-week period. By determining the level of contamination on these surfaces, the study illustrates that the SiO2-coated textile is possible to clean to an acceptable level below the critical limit value of 2,5 Colony Forming Units (CFU) per cm2. In comparison, the traditional textiles were only cleaned to the acceptable level in 56% of the microbiological controls, while the regular hard plastic surface only had acceptable levels of contamination in 25% of the samplings.
Introduction
Traditional textiles have long been known as a potential bacteria reservoir increasing the risk of spreading nosocomial infections [1–5]. As a response to this hygiene risk of using traditional textiles, an increased emergence of antibacterial textiles has been introduced to the health care market in recent years [6]. In a range of in vitro studies, these antibacterial textiles have proven their efficiency in reducing and eliminating bacteria growth [7–9], and in situ studies have also shown an, although less significant, effect in the real-life hospital context [10, 11].
The market penetration of these antibacterial textiles has in a period of years been extensive in both the health care sector and in a range of consumer products [1], but in these years, an increased scepticism toward these antibacterial textiles has developed in the Nordic countries [12–14] especially concerning the lack of knowledge on the potential increase of bacterial resistance and potential environmental issues [15–17]. As a consequence, Denmark, as one of the specific countries, has currently no desire in using antibacterial textiles in the health care sector [13].
Instead, interior textiles in hospitals are replaced by plastic-coated upholstery that may increase the cleaning potential, but not without confining the patient comfort, and challenging the architectural visions of an accommodating and supporting physical environment [18].
New materials and technologies, however, already exist, and based on alternative passive strategies, the interior textiles can be coated with a hydrophobic and easy-to-clean surface [14]. Based on these passive strategies, the bacteria are not affected actively or killed, and will therefore not directly induce the risk of increased bacterial resistance [14].
Coated textiles, containing hydrophobic properties, have in recent years received increased commercial interest, and focus has been directed toward the development of more environmental friendly and durable coatings [19]. However, despite the use of these passive coatings in the field of apparel, or even on hard surfaces in the food industry [20], the experience in the hospital context is rather limited [21]. To broaden the field on the application of these passive, nonantibacterial textile coatings in the health care market, this paper will specifically explore if a coating of SiO2 can provide a textile surface with an improved cleaning ability.
In regard to the environmental awareness in the hospital context, the SiO2 coating is considered a suitable solution, as this fundamentally is based on a fluorocarbon-free technology. The coated textiles are generally designed to prevent fluid permeation and to restrict bacterial growth [22], and they will potentially contribute to a more cleaning-friendly hospital interior. The specific effect of the cleaning potential was investigated in an in situ study at a Danish hospital. Aiming to evaluate the effect of nonantibacterial SiO2-coated textiles in hospital interiors, focus in this study is directed toward hospital upholsteries as they are considered to constitute the critical challenge in regard to cross-contamination and nosocomial infections.
Methods
Premises
As the purpose of this study is to conduct an in situ test on the cleaning potential of SiO2-coated textiles in hospital interiors, the specific premises for the study should be in continuous use during the day to increase the necessity for cleaning. Therefore, a demarcated waiting room at the outpatient lung department, Sygehus Vendsyssel (Hospital Vendsyssel), Hjørring, Denmark, was settled as the specific context. To represent the “worse-case-scenario” of upholsteries, the different textiles were installed on the armrest of existing hospital chairs (Figure 1). Here the patients’ hands are in direct contact with the chairs, which constitute the greatest risk of cross-contamination. The specific premises offered a broad patient mix and an ongoing flow of patients, and this constant people traffic was important to have all the different chairs frequently in use.
Materials
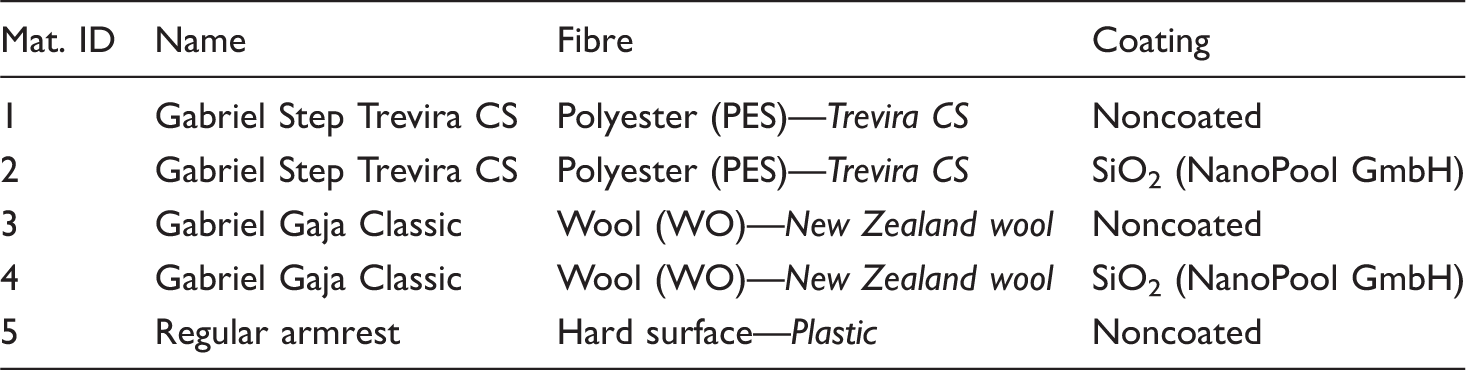
Materials for the test included a Trevira CS polyester-based (PES) and a WO-based (WO) textile, Gabriel Step Trevira CS, and Gabriel Gaja Classic, respectively. Designed for upholsteries, both fabrics had similar weight (336–378 g/m2) and being plain weaved the textile design defined the same surface structure.
Nobicon A/S, Danish distributor of the NanoPool GmbH “liquid glass coating,” performed the water-based SiO2 coating that contains SiO2 molecules as the functional ingredient. The solution is sprayed on the textile surface and is allowed to dry for 24 h at 20℃. As illustrated in the Figure 2, the coating is active at fibre level, and in low concentration (2–10% of SiO2), the solgel-processed coating forms an 80 - to 100-nm thin glass membrane at the surface of the textile fibres. This passive coating of SiO2 performs hydrophobic and defines an easy-to-clean surface that prevents bacteria growth [23–25]. Contact angles are determined for water droplets as 135 ± 4° for the coated WO fabric, and 128 ± 4° for the coated PES. Despite the hydrophobic properties, the textile handling is maintained in full, and there is no visual or tactile difference in the coated versus noncoated textile surface.
Illustration of the armrest where five different surfaces were installed during the test study. SEM images of WO fibres: (a) noncoated standard WO fibre and (b) WO fibre coated with SiO2.

Overview of the five different surfaces tested.
Surface sampling and cleaning procedure
In the in situ study, the bacterial contamination of the various material surfaces is naturally not controlled, and to evaluate the cleaning potential, the surfaces were sampled before cleaning and after cleaning to determine the bacteria reduction.
Cleaning the armrests was performed according to current hospital practice, using the currently valid cleaning procedure defined by the required national guidelines and standard “Infection control in the health care sector—part 10 requirements for cleaning” [26]. The surface was thus cleaned by damp wiping with a clean cloth and clean water containing a cleaning agent, with mechanical rubbing of the surface [26]. Following this cleaning process, the surfaces were allowed to dry for 20 min before resampling the surface for the after cleaning control. During this time frame, the chairs and the waiting room were not in use.
Through the test study, surface samples were collected after 24 h, 48 h, one week, and three weeks after installation of the textiles in the waiting room.
Microbiology
TTC Total Count Dipslides (Transia GmbH) were used for the surface sampling. As the potential risk of nosocomial infections transmitted through surface materials is related to the contact between patient and surface, dipslides with contact agar plates were found suitable for the microbiological sampling. The dipslides were flexible at the base and granted a firm and evenly pressure against the surface being sampled. The dipslides had two independent sides (side A and side B). Both sides contained culture media for total count of microbial presence, and to expand the specific sample area of each tested surface, sides A and B were pressed against the surface on two different places. For each surface, two microbiological samples (side A and side B) were thus collected, and both samples are presented in the results (Table 2). Immediately after the sampling, the dipslides were placed in the original container, and the lid was closed tightly and stored in a lightproof container for transportation. Prior to incubation, the lid was opened, and the dipslides were incubated in aerobic conditions at 35℃ for 72 h, according to manufacturer’s recommendation. The microbial growth was quantified as <2.5 CFU/cm2 = scanty contamination (S); 2.5–5.0 CFU/cm2 = light contamination (L); 5–15 CFU/cm2 = moderate contamination (M); and >15 CFU/cm2 = heavy contamination (H), inspired by the manufacturer’s instruction (see Figure 3 for illustration).
Picture of dipslides after 72-h incubation: (a) heavy contamination and (b) scanty contamination. Results from surface sampling on five different armrest surfaces. Note: Contamination levels: (S): < 2.5 CFU/cm2; (L): 2.5–5.0 CFU/cm2; (M): 5.0–15.00 CFU/cm2; (H): > 15 CFU/cm2. Sides A and B refer to the dipslides two independent sides (both used on the same textile surface).

This categorization enabled the results to be analyzed according to the present standards for microbiological control and evaluation of cleanliness on hospital surfaces [26], where the limit value for total CFU/cm2 shall be ≤2.5 for evaluating whether the tested surface would pass or fail.
Results
Five different surfaces were tested through a three-week period, and a total of 80 samples (40 before cleaning and 40 after cleaning) were collected in the in situ test. Figure 3 illustrates the difference between a sample of heavy contamination (>15 CFU/cm2) and a sample of scanty contamination (<2.5 CFU/cm2). Before cleaning, 67.5% of the sampled surfaces were contaminated on a level ranging between light and heavy contamination, and would thus have failed the microbiological control as stated in valid standard of hospital cleaning [26]. After cleaning, 32.5% of the samples still revealed a light contamination and were above the critical limit value of 2.5 CFU/cm2 (scanty contamination).
As illustrated in Table 2, the armrest surfaces perform quite differently on the standard cleaning procedure. Only 56% of the traditional textiles are reduced to scanty contamination (S) by the damp wiping, while all the SiO2-coated textiles were cleaned to an acceptable level.
The traditional textiles had after one week reached a medium level of contamination, and it was only traditional PES that reached the critical limit value after cleaning. In comparison, the SiO2-coated textiles were after three weeks categorized with moderate and heavy contamination before cleaning, but it was here possible to clean the surfaces to a level of scanty growth.
The percentage of surface samplings that reach a bacteria level below the critical limit value of 2.5 CFU/cm2.

As the results indicate, the reference material, the existing armrest of plastic, only reached acceptable level of scanty growth in 25% of samples after cleaning, and was in this in situ study actually deficient in maintaining a proper hygiene level. In comparison, the traditional WO and traditional PES passed the microbiological control in 62.5% and 50% of the samples, respectively. Only the SiO2-coated textiles reached the acceptable level in all of the tests after cleaning, and were even below the critical limit in 37.5% and 62.5% of the samples before the cleaning procedure.
Discussion
Cleaning of hospital furniture is a high priority for hospital hygiene [26] and as 10% of all hospitalized patients in Denmark are affected by nosocomial infections [27], there is an extensive call for improving the cleaning potential of interior materials. The survival rate of bacteria is generally prolonged on both textiles and hard surfaces [2, 3, 28], and traditional textiles have long been known as a potential bacteria reservoir [1], where the cleaning of the structural surface may be difficult [29].
The immediate solution of replacing traditional textiles with full-coated plastic, as seen in hospitals today, is simultaneously resulting in more clinical and institutional interiors, contradicting the new design visions of healing architecture [18]. Neither the antibacterial textiles seems to be the solution, as the increased scepticism toward these materials is gaining ground especially in Denmark and other Nordic countries [12, 14].
New technologies in the field of passive textile coatings have therefore been proposed with this study, and as it appears from the results of this in situ test, the potential of these technologies seems promising. Even with high initial contamination levels (medium–high contamination), the SiO2-coated textiles were possible to clean to an acceptable level below 2.5 CFU/CM2.
In this study, it was only the coated textiles that were possible to clean in accordance to the valid national standard [26], while neither the traditional textiles nor the regular plastic armrest were adequately cleaned by the standard cleaning method.
Only in 25% of the samples, the plastic armrest was below the critical limit value after cleaning, although the bacterial growth was at the borderline in all cases. Based on this in situ test, Noskin et al.’s [29] observations on the challenge of cleaning traditional textiles are recognized. However, this study found it possible to clean the coated textile, and this improved cleaning potential seems to be worth further studies. Additional long-term in situ studies in new contextual areas are thus considered relevant, while also the disinfection potential of these coated textiles needs to be examined. In Noskin et al.’s [29] study on vancomyocin-resistant enterococci contaminated hospital chairs, a standard disinfectant (quaternary ammonium solution) was not successful in disinfecting the fabric, and alternative disinfection methods thus need to be investigated. In Denmark, the combination of steam and ultrasound has recently been adapted at a Danish hospital for the purpose of disinfecting hospital mattresses [30] and also nontouch room disinfection, based on e.g., damp of hydrogen peroxide, is used in hospitals for disinfection today [31]. These alternative methods for disinfecting the textiles are thus considered worth further attention, and due to the costs of traditional washing, and a general limited washing durability for the SiO2 coating (five wash cycles, according to modified ISO 6330:2012; 80℃ in 10 min), additional research in these aspects would be essential before hospital implementation. Additionally, the abrasion resistance of the coated textiles is an area of concern, where future research and logistic hospital planning should propose new directions for use in the hospital environment. While the tested fabrics itself resist 50,000 Martindale (WO) and 100,000 Martindale (PES), the abrasion resistance of the SiO2 coating is limited to 15,000 Martindale, before increased wettability is observed. In order to implement these coated textiles in the hospital environment, a new logistic process for maintenance of the coated textile surfaces should therefore be developed. The textiles may for that reason be recoated according to the use of the specific furniture, although this fundamentally adds to the costs of general hospital maintenance. However, architectural research on hospital design shows that the physical environment influences the patients’ healing process [32], and here the qualities of interior textiles could potentially promote the architectural experience [18], which would justify the costs of the coatings’ maintenance. With this pilot study, focus has been directed on the passive coatings for hospital interiors, and the evaluation of the cleaning potential of SiO2-coated textiles indicates that the coating provides an easy-to-clean surface that can maintain the high standards of hospital hygiene.
Conclusion
This in situ study on the effect of passive coatings on the surface cleaning potential, showed a substantial difference between the five tested surfaces. Only the SiO2-coated textiles were possible to clean to an acceptable level below the critical limit value of 2.5 CFU/CM2. Neither the traditional textiles nor the regular plastic armrest were cleaned to an adequate level. Relating to this study, the use of interior textiles seems to be enabled by applying a passive coating, providing a hydrophobic, easy-to-clean surface that improves the daily cleaning potential.
On the basis of this pilot study, it is therefore advised that research on the application of these passive technologies is progressed. Additional long-term in situ studies and laboratory tests on disinfection are however still considered pivotal before a final recommendation.
Footnotes
Acknowledgement
The authors of this paper would first of all like to thank the service department at Vendsyssel Hospital, Hjørring, Denmark, for participating in this in situ study. Our acknowledgement also includes Gabriel A/S, for providing textile materials for the tests, and Nobicon A/S for giving the opportunity to test the SiO2 coatings in the hospital environment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.