
Abstract
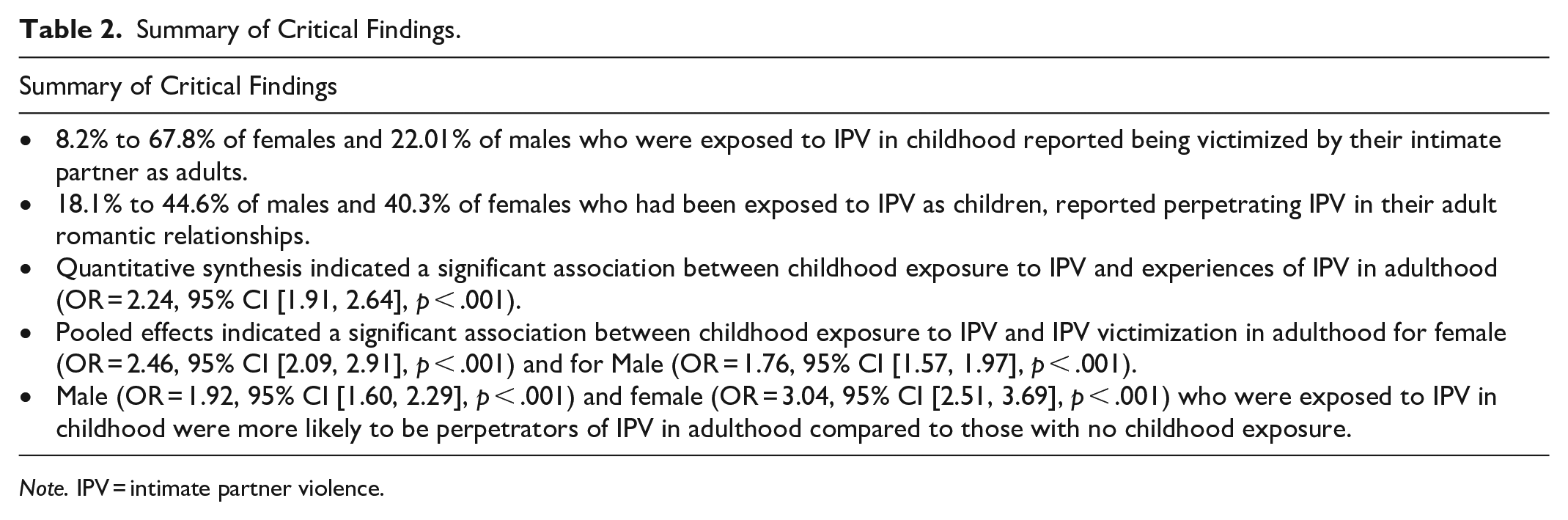
Intimate partner violence (IPV) is widespread in many African countries. Evidence, mainly from Western countries, shows that exposure to IPV in childhood is an important risk factor for experiences of IPV in adulthood. However, to date, no systematic review has synthesized the evidence on this association for individuals living in Africa, which is the goal of the current study. We used three search strategies: database searches (e.g., MEDLINE and PsycINFO), manual searches, and machine learning tools (e.g., Connected Papers). We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and included peer-reviewed studies (in French or English) that reported quantitative or qualitative associations between childhood exposure to IPV and later IPV victimization/perpetration. A total of 48 studies from 29 African countries were included (N = 520,000 participants). Pooled effects indicated an association between childhood exposure to IPV and IPV victimization for females (odds ratio [OR] = 2.46, 95% CI [2.09, 2.91], p < .001) and males (OR = 1.76, 95% CI [1.57, 1.97], p < .001). Similarly, males (OR = 1.92, 95% CI [1.60, 2.29], p < .001) and females (OR = 3.04, 95% CI [2.51, 3.69], p < .001) who were exposed to IPV in childhood were more likely to perpetrate IPV compared to those with no childhood exposure. Effect sizes varied substantially across studies (0.89–5.66), suggesting that other risk factors should be considered in future studies. This review provides unique insights on cycles of IPV in Africa that may usefully inform practice and research.
Keywords
Intimate partner violence (IPV; physical, sexual, and emotional violence by a current or former spouses or dating partners) is regarded as a major public health problem worldwide due to its lifelong adverse consequences (Stewart et al., 2021). Africa has some of the highest prevalence rates of IPV—36%—which is above the global average of 30% (García-Moreno et al., 2013). In 2021, the rate of intimate partner homicide in Africa was estimated at 2.5 per 100,000 females, compared to 1.4 in America, 1.2 in Oceania, 0.8 in Asia, and 0.6 in Europe (UN Female, 2023). The economic burden of IPV on African society, as well as the negative psychosocial consequences, is substantial. For example, medical expenses and productivity that was lost following an episode of IPV in Sub-Saharan Africa is estimated to range from $29.72 USD to $2,151.48 USD (Vyas et al., 2023). Several studies have shown that childhood exposure to IPV can lead to victimization or perpetration of IPV in adulthood, a phenomenon described as cycles of IPV (Hinsberger et al., 2016; Velloza et al., 2022). However, while many studies conducted in Africa were published over the years, no recent review qualitatively and quantitatively synthesizing this literature exists, limiting our ability to draw conclusions about the magnitude of this phenomenon to orient interventions in African countries, and to plan future research endeavors aiming to fill the gaps in our knowledge.
State of Research on Cycles of IPV
A large body of research supports the hypothesis of cycles of IPV described as a situation in which individuals exposed to IPV during childhood (i.e., seeing, hearing, or perceiving the aftermath of interparental violence) are more likely to experience IPV in adulthood (Kimber et al., 2018). Children exposed to IPV may learn that violence is an acceptable way of functioning or resolving conflict within a couple, and this acceptability or tolerance may increase their risk of becoming perpetrators or victims when they reach adulthood (Chernyak et al., 2020). For example, research comparing males who were exposed to IPV during childhood to males who were not highlighted that those exposed to IPV were more likely to approve of violence, and to perpetrate sexual and physical violence in intimate relationships in adulthood (Gupta et al., 2008; Ringwald et al., 2022). Similarly, females who have seen their mother beaten by a male partner during childhood were more likely to normalize and tolerate this in later intimate relationships (Mhelembe et al., 2022). Thus, the experience of IPV in childhood may be an important risk factor that can pave the way for cycles of violence (Cervantes & Sherman, 2021).
The existence of these cycles of IPV has been confirmed in previous reviews, with most evidence coming from high-income countries (Kimber et al., 2018; Smith-Marek et al., 2015; Stith et al., 2000). However, despite Africa having the highest daily incidence of IPV worldwide (McCloskey, 2013) and unique cultural and social characteristics (e.g., higher acceptance of IPV, traditional gender roles, and social acceptance of the husband’s right to use violence; Maguele et al., 2020; Perrin et al., 2019), no systematic review of the cycles of IPV in Africa has been conducted yet. Moreover, few prior reviews on the topic have explored both victimization and perpetration in males and females. Often, males are not portrayed in the literature on victimization, and females are rarely represented in the literature on perpetration (Stemple et al., 2017; Taylor et al., 2022). To help practitioners and researchers develop avenues for targeted IPV prevention and intervention in Africa, a comprehensive review of this literature and a meta-analysis of empirical studies is needed. Furthermore, a critical appraisal of the methodological qualities of existing studies will serve to guide future research endeavors.
The Current Study
The objectives of this review are to: (a) qualitatively and quantitatively synthesize the existing literature on the associations between exposure to IPV in childhood and experiences of IPV victimization/perpetration in adulthood in Africa; and (b) systematically assess the methodological quality of available studies. Moderating variables likely to increase or decrease the strength of the association between childhood exposure to IPV and experience of IPV in adulthood will be examined. Results from this review will provide a deeper understanding of cycles of IPV in Africa and help identify where research and intervention is needed in this region.
Method
Article Search and Selection
This review was pre-registered on PROSPERO (CRD42023472461). The literature search took place on April 12, 2023 and was updated in June 4, 2024. To ensure comprehensiveness, we used three search strategies: database searches, manual searches of reference lists of relevant articles, and machine learning tools.
Database Search
The review followed the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009), and the following databases were searched: (1) MEDLINE (Ovid; 1946-present); (2) PsycINFO (Ovid; 1806-present); (3) Scopus; and (4) Web of Science Core Collection. Keywords and search terms were defined with the guidance of a librarian. The initial search was peer-reviewed by an expert in the field of family violence. After amending the protocol and search terms based on peer-review recommendations, the final search strategy was applied to all the databases. The search combined terms related to IPV (e.g., exposure to violence, domestic violence, marital conflict, and interparental violence) with terms related to Africa/African countries, and cycles of abuse (e.g., revictimization, intergenerational relationships, intergenerational discontinuity, and family relationships). See Supplemental Appendix A for MEDLINE search. Finally, papers were identified through the list of references of relevant articles, systematic reviews, and meta-analyses.
Machine Learning Approach
To find similar and relevant articles, we used three publicly available software programs that apply machine learning for title and abstract screening (e.g., Connected Papers, Elicit, and ResearchRabbit). This search generated a total of 100 additional papers that were screened.
Inclusion and Exclusion Criteria
Quantitative and qualitative papers published in English and French were included if they were: (a) published in peer-reviewed journals; (b) included a sample of adult humans; (c) measured both the childhood exposure to IPV and experiences of IPV victimization/perpetration in adulthood; (d) involved participants living in Africa; and (e) qualitatively (for qualitative studies) or quantitatively (for quantitative studies) examined the association between childhood exposure to IPV and experiences of IPV victimization/perpetration in adulthood.
It was decided not to include the gray literature such as theses, working papers, newsletters, and government documents. Studies were excluded if they did not provide original empirical data (e.g., books and book chapters, presentations, literature reviews, and meta-analyses).
Data Screening and Eligibility
After removal of the duplicates in EndNote (version 20.3, Clarivate, Philadelphia, USA), all abstracts were imported into the Rayyan software (Ouzzani et al., 2016). Titles and abstracts were screened independently by the first (D.W.) and second (T.P.) authors. The level of agreement between the two independent screeners was 85% for titles and abstracts screening, data extraction, and the quality assessment. When disagreements occurred, they were discussed based on the predetermined inclusion and exclusion criteria, and by discussion with the third team member (R.L.).
Data Extraction
One researcher (D.W.) extracted the data, and another researcher (T.P.) cross-checked it for accuracy. The data extracted included authors, country, study aims, type of adult IPV experience, study design, participants, measures, and relevant findings.
Quality Assessment
Two researchers (D.W. and T.P.) performed the quality assessment for each article independently and then compared their ratings. Any disagreements were resolved through discussion. All included studies were quantitative and were, therefore, assessed using the Appraisal tool for Cross-Sectional Studies (AXIS) (Downes et al., 2016), which is a 20-item tool documenting risk of bias in all components of the manuscript (i.e., research questions, methods, design, results/analyses, and discussion). The raters were asked to indicate whether each of the quality indicators was present (i.e., “yes” or “no”) in the included study, with a higher number of “yes” indicative of higher study quality. We applied the scoring method used in previous systematic reviews and meta-analyses: yes or not applicable (N/A) = 1 point, no or do not know = 0 point (Moor & Anderson, 2019; Oliver et al., 2023). The quality of each study was given a score out of 20. Studies were rated as Good (15), Fair (10–14), or Poor (<10).
Quantitative Synthesis
A meta-analysis was conducted with Comprehensive Meta-analysis 4.0, Englewood, NJ (Borenstein et al., 2022) for Objective 1. The effect size index was the odds ratio, and the random-effects model was used for the analysis since the included studies were treated as random samples (Borenstein et al., 2010). The quantitative synthesis was presented according to IPV (all types combined) and IPV subtypes and was performed if we found at least two studies (Valentine et al., 2010). In addition, subgroup meta-analyses were calculated to test for moderating variables (i.e., type of IPV experience, countries, gender, and quality rating) using mixed effects model. Forest plots were created to present the data, and 95% confidence intervals (CIs) were calculated around the pooled estimates. Multiple tests, including Q, I2, and Tau statistics, were used to examine heterogeneity (Borenstein, 2019), and sensitivity analyses were carried out to examine the contribution of each study. To detect publication biases, we carried out three tests: Egger’s test (Egger et al., 1997), the rank correlation test (Begg & Mazumdar, 1994), and the fail-safe N (Rosenthal, 1979).
Results
Our database search generated 8,262 papers in total. The manual search from the reference lists of previous articles resulted in 10 more papers. The machine learning approach resulted in 100 additional papers to screen. After removing the duplicates, we were left with 6,001 papers. After abstract and title screening, 397 papers remained for full-text review. Full-text screening resulted in the exclusion of 349 additional papers that were: not looking at IPV both in childhood and adulthood (n = 290); theses (n = 5); reviews (n = 20); chapters with no original data (n = 2); studies not carried out in Africa (n = 9); not including data relevant to the review’s objectives (n = 22); and did not allow for the specific examination of IPV due to the combination with other traumatic events (n = 1). A final sample of 48 original studies was included in the systematic review. For the meta-analysis, 39 studies were included. When several studies used the same sample, the article with the most comprehensive results was used for the meta-analysis. After contacting the authors, papers missing the necessary information to calculate an effect size were excluded. Figure 1 illustrates the selection process.
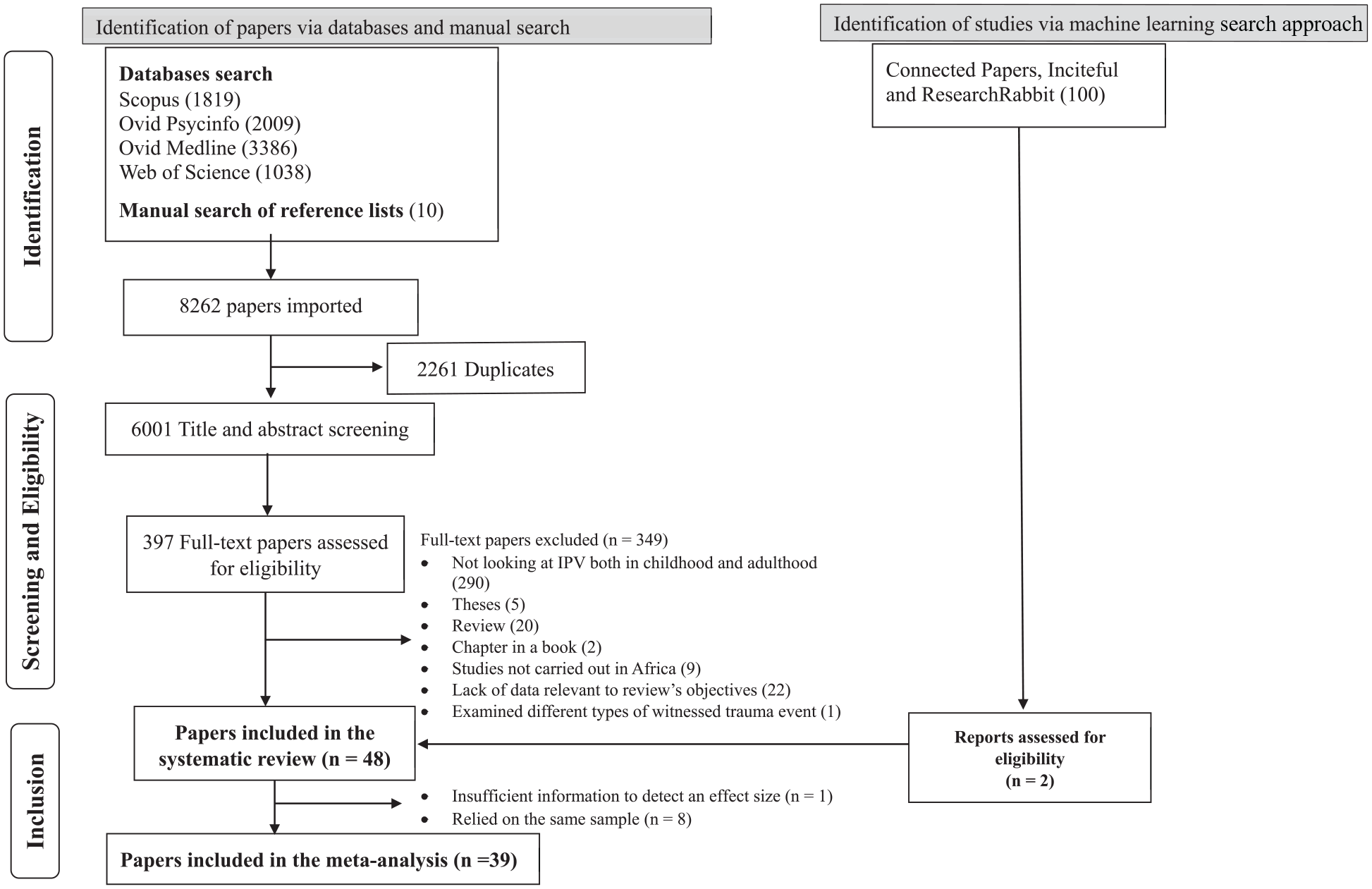
PRISMA flowchart of study selection and review process.
Descriptive Summary of the Included Papers
Sample sizes ranged from 834 to 97,542 participants for a total sample of N = 520,000 (Table 1). They described experiences of IPV in 29 African countries: nine in Nigeria; seven in Ethiopia, seven in South Africa; six in Uganda; six in Kenya; five in Ghana; four in Mali; four in Sierra Leone; four in Gambia; three in the Democratic Republic of Congo; three in Rwanda; three in Zambia; three in Tanzania; three in Angola; three in Zimbabwe; three in Liberia; three in Namibia; two in Cameroon; two in the Ivory Coast; two in Togo; two in Malawi; two in Benin; one in Egypt; one in Burundi; one in Gabon; one in Comoros; one in Burkina Faso; one in Chad; and one in Mozambique. The earliest study to examine cycles of IPV was published in 2002 (Jewkes et al., 2002); 60% (29/48) of included articles were published between 2020 and 2024. For all the studies, childhood exposure to IPV focused on father-to-mother violence. Included papers were all quantitative, cross-sectional, and, for the most part, population-based. Most studies examined IPV subtypes in adulthood, including physical, emotional, and sexual violence, and how each subtype may be associated with childhood exposure to IPV. To measure IPV, most studies (28/48; 58%) used the Domestic Violence Module Questionnaire of the Demographic and Health Survey (DHS), which is a modified version of the Revised Conflict Tactics Scale (Yount et al., 2022). Other validated instruments included the Abuse Assessment Screen/Partner Violence Screen, and the World Health Organization (WHO) instruments (e.g., WHO violence against female instruments, WHO multi-country study questionnaires, WHO multi-country study on female’s health and life, World mental health survey questionnaire).
Descriptive Summary of Studies Investigating Cycles of IPV.
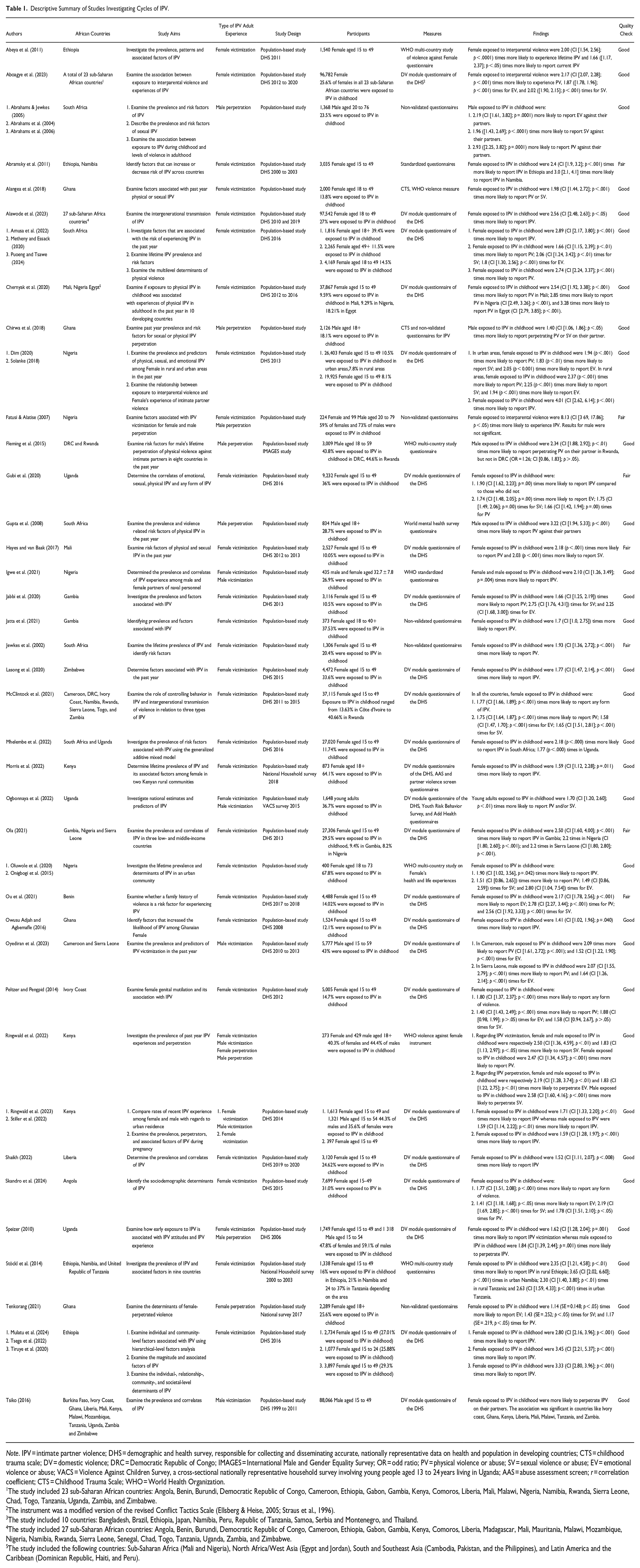
Note. IPV = intimate partner violence; DHS = demographic and health survey, responsible for collecting and disseminating accurate, nationally representative data on health and population in developing countries; CTS = childhood trauma scale; DV = domestic violence; DRC = Democratic Republic of Congo; IMAGES = International Male and Gender Equality Survey; OR = odd ratio; PV = physical violence or abuse; SV = sexual violence or abuse; EV = emotional violence or abuse; VACS = Violence Against Children Survey, a cross-sectional nationally representative household survey involving young people aged 13 to 24 years living in Uganda; AAS = abuse assessment screen; r = correlation coefficient; CTS = Childhood Trauma Scale; WHO = World Health Organization.
The study included 23 sub-Saharan African countries: Angola, Benin, Burundi, Democratic Republic of Congo, Cameroon, Ethiopia, Gabon, Gambia, Kenya, Comoros, Liberia, Mali, Malawi, Nigeria, Namibia, Rwanda, Sierra Leone, Chad, Togo, Tanzania, Uganda, Zambia, and Zimbabwe.
The instrument was a modified version of the revised Conflict Tactics Scale (Ellsberg & Heise, 2005; Straus et al., 1996).
The study included 10 countries: Bangladesh, Brazil, Ethiopia, Japan, Namibia, Peru, Republic of Tanzania, Samoa, Serbia and Montenegro, and Thailand.
The study included 27 sub-Saharan African countries: Angola, Benin, Burundi, Democratic Republic of Congo, Cameroon, Ethiopia, Gabon, Gambia, Kenya, Comoros, Liberia, Madagascar, Mali, Mauritania, Malawi, Mozambique, Nigeria, Namibia, Rwanda, Sierra Leone, Senegal, Chad, Togo, Tanzania, Uganda, Zambia, and Zimbabwe.
The study included the following countries: Sub-Saharan Africa (Mali and Nigeria), North Africa/West Asia (Egypt and Jordan), South and Southeast Asia (Cambodia, Pakistan, and the Philippines), and Latin America and the Caribbean (Dominican Republic, Haiti, and Peru).
Methodological Quality Assessment
Overall, most papers (41/48; 85%) were of high methodological quality. This may be due to the use of large national population-based datasets (e.g., DHS, household survey) for secondary analyses. With large samples that do not raise concerns about statistical power, these highly rated papers provided a clear provision for the target population, sampling frame, sample selection, sample size, and sample justification. In addition, the research questions, method of data collection, analyses and representation of the data, and interpretation of the results were aligned. Finally, some studies performed adjusted analyses and provided differences in baseline sociodemographic/other variables between groups that may influence the outcome. Still, seven studies (14%) were rated fairly (Abramsky et al., 2011; Fatusi & Alatise, 2007; Gubi et al., 2020; Hayes & van Baak, 2017; Jewkes et al., 2002; Ola, 2021; Ou et al., 2021). In many cases, there was no clear justification of the sample size nor a power analysis. Furthermore, the statistical significance and the statistical methods were not sufficiently described to enable replication.
Meta-Analysis Synthesis
We included 39 studies in the meta-analysis; however, with regards to countries (when more than one was included in a given study) and gender, studies were entered separately in the meta-analysis. Figure 2 shows the forest plot presenting the effect sizes for each sample and the total effect using the random effects model. Overall, pooled effects indicated a significant association between childhood exposure to IPV and experiences of IPV in adulthood (OR = 2.24, 95% CI [1.91, 2.64]; p < .001). Sensitivity analyses showed that by removing one study at a time, the effect size did not change (OR = 2.29, 95% CI [1.94, 2.70]; p < .001), indicating the robustness of our effect size. Respondents who were exposed to IPV in childhood were more than twice as likely to be involved in IPV in adulthood. The true effect size was not the same in all the studies (Q-value = 1015.32, df = 33, p < .001). The I-squared statistic showed that 97% of the variance in observed effects reflect variance in true effects rather than sampling error (I2 = 97%). The variance of true effect sizes (T2) was 0.19 in log units, while the standard deviation of the true effect sizes (T) was estimated at 0.44 in log units with a prediction interval of 0.89–5.66.
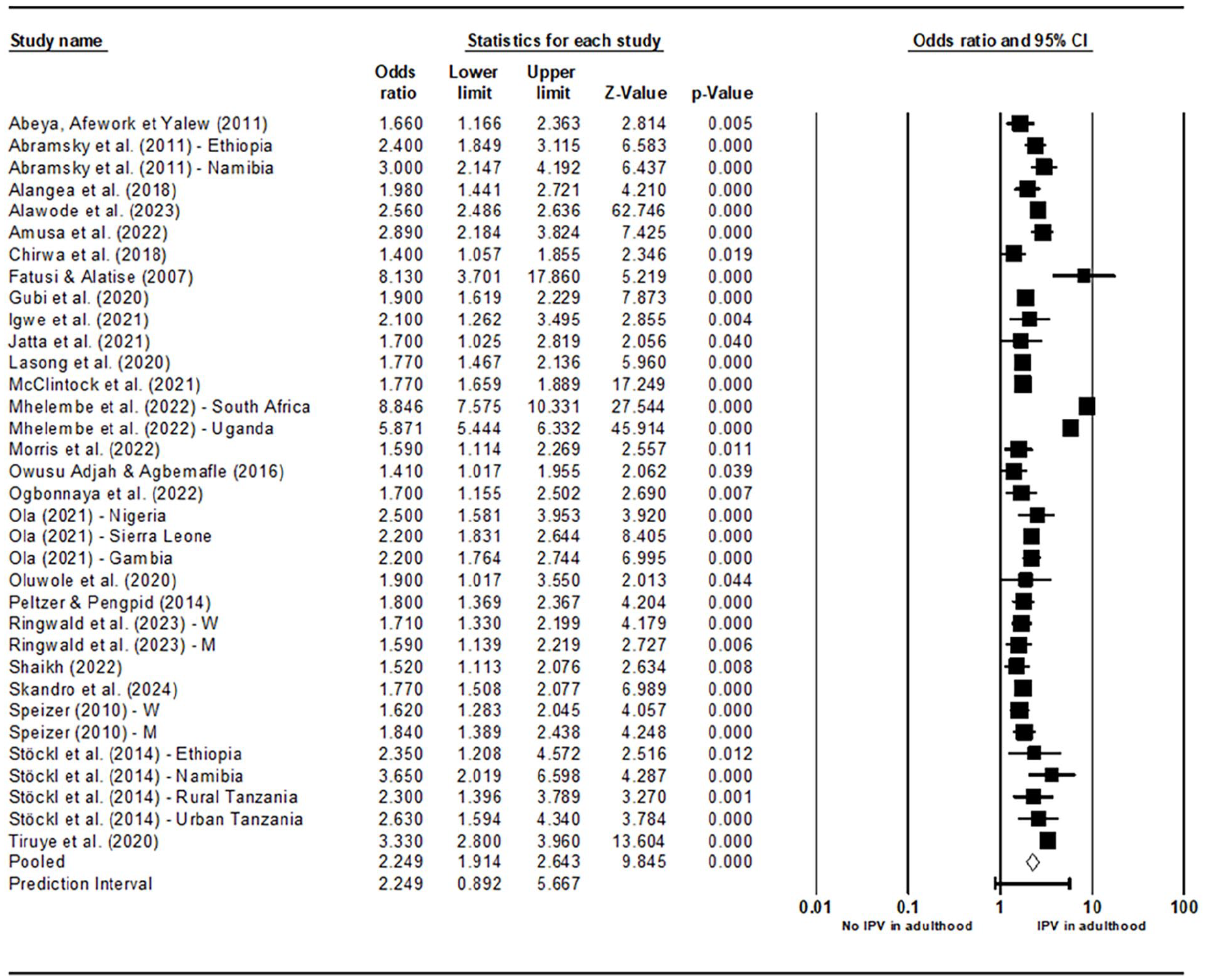
Forest plot showing effect size of studies on IPV experience in adulthood.
When looking at different types of IPV, it was found that respondents who were exposed to IPV in childhood were 2.24 times (95% CI [1.50, 3.35], p < .001; Q-value = 7920.71, df = 26, p < .001, I2 = 100%) more likely to be involved in physical violence in adulthood, 2.39 times (95% CI [1.47, 3.87, p < .001; Q-value = 3735.18, df = 17, p < .001, I2 = 100%) more likely to be involved in sexual violence in adulthood, and 1.91 times (95% CI [1.57, 2.31, p < .000; Q-value = 343.88, df = 18, p < .001, I2 = 95%) more likely to be involved in emotional violence in adulthood. See Supplemental Appendix B for the forest plots of IPV subtypes meta-analyses (Supplemental Figures S1–S3).
To assess the risk of bias between studies on IPV, the funnel plot of the overall effect was visually inspected (see Figure 3). A general asymmetry between studies was observed. Regression for funnel plot asymmetric (Egger's intercept = −1.09, 95% CI [−3.64, 1.45], p = .19) and the rank correlation test (p = .02) suggested that publication bias was present. On the other hand, the fail-safe N analysis showed that 22,219 studies with null results would be needed for the cumulative effect to become statistically non-significant.
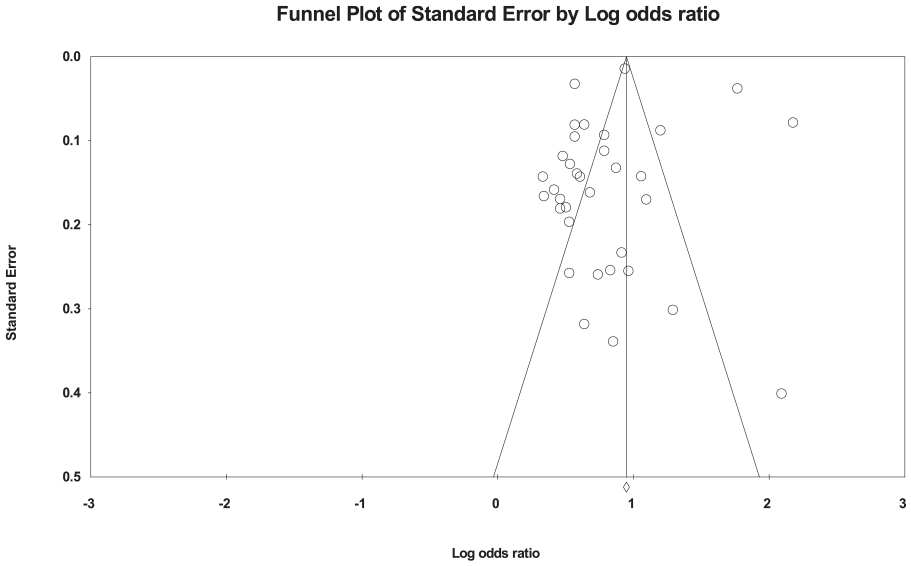
Funnel plot showing publication bias of studies on IPV experience in adulthood.
Childhood Exposure to IPV and IPV Victimization in Adulthood
Thirty-eight out of the 48 (79%) studies reported on the association between childhood exposure to IPV and female victimization in adulthood (Abeya et al., 2011; Aboagye et al., 2023; Abramsky et al., 2011; Alangea et al., 2018; Alawode et al., 2023; Amusa et al., 2022; Chernyak et al., 2020; Dim, 2020; Fatusi & Alatise, 2007; Gubi et al., 2020; Hayes & van Baak, 2017; Igwe et al., 2021; Jabbi et al., 2020; Jatta et al., 2021; Jewkes et al., 2002; Lasong et al., 2020; McClintock et al., 2021; Metheny & Essack, 2020; Mhelembe et al., 2022; Morris et al., 2022; Mulatu et al., 2024; Ogbonnaya et al., 2022; Ola, 2021; Oluwole et al., 2020; Onigbogi et al., 2015; Ou et al., 2021; Owusu Adjah & Agbemafle, 2016; Peltzer & Pengpid, 2014; Puoeng & Tsawe, 2024; Ringwald et al., 2022; Ringwald et al., 2023; Shaikh, 2022; Skandro et al., 2024; Solanke, 2018; Speizer, 2010; Stöckl et al., 2014; Tiruye et al., 2020; Tsega et al., 2022).
Very few papers (6/48; 12%) looked at male victimization (Igwe et al., 2021; Ogbonnaya et al., 2022; Oyediran et al., 2023; Ringwald et al., 2022; Ringwald et al., 2023; Tsiko, 2016). Most researchers carried out a secondary analysis of the data made available by the DHS. Remarkably, Tsiko (2016) provided a more holistic picture of male victimization in Africa, as the data he used were based on DHS data from 12 African countries: Burkina Faso, Ivory Coast, Ghana, Liberia, Mali, Kenya, Malawi, Mozambique, Tanzania, Uganda, Zambia, and Zimbabwe. It is also worth noting that one researcher examined a high-risk population of military personnel (Igwe et al., 2021).
Results indicated that between 8.1% and 67.8% of females and 22.01% of males who were exposed to IPV as children reported being victimized by their intimate partner as adults. The pooled estimates for IPV victimization for female (OR = 2.46, 95% CI [2.09, 2.91], p < .001) and for male (OR = 1.76, 95% CI [1.57, 1.97], p < .001) were statistically significant (see Supplemental Material). Males and females who were exposed to IPV in childhood were more likely to be victims of IPV in adulthood compared to those with no childhood exposure.
Childhood Exposure to IPV and IPV Perpetration in Adulthood
Nine studies (18%) reported male perpetration of IPV over the previous year (Abrahams & Jewkes, 2005; Abrahams et al., 2004; Abrahams et al., 2006; Chirwa et al., 2018; Fatusi & Alatise, 2007; Fleming et al., 2015; Gupta et al., 2008; Ringwald et al., 2023; Speizer, 2010), and two studies (4%) investigated female perpetration of IPV over the past year (Ringwald et al., 2022; Tenkorang, 2021) using, respectively, a community sample in Kenya and a nationally representative sample collected in Ghana.
Studies showed that 18.1% to 44.6% of males and 40.3% of females who were exposed to IPV as children perpetrated IPV in adulthood. Our results showed that exposure to IPV in childhood was associated with male perpetration of physical, sexual, and emotional IPV and female perpetration of emotional IPV in adulthood. The pooled estimates for IPV perpetration for male (OR = 1.92, 95% CI [1.60, 2.29], p < .001) and for female (OR = 3.04, 95% CI [2.51, 3.69], p < .001) were statistically significant, indicating that individuals who were exposed to IPV in childhood, compared to non-exposed individuals, regardless of gender, were almost twice as likely to be perpetrators of IPV in adulthood.
Moderator Analyses
Moderator analyses for gender revealed that there was a significant gender mean difference in the strength of the relationship between childhood exposure to IPV and experiences of IPV in adulthood (Q-value = 6.63, df = 1, p = .010). The effect size for female studies (OR = 2.35, 95% CI [1.85, 2.99]) was significantly higher than the effect size for male studies (OR = 1.60, [1.35, 1.89]). Results also showed that effect sizes varied when countries were used as a moderator (Q-value = 31.87, df = 13, p = .003), with countries such as Namibia and South Africa showing larger effect sizes (OR > 3.00) compared to other countries. Furthermore, the mixed effect moderation analysis for type of IPV experience was significant (Q-value = 3.89, df = 1, p = .048). However, the results for quality rating as a moderator was not significant (Q-value = 1.079, df = 1, p = .29).
Discussion
The aim of the present study was to quantitatively and qualitatively synthesize the existing literature on the association between exposure to IPV in childhood and experiences of IPV in adulthood in Africa. A total of 48 studies were included, with data concerning close to 520,000 males and females from 29 African countries. The most common experience of IPV in adulthood was female victimization (38/48; 79%) followed by male perpetration (9/48; 18%). However, few studies also examined male victimization (6/48; 12%) or female perpetration (2/48; 4%). Our results indicated that between 8.2% and 67.8% of females and 22.01% of males who were exposed to IPV in childhood reported being victimized by an intimate partner in adulthood. Furthermore, 18.1% to 44.6% of males and 40.3% of females who had been exposed to IPV as children, reported perpetrating IPV in an adult relationship. Overall, pooled effects indicated a strong significant association between childhood exposure to IPV and experiences of IPV in adulthood. Regardless of gender, individuals who were exposed to IPV in childhood were more likely to be involved as victims or perpetrators of IPV in adulthood. However, the effect size varied substantially across studies, suggesting that other risk factors should be considered in future studies. Table 2 provides a summary of the critical findings.
Summary of Critical Findings.
Note. IPV = intimate partner violence.
Association between Exposure to IPV in Childhood and Experiences of IPV in Adulthood
Our results show that the prevalence of childhood exposure to IPV ranges from 9.3% to 67.8%. This prevalence is much higher than the 8% to 25% reported by previous research from high-income countries (Gilbert et al., 2009). This discrepancy may be explained by the high levels of IPV in Africa, also documented in previous studies (McCloskey et al., 2016). The overall pooled effect size indicated that males and females who reported childhood exposure to IPV were more likely to be a victim or perpetrator of IPV in adulthood. This finding is consistent with results documented in many IPV studies conducted in Western countries and strongly supports the existence of cycles of IPV (Puno et al., 2023; Roberts et al., 2010; Yan & Karatzias, 2020).
Gender Differences with Regard to IPV Experiences in Adulthood
Substantial differences between males and females regarding perpetration in adulthood were observed. Specifically, male were the perpetrators of physical, sexual, and emotional IPV, while female’s perpetration was only reported for emotional IPV. In line with earlier studies, this suggests that emotional IPV may be the most common form of IPV perpetrated by female (Harned, 2001; Karakurt & Silver, 2013).
Our results showed that females were, to a considerably higher extent, more likely than males to be victims of physical, sexual, and emotional IPV in adulthood. This is probably because most studies were carried out on abused females, in contrast to abused males. It may be that this disproportionate risk of IPV victimization between males and females is reflecting the gender power imbalance in most African countries, reinforced by cultural norms and society’s strong endorsement of traditional gender roles (Umubyeyi et al., 2014). Moreover, IPV experiences are deeply rooted in social and cultural values supporting violence against female (e.g., male dominance, the need to maintain family secrecy, woman perceived as the property of her husband, and rigid gender roles) (World Health Organization [WHO], 2009), and these values are more powerful in the African context compared to other world regions (WHO, 2013).
It is encouraging that some studies examined male victims and female perpetrators of IPV in Africa, where males are not traditionally positioned to be victims (Ayodele, 2017), and where admitting one’s victimization could lead to serious social stigmatization (Moore, 2021). As a result, IPV, once considered a crime perpetrated only by males against females, is increasingly recognized (and demonstrated by research) as also being perpetrated by females against males (Hine et al., 2022). Some researchers have even suggested that male now account for approximately 40% of IPV victims, and that the most common forms of violence are physical and emotional (Tsiko, 2016). In Western countries, reciprocal violence (i.e., being involved as both victims and perpetrators) is a predominant pattern of violence among couples (Costa et al., 2015). Male victimization and female perpetration in Africa may be explained by reactive violence in which females are defending themselves against violent male. Including more male victims and more countries in future research could give us a better understanding of the profiles and needs of abused males and may even lead to needed legislative and policy changes to recognize this form of violence.
Comparison between Countries
Some researchers suggested some cross-cultural differences in cycles of IPV across countries, although an in-depth exploration of these differences was not provided. Moderation analysis showed that countries such as Namibia, and South Africa had larger effect sizes compared to other countries. It is likely that people living in communities with more receptive norms and practices around violence (e.g., restrictive gender norms on female participation in decision making, laws and other local conditions that favor/disfavor gender inequity, restrictive community norms about female’s sexual rights) would experience higher prevalence of IPV (Mossie et al., 2023; Okenwa et al., 2009; Oyediran & Feyisetan, 2017). However, there may be some contextual and country-specific drivers of IPV, which would require further investigation.
Strength and Limitations
Included Papers
Some limitations of the included papers must be acknowledged. First, the available data focus exclusively on violence in heterosexual couples. Second, most studies only looked at sexual, physical, and emotional violence and did not examine other types of IPV such as coercive control and economic violence. Moreover, emotional abuse was relatively rare as a type of IPV in the papers that were reviewed. Third, some of the participants were exposed to both IPV and maltreatment (e.g., physical abuse, sexual abuse) in their childhood, so it is possible that other forms of childhood adversity than exposure to IPV may have contributed to the adulthood experiences of IPV. Fourth, studies were all cross-sectional, while the ideal design to study cycles of IPV is prospective longitudinal studies. Indeed, adult males and females were asked to retrospectively report on their experience of IPV during childhood which may have introduced recall bias. Finally, the measurement tools used to examine experiences of IPV in adulthood and IPV exposure in childhood lacked consistency. In fact, some studies used non-validated measures (e.g., a single question to assess it). In other papers, no details were provided on the instrument used to measure violence. Despite these limitations, however, some strengths of the included studies need to be noted. The quality appraisals of most studies were high, and most studies included very large nationally representative samples.
The Current Review
This is the first systematic review and meta-analysis examining the association between childhood exposure to IPV and later adult IPV experiences in African countries; it included a very large pooled sample of close to 520,000 participants. Another strength is that a rigorous search was carried out using multiple strategies such as database searches, manual searches, and machine learning tools. Data screening and eligibility as well as quality assessment was carried out by two independent reviewers. Despite these strengths, our search did not yield any qualitative or longitudinal studies. Our review did not include clinical samples of abused females or males recruited via residential facilities and shelters. Clinical samples may represent more severe levels of IPV and, therefore, show a stronger relationship, increasing the robustness of our results. Furthermore, the effect sizes varied considerably from one study to another, indicating heterogeneity between studies. This heterogeneity may impact the quality and certainty of the evidence, so caution should be taken when interpreting the results. Finally, we need to consider the potential impact of publication bias, which may have inflated the effect size despite the robust sensitivity of the meta-analysis.
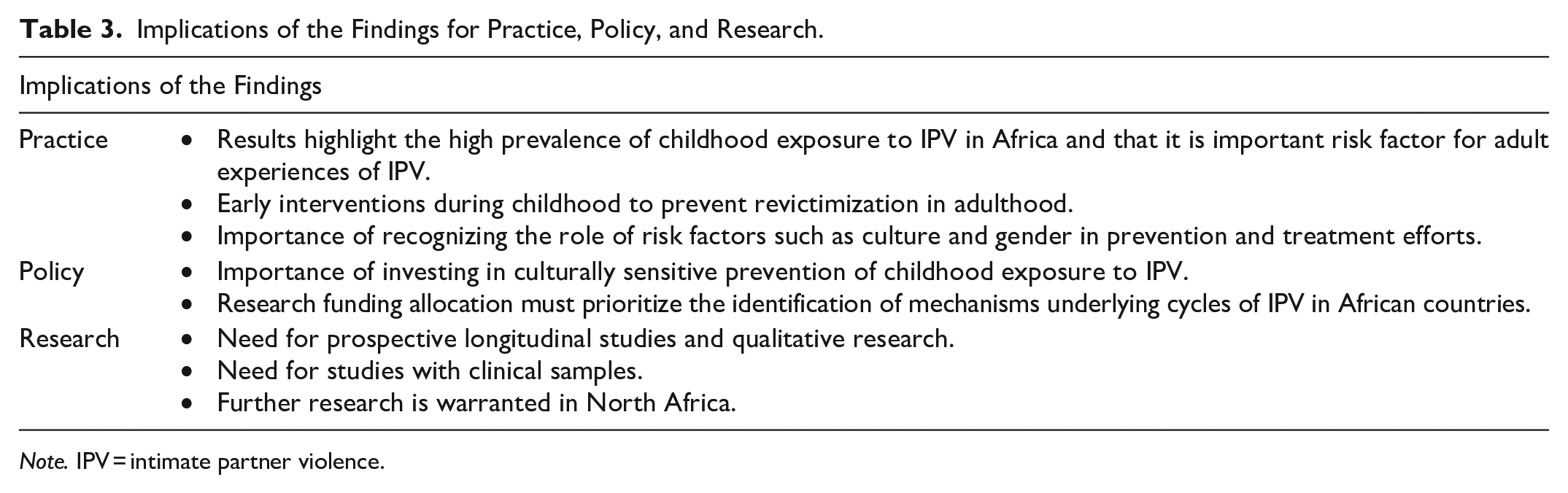
Implications of the Findings for Practice, Policy, and Research
A summary of core implications of the current review for practice, policy, and research is provided in Table 3. Findings suggest that childhood exposure to IPV is an important pathway that must be overcome to properly address intergenerational cycles of IPV. Hence, interventions during childhood may be necessary to prevent revictimization in adulthood. Public health policymakers should be aware of the importance of investing in primary prevention of IPV. In particular, the prevention of childhood exposure to IPV could be integrated in existing efforts to prevent IPV and should be integrated into existing public policy and community structures if they are to be successful. Cross-cultural differences were observed, so it may be essential to recognize the social determinants of IPV in prevention and treatment efforts. Given that culture can influence the magnitude of the association between childhood exposure to IPV and later IPV experiences, developing and evaluating culturally sensitive programs is essential. Additionally, given the high prevalence of IPV in African countries, identifying the individual and community mechanisms underlying IPV cycles is crucial for primary prevention and early intervention. Significant gaps in the literature were also apparent. The geographical distribution of studies indicated overrepresentation of sub-Saharan African regions and underrepresentation of North African countries. Very few studies collected data on other forms of IPV such as coercive control and economical violence. Prospective longitudinal studies and qualitative research are essential to support findings from the cross-sectional research previously discussed. One area for increased attention is the inclusion of more studies about male victims and female perpetrators of IPV. More importantly, cultural validation of IPV measures is needed to demonstrate that they are appropriate, accurate, and comprehensive and that they reflect the construct of IPV as experienced in this area. Finally, our review draws attention to the lack of evidence among clinical samples.
Implications of the Findings for Practice, Policy, and Research.
Note. IPV = intimate partner violence.
Conclusion
The review provides a unique insight into cycles of IPV from childhood to adulthood among males and females in Africa and shows clear evidence that exposure to IPV as a child is a strong risk factor for both perpetration and victimization of IPV in romantic relationships during adulthood. The results of this review fill an important gap in the literature and give rise to a number of implications for practice, policymaking, and research that may be considered.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241287144 – Supplemental material for A Systematic Review and Meta-Analysis of the Association between Childhood Exposure to Intimate Partner Violence and Intimate Partner Violence Victimization/Perpetration in Adulthood in Africa
Supplemental material, sj-docx-1-tva-10.1177_15248380241287144 for A Systematic Review and Meta-Analysis of the Association between Childhood Exposure to Intimate Partner Violence and Intimate Partner Violence Victimization/Perpetration in Adulthood in Africa by Dany Laure Wadji, Teresa Pirro and Rachel Langevin in Trauma, Violence, & Abuse
Footnotes
Acknowledgments and credits
Our gratitude goes to Michael Borenstein and Audrey Kern for their guidance in carrying out this meta-analysis. We thank Sharon Rankin and Andrea Quaiattini, McGill University Librarians, for her help in refining the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by an SNSF Postdoc. Mobility grant (#P500PS_214332) from the Swiss National Science Foundation awarded to the first author. The last author is supported by a salary award from the Fonds de recherche du Québec – Santé (#310809).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.