
Abstract
Background and Aims:
FreeStyle Libre® systems are effective and convenient glucose flash monitoring (FM) devices. This cost analysis compared FM versus self-monitoring of blood glucose (SMBG) in poorly controlled (glycated hemoglobin [HbA1c] >8%) patients with type 2 diabetes (T2D) on basal insulin in Spain.
Methods:
A model was used to compare the costs of FM and SMBG in a 1000-patient cohort. All model inputs were sourced from scientific literature and validated by a multidisciplinary experts’ group. Unitary costs were included in euros (2025), including value-added tax (VAT). The daily use of 2.5 strips (€0.57/strip) and 2.5 lancets (€0.14/lancet) was considered for SMBG according to Spanish recommendations. The events/person-year was 2.5 for severe hypoglycemic events (SHEs) (€1403.03/event), 17.02 for non-SHEs (NSHEs) (€3.92/event), and 0.0025 for diabetic ketoacidosis (DKA) (€2523.93/event). FM reduced the use of strips/lancets (−83.0%; sensor: €3.00/day) and acute events (NSHEs/SHEs: −58.0%; DKA: −68.0%). Sensitivity analyses were conducted to test robustness. Two additional scenarios were studied, including chronic diabetic complications (absolute reduction in HbA1c with FM: −1.1%) and absenteeism-related costs (reduction in absenteeism with FM: −58.4%).
Results:
The annual cost per patient was €3299.99 with SMBG and €2320.20 with FM. In 1000 patients, FM averted 2162 NSHEs (FM vs. SMBG: −€66,672), 1450 SHEs (FM vs. SMBG: −€2,579,224), and 1.5 DKA (FM vs. SMBG: −€6310), producing total cost savings of €979.706 compared with SMBG. All sensitivity analyses confirmed cost savings of FM versus SMBG, even when strips/lancets were free (−€442,117) or assuming a lower SHE frequency (1.4 events/patient-year; −€321,488). In 1000 patients, when considering chronic diabetic complications (SMBG: €3,745,869; FM: €2,886,785) and absenteeism (SMBG: €237,990; FM: €99,004), the annual cost savings of FM versus SMBG rose to €1,997,777.
Conclusions:
FreeStyle Libre could reduce acute events, chronic diabetic complications, and work absenteeism in poorly controlled patients with T2D on basal insulin, generating cost savings for the Spanish health system and society.
Keywords
Introduction
The prevalence of diabetes increased from 3.2% worldwide in 1990 to 6.1% in 2021, representing a growth of almost 90.5%. 1 The prevalence of this condition is expected to reach 9.8% by 2050, which means that 1.3 billion people will be living with diabetes in 2050. 1 In addition, diabetes ranks among the top 10 diseases contributing to years lived with disability worldwide 2 and is the leading cause of blindness, kidney and heart diseases, stroke, and lower limb amputation. 3
Among the population with diabetes, the World Health Organization estimated that more than 95% have type 2 diabetes (T2D). 3 In Spain, epidemiological data highlight the important challenge that T2D represents for the National Health System (NHS). As estimated by the Di@bet.es nationwide cross-sectional study, the prevalence of known T2D was 7.8%. 4 Moreover, the incidence of T2D reported by the Di@bet.es study was 11.6 cases/1000 person-years. 5 In addition to its epidemiological burden, the mean annual cost per patient with T2D in Spain, as estimated from 2022 to 2023, was €5171. Of this amount, €2228 was attributed to hospital admissions, whereas €1703 was allocated to treatments covering an average of nearly 10 different drugs to manage their disease. The remaining €1240 was associated with outpatient care and additional tests. 6
Unlike the treatment of type 1 diabetes (T1D), in which patients require regular insulin doses, the initial treatment for most patients with T2D involves lifestyle modifications and noninsulin pharmacological treatment. If glucose levels remain uncontrolled after combining several antihyperglycemic drugs, including glucagon-like peptide-1 (GLP-1) receptor agonists for people with obesity, insulin-based regimens should be considered. International guidelines usually recommend starting with basal insulin and, if necessary, progressing to more complex insulin regimens.7,8
Sustained hyperglycemia contributes to the development of major diabetic complications, including acute diabetic ketoacidosis (DKA). 9 However, the treatment of T2D, particularly in the case of insulin therapy, can lead to hypoglycemia,10,11 which represents an important cause of morbidity and mortality in people with diabetes and adversely affects quality of life. 12 In this context, relying only on glycated hemoglobin (HbA1c) is insufficient to ensure proper disease control. 13
International clinical practice guidelines recommend the use of continuous glucose monitoring (CGM) in patients receiving insulin-based treatments. 14 Self-monitoring of blood glucose (SMBG) results in low adherence due to pain and discomfort caused by frequent finger pricks and interference with daily activities. 15 Although CGM systems have been developed somewhat to address these constraints, 16 its reimbursement remains limited, and the use of SMBG continues to be the standard of care in many settings.
CGM systems are classified into real-time CGM and on-demand systems, also called glucose flash monitoring (FM) or intermittent scanned glucose monitoring. Among the FM systems, FreeStyle Libre (
In addition to the demonstrated efficacy and effectiveness, previous economic evaluations from the perspective of the Spanish NHS revealed that FreeStyle Libre could lead to potential cost savings for people with T1D 29 or T2D receiving MDI. 30 Thus, providing economic evidence for its use in patients with T2D on basal insulin is key for decision-making.
Epidemiological estimates indicate that 81.6% of Spanish patients with T2D receive pharmacological treatment. 31 Insulin-based therapies are used in almost 21.3% of these patients, 31 approximately 61.8% of whom are receiving basal insulin regimens. 32 Among all Patients with T2D receiving basal insulin, poorly controlled patients remain a priority subgroup due to their susceptibility to worse clinical outcomes than adequately controlled patients. 18 It is estimated that 3.9% of patients present HbA1c levels over 10%, which increase to 4.5% and 18.9% for 9% and 8% cutoff values, respectively. 33 Thus, people on basal insulin with poorly controlled T2D in Spain represent a potential priority subgroup to benefit from a CGM system.
This study aimed to perform a cost analysis of the FreeStyle Libre systems compared with SMBG in Spain, focusing on adults with T2D on basal insulin therapy and poor glycemic control, defined as an HbA1c over 8%.
Materials and Methods
In line with those previous analyses conducted in Spain,29,30 a decision analytic model was developed in Microsoft Excel®, which estimated the clinical and economic impact associated with the FreeStyle Libre system compared with the SMBG. The model simulated two hypothetical cohorts comprising 1000 adults with poorly controlled T2D who received basal insulin therapy exclusively. The model estimated the occurrence of clinical events and the associated costs for the cohort using SMBG. The events and costs were subsequently compared with those estimated for the cohort using the FreeStyle Libre systems. In the base case, the model accounted for acute events, including hypoglycemic episodes and DKA events, over a 1-year time horizon.
The model inputs were validated by a multidisciplinary board of eight clinicians specializing in Endocrinology, Nutrition, Internal Medicine, and Primary Care, as well as Health Economists experienced in the economic evaluation of health care interventions. A literature review was conducted to collect the available evidence concerning the inputs of the model. All of these data were included in a structured questionnaire, which was completed individually by each clinician in the multidisciplinary group. Their answers were shared during a face-to-face meeting to validate and agree upon the most representative sources and values for all the inputs on the basis of clinical practice in Spain (Table 1).
Summary of Model Inputs
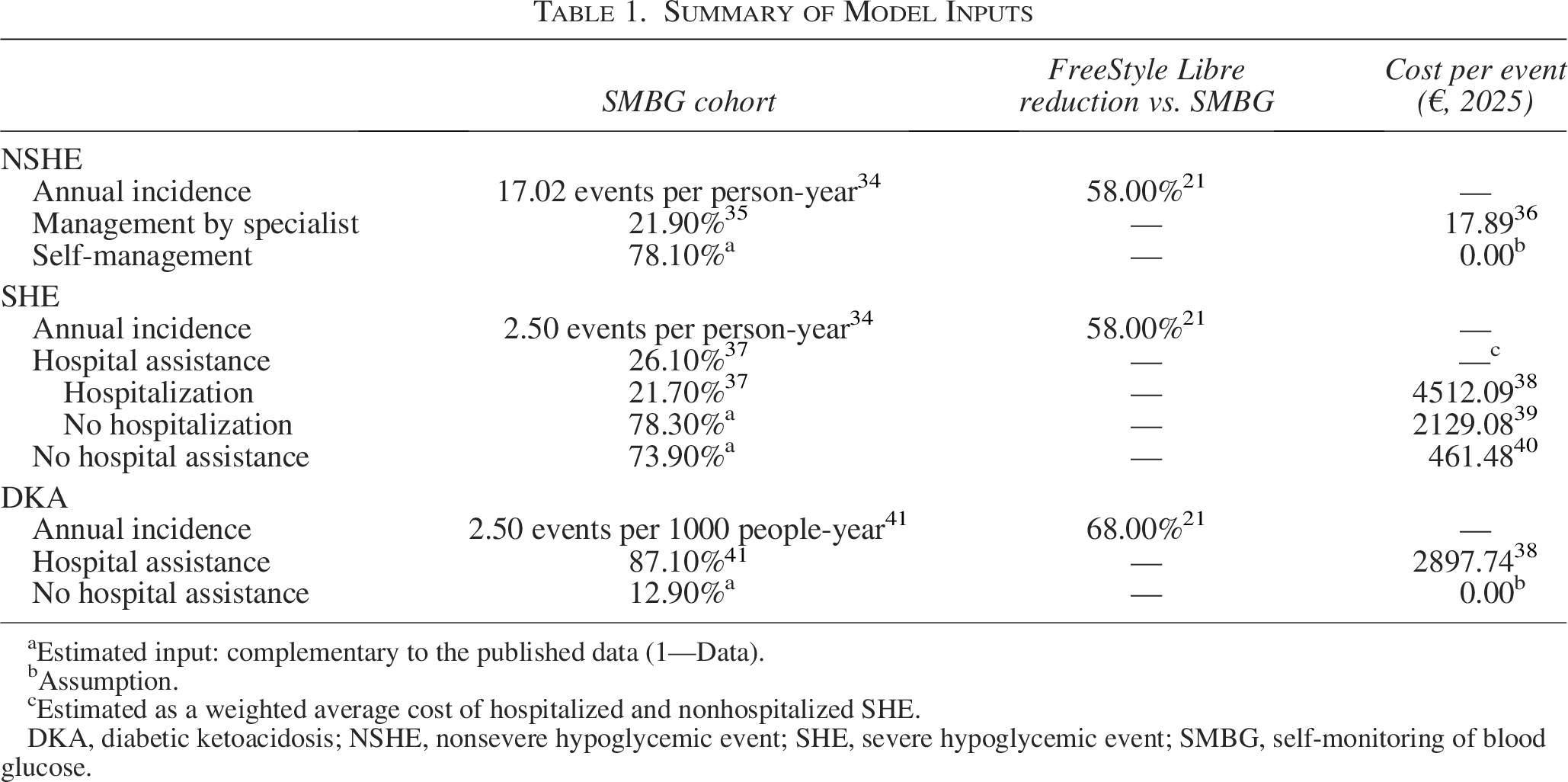
aEstimated input: complementary to the published data (1—Data).
bAssumption.
cEstimated as a weighted average cost of hospitalized and nonhospitalized SHE.
DKA, diabetic ketoacidosis; NSHE, nonsevere hypoglycemic event; SHE, severe hypoglycemic event; SMBG, self-monitoring of blood glucose.
The model and the results of this analysis were reported following the International Society for Pharmacoeconomics & Outcomes Research Consolidated Health Economic Evaluation Reporting Standards checklist published in 2022 (Supplementary Table S1). 42
Study population
The target population consisted of poorly controlled adults with T2D on treatment with basal insulin in Spain, excluding those also treated with rapid-acting insulin. Clinicians were asked to agree on an HbA1c threshold to distinguish between adequate and poor glycemic control. Although some of the experts considered that an HbA1c level of 7.5% should prompt a therapeutic intervention, the final cutoff for this analysis was set at 8% based on available epidemiological evidence. Thus, patients with HbA1c levels greater than 8% (HbA1c >8%) were considered poorly controlled in this study.
Clinical inputs
The clinical events considered in the base case included acute events as follows: nonsevere hypoglycemic events (NSHEs), severe hypoglycemic events (SHEs), and DKA.
The occurrence of NSHEs in the SMBG cohort was derived from the Hypoglycemia Assessment Tool (HAT) multicentric study, which included 24 countries and enrolled 27,585 patients worldwide. The data used in the model (17.02 events/person-year) referred to the subgroup of adults with T2D receiving insulin therapy (N = 19,563 patients). 34 With respect to SHEs, the occurrence informed from the HAT study (2.5 events/person-year) was also selected for the base case analysis. 34 Although Spain did not participate in the HAT study, given the large sample size and robust study design, clinicians considered it the most representative source for real-world clinical practice.
Data on the occurrence of DKA in SMBG users were obtained from a retrospective study conducted in Andalusia, a region with 8.5 million inhabitants in Spain. 41 Hyperglycemic episodes were reported for 2484 patients using the International Classification of Diseases (ICD) codes for DKA (ICD-9: 250.1) and hyperosmolar hyperglycemic state (ICD-9: 250.2). For this analysis, only the occurrence of DKA was considered (2.5 events/1000 people-year). 41
In the case of the cohort potentially using FreeStyle Libre, reductions in the incidence of these acute events were estimated based on data from the RELIEF study, 21 a retrospective real-world evidence (RWE) study. 21 This study included data collected from French databases concerning 5933 adults with T2D on basal insulin monitored by FreeStyle Libre, who were previously using SMBG. The reductions in hypoglycemic events (−58.0%) and DKA (−68.0%) were obtained 12 months after starting FM. 21
Health care resource consumption and costs
The Spanish NHS perspective was considered to estimate the total costs associated with direct health care resources use for glucose monitoring (glucose sensors and/or glucose strips and lancets) and the management of acute events.
The health care resources dedicated to SMBG consisted of daily usage of 2.5 strips and 2.5 lancets per poorly controlled patient, according to the Spanish Diabetes Society (SED [Sociedad Española de Diabetes]) published guidelines. 43 A reduction of 83% in the use of strips and lancets was applied in the FreeStyle Libre cohort, based on evidence from the RELIEF study. 21 Otherwise, the annual usage of the FreeStyle Libre sensors per patient was considered for this analysis. The unitary costs of strips and lancets were obtained from the latest published economic evaluation of FM devices conducted by a regional Health Technology Assessment (HTA) Agency in Spain (€0.57 and €0.14, respectively). 44 The cost associated with the use of the FreeStyle Libre system was €3.00/day.
To estimate the cost associated with the management of acute events, these were further classified according to whether they are self-managed, required contact with specialists, hospital assistance, or even hospital admission,35,37,41 to account for both specific health resource consumption and associated costs per event.36,38–40
For NSHEs, data from a Spanish study, including 630 patients with T1D and T2D aged under 15 years, indicated that 21.9% of NSHEs in T2D required specialist care. 35 The selected source for characterizing SHEs consisted of a cross-sectional survey conducted in 8 countries (including Spain), which enrolled 184 participants with T2D. According to the T2D subgroup-specific data, 26.1% of SHEs required hospital assistance, of whom 21.7% were hospitalized. 37
Regarding the management of DKA, the previously described study conducted in Andalusia (Spain) reported that 87.1% of DKA events required hospital assistance. 41
The costs associated with self-, specialist-, or hospital-managed acute events were obtained from published studies. Although other sources of costs were evaluated by the multidisciplinary panel, given that the previously published cost analysis of FreeStyle Libre included the costs of interest, 30 these sources were selected because they are still considered an accurate reflection of clinical practice.36,38–40
All costs were considered in euros (€) and updated to 2025 according to variations in the consumer price index. The value-added tax (VAT) was included where applicable, following national recommendations for developing economic evaluations. 45 No discount rate was applied given the short time horizon.
Sensitivity analyses
One-way sensitivity analyses (OWSAs) were conducted to test the robustness of the model. First, all the parameters included in the model were varied by applying a ±20% variation to the base case value.
The subsequent OWSA included variations in potential key parameters as informed by the advisory board. First, the advisory board noted that the HAT study-reported rate of SHEs (2.5 events/person-year) 34 might overestimate the occurrence of SHEs in the target population of this analysis. An alternative rate of SHEs of 1.4 events/person-year 46 was considered in this OWSA. This rate was sourced from a prospective study conducted in Greece, which included 817 patients with T2D. 46
Although the RELIEF study was considered the most representative source of FreeStyle Libre effectiveness in clinical practice, alternative data sources for hypoglycemia and DKA reduction were also considered. One OWSA included a reduction in hypoglycemia associated with the use of FreeStyle Libre of 29.0%, 20 which was derived from a RWE study conducted in the United States, in which the clinical records of 2463 patients using FreeStyle Libre were analyzed. 20 Moreover, another OWSA included an alternative reduction in DKA associated with the use of FreeStyle Libre of 52.1%, 32 which also proceeded from the RELIEF study; however, in this case, all patients with T2D were pulled, 32 rather than exclusively those receiving basal insulin therapy.
Finally, in the last OWSA, the unit cost of strips and lancets was assumed to be €0.00.
Alternative scenarios
In addition to the base case, two alternative scenarios were proposed. The first alternative scenario included diabetic complications (Table 2), which were modeled by applying the occurrence of acute myocardial infarction, angina pectoris, heart failure, stroke, transitory cerebral ischemia, diabetic neuropathy, retinopathy, peripheral arterial disease, nephropathy, and end-stage renal disease. 47 The model estimated the reduction in the occurrence of these chronic complications based on HbA1c reduction associated with FreeStyle Libre use and the overall reduction in the risk of these comorbidities per 1% decrease in HbA1c levels. The HbA1c reduction associated with the FreeStyle Libre system was obtained from a retrospective RWE study conducted in the United States and Canada, including data from the clinical histories of 191 patients on basal insulin regimen. This study reported an annual HbA1c reduction of 1.1%. 57 On the basis of the clinicians’ opinions, this reduction was deemed representative of patients with T2D on basal insulin with a baseline HbA1c >8%. The risk reduction estimates for diabetic complications per 1% decrease in HbA1c levels were obtained from several studies in the T2D population with broad scientific support, such as the United Kingdom Prospective Diabetes Study 48 and Wisconsin Epidemiologic Study of Diabetic Retinopathy, 56 studies including large samples 49 and meta-analyses. 55 The annual costs associated with the management of chronic complications were obtained from sources considered in previously published economic evaluations conducted by a regional HTA Agency 44 in Spain.50–52,54 For those complications not included in this report, the Minimum Basic Data Set (Conjunto Mínimo Básico de Datos) costs published by the Spanish Ministry of Health 53 were used.
Occurrence, Risk Reduction per 1% Decrease in Glycated Hemoglobin A1c, and Costs Associated with Chronic Diabetic Complications
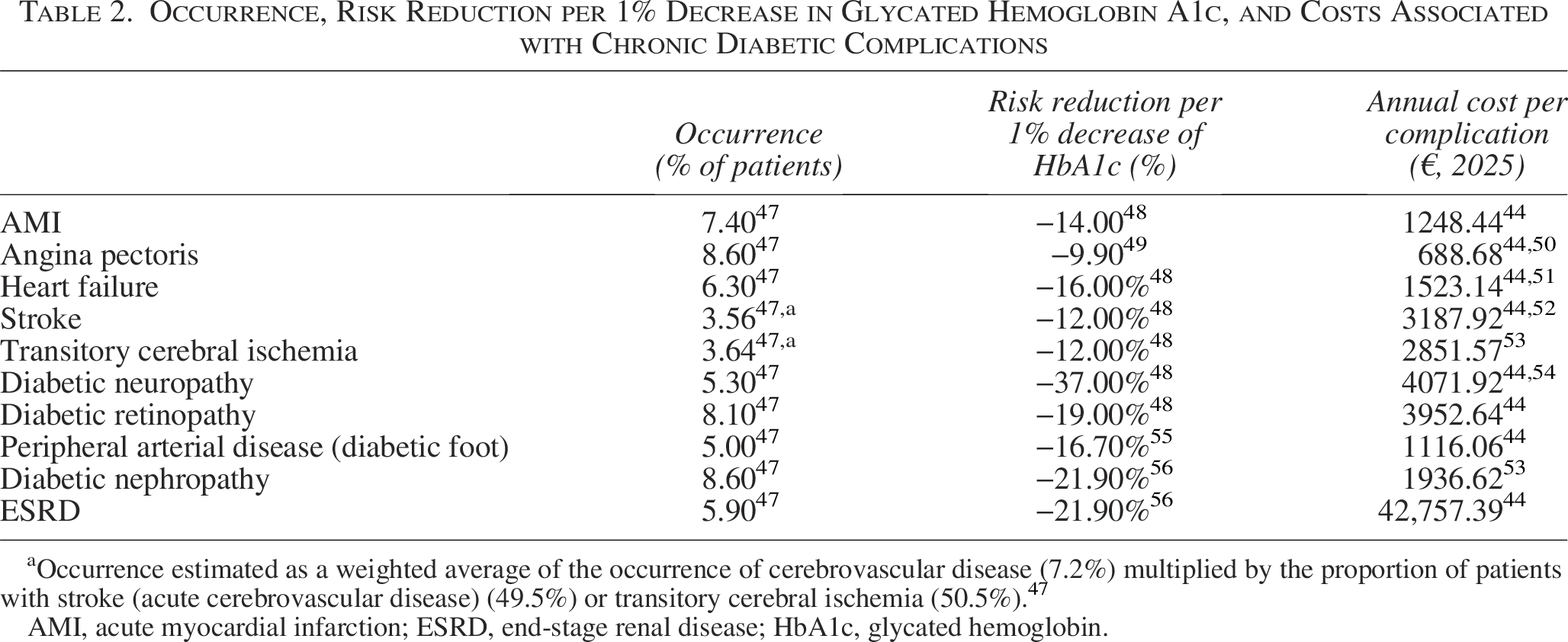
aOccurrence estimated as a weighted average of the occurrence of cerebrovascular disease (7.2%) multiplied by the proportion of patients with stroke (acute cerebrovascular disease) (49.5%) or transitory cerebral ischemia (50.5%). 47
AMI, acute myocardial infarction; ESRD, end-stage renal disease; HbA1c, glycated hemoglobin.
In line with national recommendations for economic evaluations, 45 a second alternative scenario provided economic evidence of FreeStyle Libre in patients with T2D on basal insulin from a societal perspective. Thus, in addition to acute and chronic diabetic complications, the costs associated with patients’ absenteeism were considered. In this analysis, the proportion of patients with T2D actively working, described in a Spanish study, was applied (26.5%). 35 In addition, a study showing the reduction in absenteeism associated with the use of FreeStyle Libre was selected to provide the absenteeism rate in patients with T2D (18.5%), 58 the mean number of absence days per patient (64.6 days), 58 and the decrease in absenteeism associated with the use of the sensor. 58 This study revealed that, over 12 months after switching from SMBG to FM with FreeStyle Libre, the absenteeism rate decreased from 18.5% to 7.7%, corresponding to a reduction of 58.4%. 58 The mean annual earnings per person, published by the Spanish National Statistics Institute, were used to estimate the costs associated with work absenteeism (27,447.21€/year). 59
Results
Base case results
The estimated total costs per patient with T2D on basal insulin and poor glycemic control (HbA1c >8%) were €3299.99 in the SMBG cohort and €2320.20 in the FreeStyle Libre cohort.
Glucose monitoring resource consumption yielded a cost per patient on SMBG of €647.70 and €1206.90 per patient receiving FreeStyle Libre. Compared with SMBG, the use of FreeStyle Libre would increase the cost by €559.20 (+86.3%), mainly because of the acquisition of the sensors, estimated at €1096.79 per patient-year. However, among the FreeStyle Libre users, the annual cost derived from the lower consumption of strips and lancets decreased from €630.06 to €110.11 per patient.
Regarding hypoglycemia episodes, the cost associated with the management of NSHEs was €66.67 per patient on SMBG and €28.00 per patient on FreeStyle Libre. These costs were caused exclusively by the episodes that required a specialist.
The cost of SHEs per patient in the SMBG cohort was €2579.22. The episodes not requiring hospital assistance produced a cost of €852.58. For those SHEs requiring hospital assistance, the cost per patient rose to €1087.76 and €638.88 in the case of patient admission or not, respectively. In the cohort receiving FreeStyle Libre, SHEs resulted in a cost of €1083.27 per patient, of which €358.09 derived from the episodes not requiring hospital assistance, €456.86 from SHEs requiring hospital admission, and €268.33 from those in which hospital care was provided without admission.
Overall, the annual cost per patient associated with both NSHEs and SHEs was €2645.90 per patient on SMBG and €1111.28 per patient on FreeStyle Libre, leading to savings of €1534.62/patient-year (−58.0%).
In relation to DKA, the cost per patient on SMBG was €6.31, which, compared with the cost of €2.02 per patient with FreeStyle Libre, resulted in savings of €4.29 (−68.0%). The total cost was derived from the specialist-managed episodes.
In summary, the use of FreeStyle Libre, compared with SMBG, would lead to annual savings of €979.71 per patient with T2D on basal insulin and poor glycemic control (−29.7%). A visual summary of the model results is presented in Figure 1.
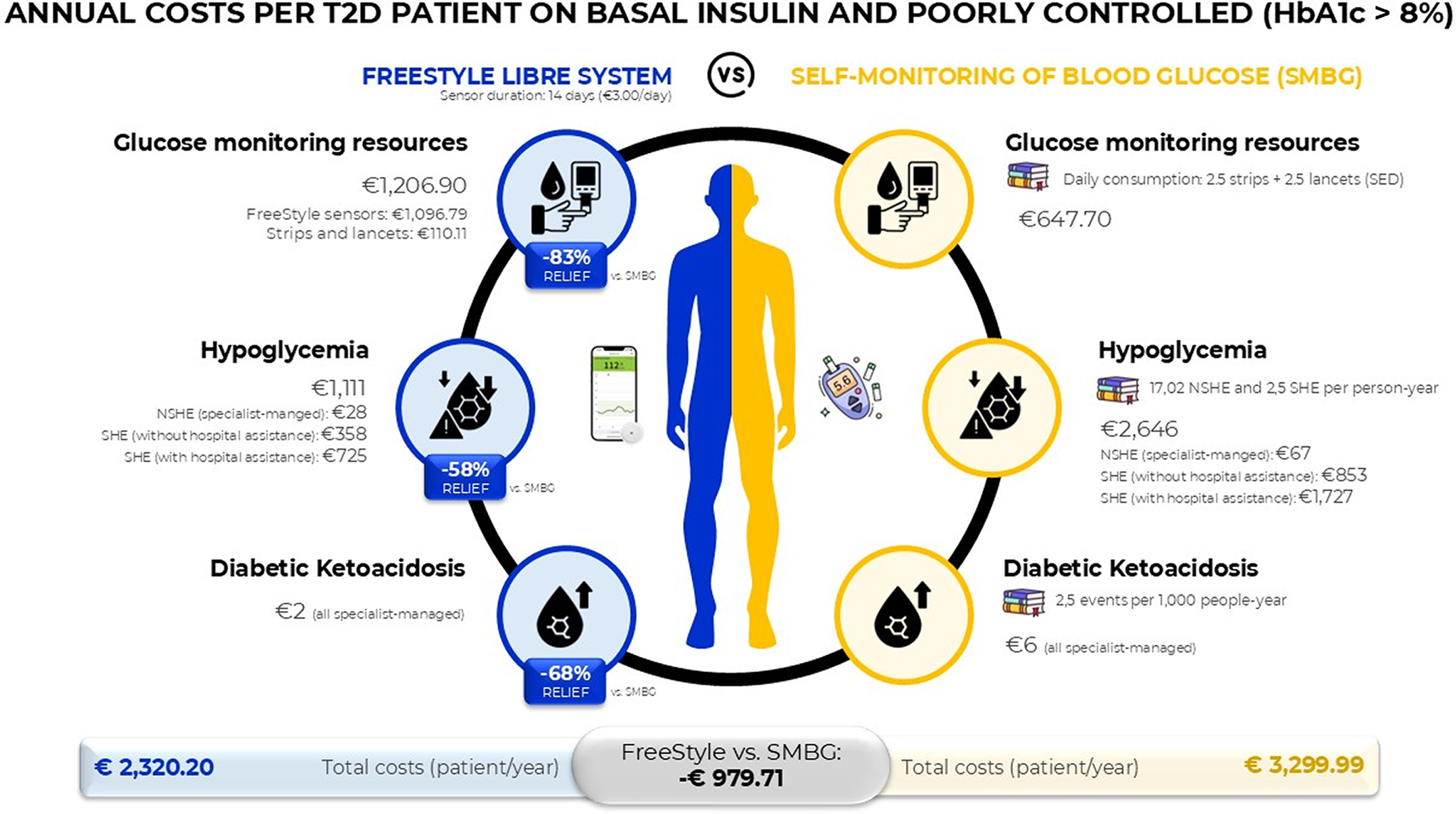
Visual summary of the base case results. HbA1c, glycated hemoglobin A1c; NSHE, nonsevere hypoglycemic event; SHE, severe hypoglycemic event.
In a cohort of 1000 patients with T2D on basal insulin and poorly controlled (HbA1c < 8%), the total number of acute events that would occur in the SMBG cohort was 19,523 versus 8199 in the FreeStyle Libre cohort, meaning that the device would prevent 11,324 acute events (−58.0%). Among those acute events, both SMBG patients and FreeStyle Libre patients would experience 3727 and 1565 specialist-managed NSHEs, respectively. SHEs would occur in 2500 patients on SMBG, of whom 653 required hospital assistance (142 would require admission). For the FreeStyle Libre cohort, a total of 1050 SHEs were estimated, of which 274 were hospital assisted (59 required hospitalization). With respect to specialist-managed DKA, 2.2 events would occur in the SMBG cohort, whereas 0.7 events would arise in the FreeStyle Libre cohort (Table 3).
Base Case Results: Events, Glucose Monitoring Resource Consumption, and Cost Estimates for a Cohort of 1000 Patients with Type 2 Diabetes on Treatment with Basal Insulin
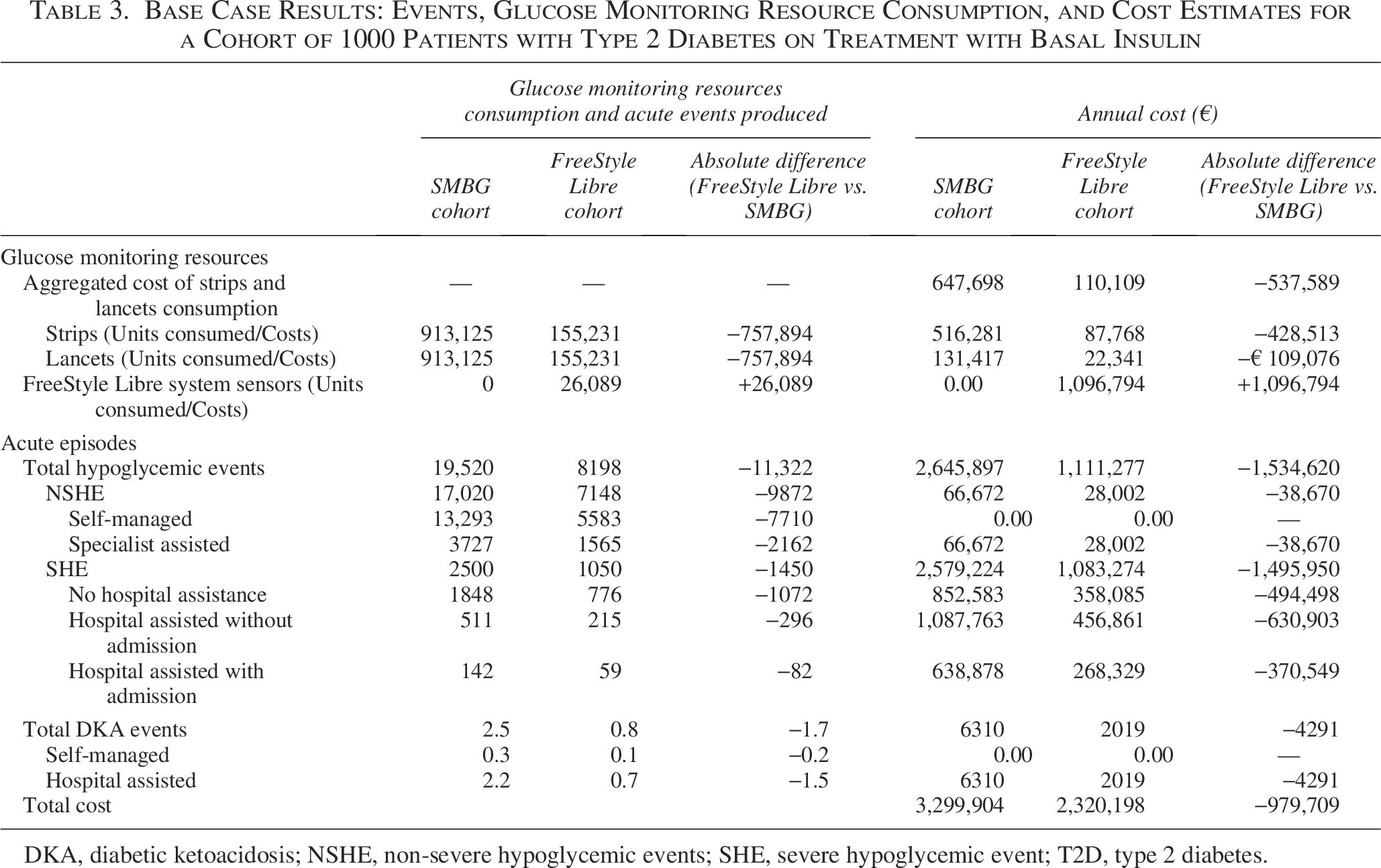
DKA, diabetic ketoacidosis; NSHE, non-severe hypoglycemic events; SHE, severe hypoglycemic event; T2D, type 2 diabetes.
The use of FreeStyle Libre systems in 1000 patients with T2D treated with basal insulin and HbA1c >8% would generate annual savings that increased to €979.706 compared with SMBG (Table 3), representing a reduction of 29.7% in overall costs.
Sensitivity analysis results
Savings were observed in all the OWSAs performed (Fig. 2). However, these analyses revealed that the reduction in hypoglycemia associated with FreeStyle Libre was the most sensitive input, resulting in a variation in the results of ±31.3% from the base case when the value was modified to ±20% (base case: 58%; OWSA: 46.4%−69.6%). The daily cost of the FreeStyle Libre sensors was the second most sensitive parameter, which resulted in a variation of ±22.5%, followed by the proportion of patients experiencing SHEs who required hospital admission (±16.9%).
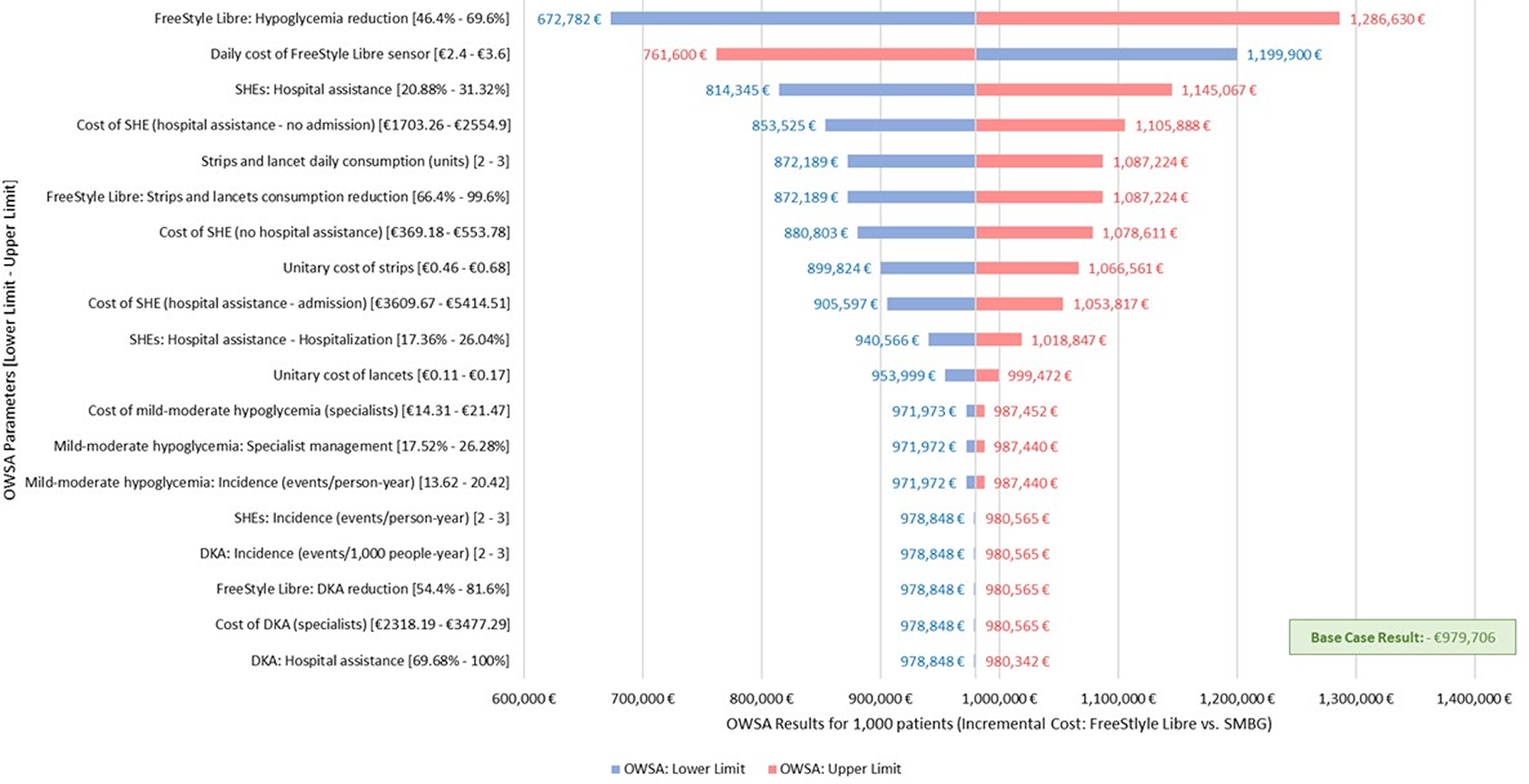
OWSA results for 1000 patients with T2D on basal insulin. DKA, diabetic ketoacidosis; OWSA, one-way sensitivity analysis; SMBG, self-monitoring of blood glucose; T2D, type 2 diabetes.
In addition, the OWSAs varying the key parameters of the model informed by the experts found that the alternative reduction in hypoglycemia associated with the use of FreeStyle Libre (base case: −58% 21 ; OWSA: −29% 20 ) would reduce savings from €979.706 to €212.396 (−78.3% vs. base case). In contrast to the reduction in hypoglycemic events with FreeStyle Libre, the reduction in DKA (base case: −68% 21 ; OWSA: −52.1% 32 ) had a slight impact on the results (−€978.703; −0.10% vs. base case). When the rate of SHEs (base case: 2.5 events/person-year 34 ; OWSA: 1.4 events/person-year 46 ) was varied, the model estimated savings of €321.488 (−67.2% vs. base case), revealing the sensitivity of that input. Finally, the use of FreeStyle Libre would produce cost savings of €442.117 even if strips and lancets were free (−54.9% vs. base case).
Alternative scenario results
In the alternative scenarios, it was estimated that a total of 624 diabetic complications per year would be suffered by the 1000 patients receiving SMBG, which would be reduced to 501 due to the use of FreeStyle Libre (Fig. 3A). The annual costs associated with the management of diabetic complications in both the SMBG and FreeStyle Libre cohorts were estimated to be €3,745,869 and €2,886,785, respectively (Fig. 3B). Thus, the use of the FM system would produce savings of €879,085 exclusively associated with the management of diabetic complications. Considering acute and chronic diabetic complications, the total costs rose to €7,045,774 for the SMBG cohort and €5,186,982 for the FreeStyle Libre cohort. In this scenario, the use of FreeStyle Libre would save €1,858,791 (−26.4%) per year to the NHS.
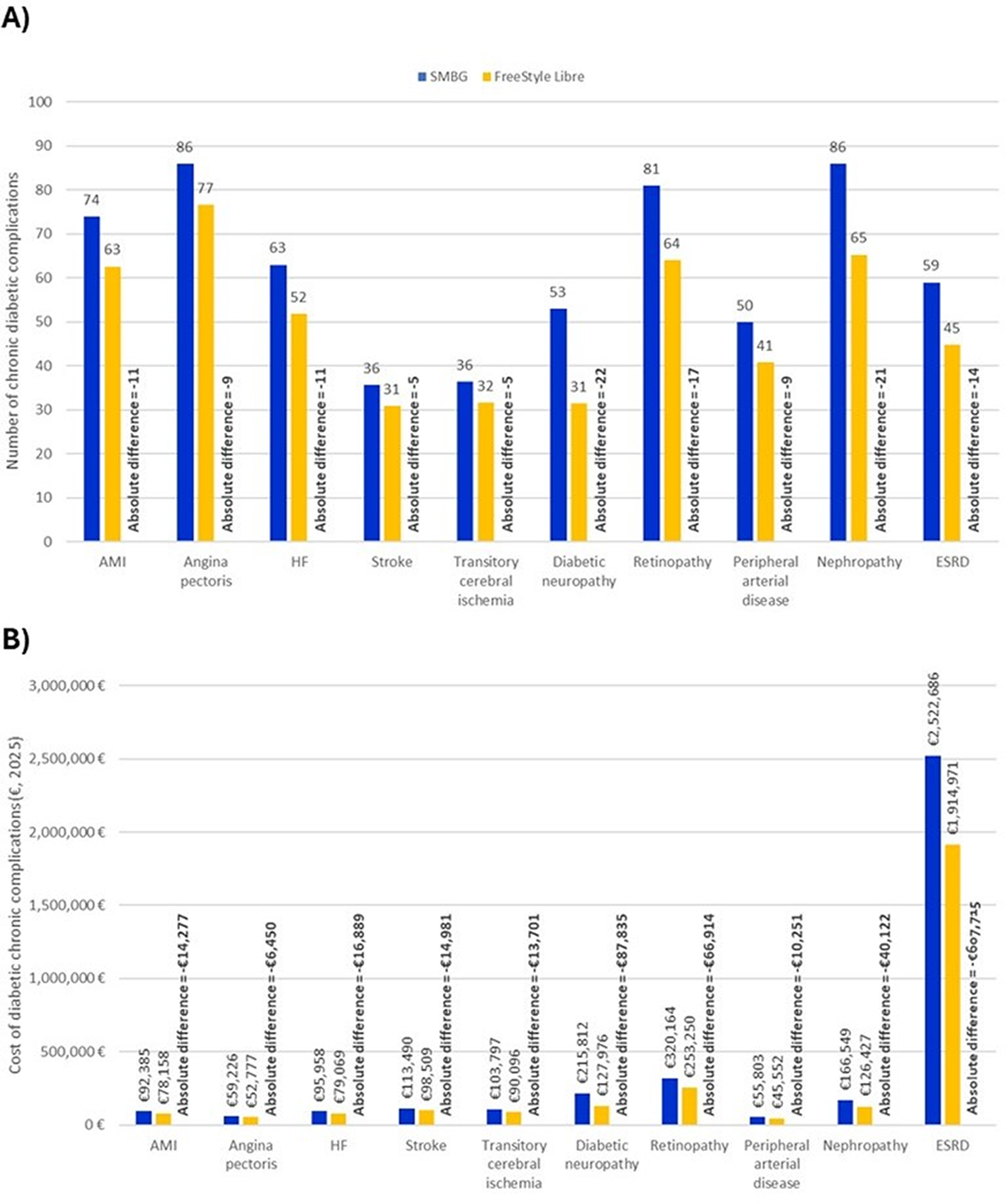
Alternative scenarios: Events and associated costs of diabetic complications in a cohort of 1000 patients with T2D on basal insulin. AMI, acute myocardial infarction; ESRD, end-stage renal disease; HF, heart failure.
In the second alternative scenario, including the work absenteeism associated with T2D, it was estimated that the 1000 patients in the SMBG cohort would lose a total of 3167 workdays, representing an indirect cost of €237,990. The model estimated 1317 lost workdays and an indirect cost of €99,004 for the cohort receiving FreeStyle Libre, which would produce savings of €138,986. Considering acute events, chronic diabetic complications, and indirect costs due to work absenteeism, a total cost of €7,283,763 was estimated for the SMBG cohort, which decreased to €5,285,986 for the cohort using FreeStyle Libre. In this setting, the use of FreeStyle Libre would produce annual savings of €1,997,777 (−27,4%) to society.
Discussion
Real-world data (RWD) have been key to capturing the clinical effectiveness of FreeStyle Libre systems in the population with T2D on basal insulin to reduce hypoglycemia and DKA. 21 The systems also showed a reduction in HbA1c associated with their use, 57 which translates into a decrease in the risk of acute and chronic diabetic complications. 48 In this setting, the evaluation of the economic impact of the use of FreeStyle Libre systems in these patients is key for decision-making.
In the base case of this cost analysis, the use of the FreeStyle Libre systems in people with T2D on basal insulin and poorly controlled (HbA1c > 8%) would result in annual cost savings for the Spanish NHS of nearly €980 per patient, representing a reduction of 29.7% from the current cost of managing these patients with SMBG (approximately 3300 per patient-year). The savings proceeded mainly from reducing SHEs using FreeStyle Libre systems compared with SMBG, which represented savings of €1455 per patient. When considering chronic diabetic complications and work absenteeism, the overall annual cost savings per patient would rise to €1998.
Previous studies conducted in Spain found that FreeStyle Libre also led to cost savings in other populations. A previous cost analysis of FreeStyle Libre in patients with T1D, 29 which considered only the cost derived from the glycemic monitoring and management of hypoglycemic events, estimated annual cost savings of €1911 (currency from 2019) per patient when the device was used compared with the use of SMBG. 29 Similarly, in patients with T2D receiving a basal-bolus insulin regimen, considering glucose monitoring resources and the management of SHEs, FreeStyle Libre was associated with savings of €581 (currency from 2020) per patient-year. 30
To the authors’ knowledge, this is the first analysis evaluating FreeStyle Libre systems for glucose monitoring in patients with T2D receiving basal insulin in Spain. However, other economic evaluations of the FreeStyle Libre systems in these patients have been conducted in other settings. A recently published cost–utility analysis (CUA) conducted in Italy provided insight into the use of FreeStyle Libre systems over the lifetime of patients with T2D on basal insulin therapy. 60 Despite the increase in costs associated with FreeStyle Libre of €5338 compared with SMBG (euros from 2023), the device was associated with 0.51 additional quality-adjusted life years (QALYs). Given that the incremental cost-effectiveness ratio was estimated at €10,556/QALY, FreeStyle Libre was shown to be cost-effective compared with SMBG. 60 Similarly, a CUA conducted from the Canadian private-payer perspective, published in 2024, revealed that FM systems represent a dominant intervention compared with SMBG, which means that patients using the devices lived more QALYs (+0.480) and achieved cost savings (CAD$8091). 61
In addition, the cost savings found in the population considered in the present and previous studies are supported by other RWD. 62 In the United States, a RWE study enrolling people with T2D using three different treatments, including noninsulin (n = 25,269), basal (n = 16,264), and prandial insulin (n = 33,146) regimens, revealed that CGM devices significantly reduced hospital admissions. 62 In patients receiving basal insulin, all-cause hospitalizations and hospital admissions caused by acute complications and visits to the emergency room were reduced by 13.9%, 47.6%, and 28.2%, respectively. 62
The present study provides a short-term analysis of the annual economic impact of the FreeStyle Libre systems, showing cost savings associated with their use in a poorly controlled T2D population treated with basal insulin and other antihyperglycemic agents. Moreover, it should be noted that the base case represented a conservative analysis, as neither diabetic long-term complications nor costs derived from work absenteeism were included. When diabetic complications were included, the savings in 1000 patients with T2D would increase to almost €1.85 million and €2.0 million if the reduction in work absenteeism is also considered.
Otherwise, several inputs of the base case could be critically assessed. First, the consumption of strips and lancets could be considered high compared with clinical practice. However, the sensitivity analysis considering both strips and lancets for free revealed that, even in this setting, FreeStyle Libre would produce cost savings.
The occurrence of SHEs might be another controversial input. The selected source reported one of the highest incidences among the wide range of data published. Nonetheless, the clinicians considered this study to represent the most robust source for the occurrence of SHEs owing to methodological aspects (study design, population representativeness, etc.). In addition, this source was also selected for the previous cost analysis of FreeStyle Libre in patients with T2D. 30 In any case, the sensitivity analyses included the variation of this source, leading to a reduction in costs estimated at €212,000 when the rate of SHEs was 1.4 events/person-year. 46
The effectiveness of the FreeStyle Libre systems may be another source of uncertainty in the model. In this context, there were several reasons for the use of RWE studies. Compared with clinical trials, the RWD provides a more faithful reflection of clinical practice, highlighting a strength of this economic evaluation. Moreover, the RWE studies included patients with T2D on basal, which aligned with the target population of the cost analysis. In contrast, both studies were conducted in France. Thus, further research should be conducted in Spain to provide national evidence for these economic studies. Sensitivity analyses considering alternative studies20,32 revealed that FreeStyle Libre would save costs even with lower effectiveness.
Finally, the source considered for modeling absenteeism consisted of a study involving 1054 participants with T1D (77.2%), 223 with T2D (16.3%), and 88 with other forms of diabetes (6.5%). 58 This study represented the unique source comparing the absenteeism before and after using FreeStyle Libre. Thus, indirect costs were modeled under the assumption that absenteeism in a mixed cohort of patients with T1D and T2D would be applicable to those patients with T2D exclusively. For this reason, the results considering the societal perspective should be interpreted with caution, as slight variations in the indirect cost estimated should be expected.
Besides the potential reduction in acute events and savings, the availability of FreeStyle Libre for patients with T2D on basal insulin and HbA1c > 8% could have further clinical implications. The use of FM sensors would reduce the frequency of SMBG measurements and, thus, the consumption of strips and lancets. According to the results of the present study, a patient on SMBG would use a total of 913 strips and lancets annually for glucose monitoring, whereas a patient using FreeStyle Libre would use only 155 strips and lancets annually, leading to a reduction of 758 units per patient per year. The reduction in the consumption of these resources translates into annual savings of €538 per patient. However, its clinical implications should also be examined. In addition, low adherence to the SMBG recommendations has been reported in several studies,63,64 often due to time constraints, procedural invasiveness, or the fear of needles.64,65 FreeStyle Libre may address these barriers, improving adherence to glucose monitoring. 66
Furthermore, the FreeStyle Libre systems increased patients’ reported outcomes, improving their quality of life and experience. A study conducted in Saudi Arabia, including patients aged 13–19 years with T1D, reported that between 80% and 95% of the participants agreed that the application of FreeStyle Libre sensor was less painful than the finger stick, and it was easy to wear because of its small size, its low interference with daily activities, and its capacity to adapt to patients’ lifestyles. These individuals also valued being able to scan the sensor without being noticed by other people, which is particularly favorable for avoiding stigmatization. In addition, improvements in distress and sleep quality were observed as measured by Diabetes Distress Scale and Pittsburg Sleep Quality Index, respectively, after the use of the FreeStyle Libre for 3 months. 67 In Japanese patients with T2D, improvements in physical activity, measured by the International Physical Activity Questionnaire, and overall satisfaction with the treatment, measured by the Diabetes Treatment Satisfaction Questionnaire, were also observed from baseline to 12 weeks after glucose monitoring with the sensor was started. 68
Conclusions
This economic analysis estimated that the use of FreeStyle Libre systems in patients with T2D and HbA1c levels greater than 8% receiving basal insulin therapy, with or without other antihyperglycemic agents, is associated with significant potential cost savings to the Spanish NHS. In a cohort of 1000 poorly controlled patients with T2D on a basal insulin regimen, FreeStyle Libre is estimated to produce annual cost savings of €979,709 for the NHS compared with conventional SMBG. In addition to reducing acute complications (hypoglycemia and DKA), FreeStyle Libre may also decrease the occurrence of chronic diabetic complications and work absenteeism, leading to additional cost savings for society as a whole. Furthermore, the convenience of using these devices would improve patients’ well-being, extending the benefits of FreeStyle Libre systems beyond economic savings.
Authors’ Contributions
F.J.A.-B., V.B., A.M.C.-C., P.M.-R., J.C.-G., A.-M.H.M., and F.G.-P. participated in the validation of the model inputs, interpretation of the results, and drafting and validation of the final version of the article. A.D.L.C.-G. and I.O. participated in the conceptualization of the study, development of the economic model, interpretation of the results, and article drafting.
Footnotes
Acknowledgments
The authors acknowledge Manuel Gómez-Barrera for his collaboration in the drafting of this article as a medical writer. In addition, the authors are grateful to Lourdes Betegón, Javier Núñez-Alfonsel, Francisco Silla, Jack Timmons, and Mireya Robles-Plaza for their invaluable support during the study.
Author Disclosure Statement
F.J.A.-B. has served as a consultant/advisor for
Funding Information
This study was funded by Abbott Diabetes Care.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.