
Abstract
Background:
Continuous glucose monitoring (CGM) and intermittently scanned CGM (is-CGM) have shown to effectively manage diabetes in the specialty setting, but their efficacy in the primary care setting remains unknown. Does CGM/is-CGM improve glycemic control, decrease rates of hypoglycemia, and improve staff/physician satisfaction in primary care? If so, what subgroups of patients with diabetes are most likely to benefit?
Methods:
A comprehensive search in seven databases was performed in June 2021 for primary studies examining any continuous glucose monitoring system in primary care. We excluded studies with fewer than 20 participants, specialty care only, or hospitalized participants. The National Heart, Lung and Blood Institute and Grading of Recommendations Assessment, Development and Evaluation were used for the quality assessment. The weighted mean difference (WMD) of HbA1c between CGM/is-CGM and usual care with 95% confidence interval was calculated. A narrative synthesis was conducted for change of time in, above, or below range (TIR, TAR, and TBR) hypoglycemic events and staff/patient satisfaction.
Results:
From ten studies and 4006 participants reviewed, CGM was more effective at reducing HbA1c compared with usual care (WMD −0.43%). There is low certainty of evidence that CGM/is-CGM improves TIR, TAR, or TBR over usual care. The CGM can reduce hypoglycemic events and staff/patient satisfaction is high. Patients with intensive insulin therapy may benefit more from CGM/is-CGM.
Conclusions:
Compared with usual care, CGM/is-CGM can reduce HbA1c, but most studies had notable biases, were short duration, unmasked, and were sponsored by industry. Further research needs to confirm the long-term benefits of CGM/is-CGM in primary care.
Keywords
Introduction
Diabetes mellitus continues to result in considerable morbidity and mortality worldwide, primarily through its strong association with increased cardiovascular and all-cause mortality,1,2 but also through vision loss, amputations, chronic kidney disease, and stroke. 3 Although diabetes-related complications have decreased significantly between 1990 and 2010, 4 recent epidemiological studies show that the global prevalence of diabetes mellitus, particularly type 2 diabetes, continues to rise. 5 Numerous studies have shown that optimal glycemic control reduces the risk of morbidity6,7 but has proven to be elusive in a significant portion of the patient population living with diabetes. 8
Continuous glucose monitoring (CGM) and intermittently scanned CGM (is-CGM) are evolving technologies with the potential to add precision to the monitoring and management of diabetes. Both involve the use of subcutaneous sensors that sample interstitial glucose levels, which can be used to alert the patient when the glucose trend is expected to reach hypoglycemia or hyperglycemia. In CGM, the device records glucose levels 280 times per day and are worn for ten days. 9 Intermittently scanned CGM (is-CGM), also called flash glucose monitoring (FGM) in some countries, uses similar approaches, but values are measured on demand, up to every minute. There are three different versions of is-CGM systems worldwide (Freestyle Libre, Freestyle Libre Pro, and Freestyle Libre 2).
Recently, both the American Diabetes Association and the American Association of Clinical Endocrinology have issued recommendations supporting the use of CGM/is-CGM for patients using multiple daily insulin injections (MDIs), infusion pumps, and for patients on noninsulin therapies.10,11 The recent increase in use has also resulted in multiple articles in the primary care literature regarding interpretation, 12 integration into clinical workflows,13,14 and reimbursement.15,16 In addition, direct advertising to health care providers and the public has brought further attention to this technology. 17
The CGM and is-CGM use in the specialty care setting is well documented. However, surveys have shown that there is an insufficient number of endocrinologists to care for the large and growing population of patients with diabetes; it is estimated that the US primary care workforce cares for 85% of patients with diabetes. 18 In many countries, people with type 1 diabetes are treated exclusively at the specialist level or in co-management with their primary care physician (PCP). However, most patients have type 2 diabetes, the majority of whom are cared for by primary care, including those managed with insulin. The evidence for widespread use of CGM/is-CGM in patients living with type 2 diabetes is limited 19 and our search showed there are no published systematic reviews for evaluating the use of CGM/is-CGM in the primary care setting. This systematic review aimed to answer the following questions: In primary care, does the use of CGM/is-CGM in patients with diabetes result in improved glycemic control, decreased rates of hypoglycemia, and improved patient and staff satisfaction? If so, what subgroups of primary care patients with diabetes are most likely to benefit?
Methods
This systematic review follows the Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines 20 and the checklists are available in Online Appendices A and B.
Sources and Search
A comprehensive literature search was conducted in January 2021 by a medical librarian specialized in systematic reviews (L.Ö.). The search was updated in June 2021. Seven biomedical and health sciences databases, PubMed (NML), MEDLINE (Clarivate), EMBASE (Elsevier), Scopus (Elsevier), CINAHL (EBSCOhost), Cochrane Library (Cochrane) and Web of Science (Clarivate), were searched from their inception.
A combination of the search fields “Text Word” (alternatively title, abstract, and keywords) and MeSH/thesaurus terms (when available) was used to locate the best available evidence. The search was performed without any geographical or publication year restrictions. A filter for English language was applied.
Cabell’s Predatory Report (Cabell’s Scholarly Analytics, 2021) 21 was consulted to confirm that none of the finally selected papers were affiliated with potentially predatory publishers or journals. Detailed search reporting of all included sources is available in Online Appendix C.
Study Selection
All records identified in the database search were exported to the Covidence systematic review software (Veritas Health Innovation, 2021) 22 for automatic de-duplication, screening, and extraction. Two reviewers independently performed title and abstract (R.D.G. and J.K.) and full-text screening (A.K. and J.K.), including primary studies involving the use of any continuous glucose monitoring system in patients with diabetes (type 1, type 2, and gestational) under the care of a primary care provider, including those co-managed with an endocrinologist. Some studies included patients co-managed by their PCP and an endocrinologist, which reflects the pragmatic study design. In actual practice, PCPs may need consultation with endocrinology. We included these studies to reflect this real-world collaboration to encourage PCPs to consider this practice. Exclusion criteria include gray literature, studies with fewer than 20 participants, participants managed only by an endocrinologist, participants hospitalized or critically ill, and studies where participants used closed-loop systems where the device automatically adjusts the infusion of insulin based on the glucose results. A third reviewer independently resolved any conflicts at each step with the support of the Covidence software. A PRISMA flow diagram of the selection process is available in Figure 1.
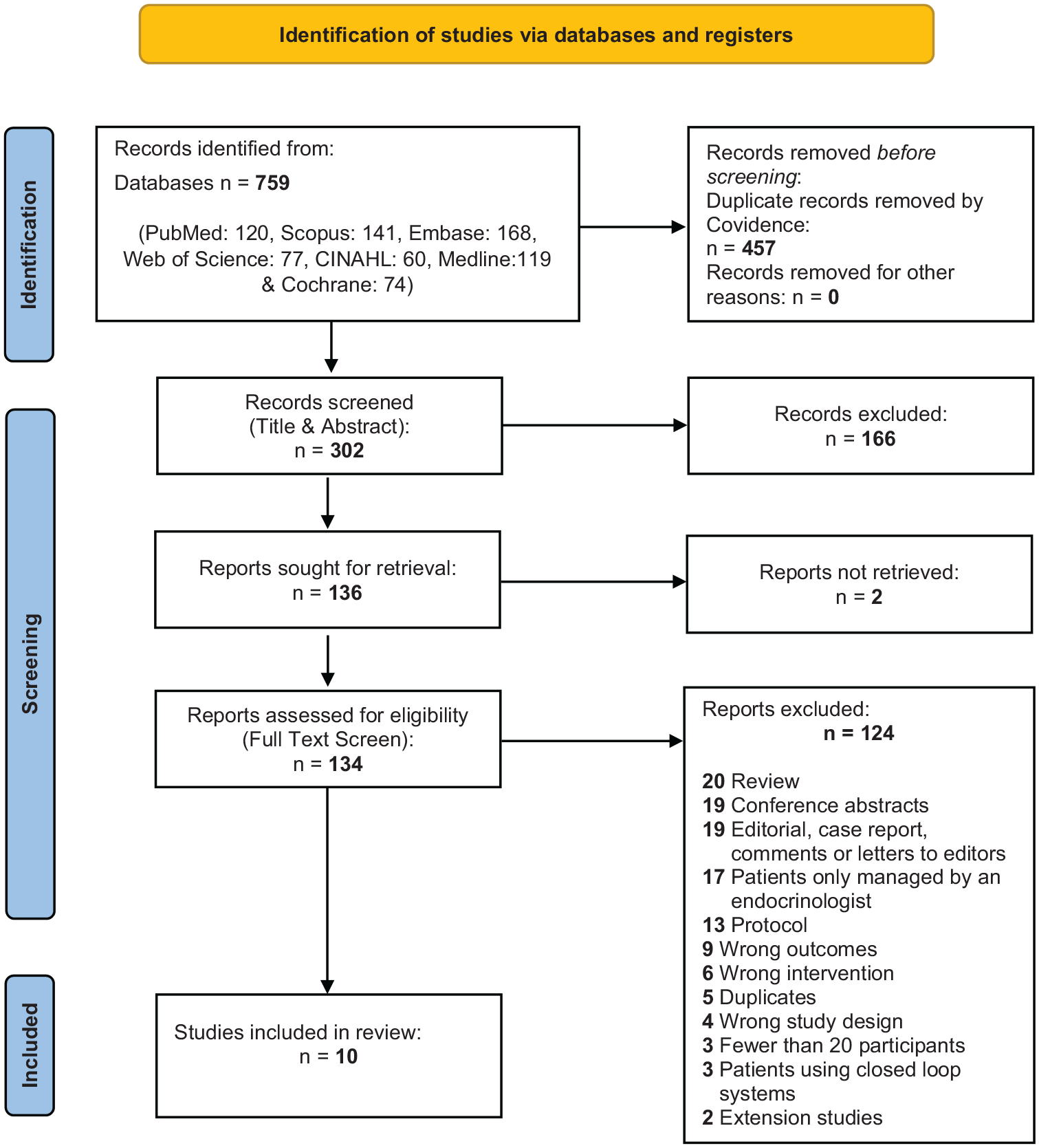
PRISMA 2020 flow diagram detailing the search, de-duplication, screening, and selection process.
Data Extraction
Two independent reviewers (A.K. and J.K.) used the Covidence software to extract study characteristics and outcomes. The primary outcome assessed was the change in HbA1c from baseline. The secondary outcomes included the change in percentage of time in range (TIR), time above range (TAR), and time below range (TBR); complications, including hypoglycemic events; physician/staff and patient satisfaction; and data on which subgroups benefit most from CGM/is-CGM, if reported. In addition, each study’s funding sources and conflicts of interest were extracted. These outcomes were compared with usual care, which, in most cases, was self-monitoring of blood glucose (SMBG) with HbA1c. A third reviewer (R.D.G.) resolved conflicts.
Quality Assessment
Two independent reviewers (A.K. and J.K.) used the National Heart, Lung and Blood Institute Quality Assessment Tools 23 and the Grading of Recommendations Assessment, Development and Evaluation 24 to assess the quality and risk of bias of each included study. The Covidence software enabled a systematic and blinded approach. A third reviewer (R.D.G.) resolved conflicts.
Data Synthesis
The study characteristics and outcomes of each study were summarized in a comprehensive table, which allowed us to group and compare similar relevant findings. For studies comparing our primary outcome, change in HbA1c, between CGM/is-CGM and usual care, the mean difference with 95% confidence intervals (CIs) was calculated using standard equations from the reported standard deviation (SD), standard error (SE), CI, and/or P values from each study. 25 If variability was reported as interquartile range, SD was estimated. 26 For studies without comparisons with usual care, the mean difference in HbA1c from baseline to study end was calculated. To accommodate the difference in the number of study participants between the studies when calculating the total mean difference in HbA1c, a weighted mean difference (WMD) was calculated. The WMD in HbA1c was calculated by summing the total mean difference in HbA1c among the ten studies and then taking the average of this total, assigning proportional weight based on the number of participants in each study. Meta-analysis was not performed due to the large heterogeneity of study designs, study participants, interventions, and outcome variables between the trials. The remaining findings, including secondary outcomes, patient/staff satisfaction, and which subgroups of persons with diabetes benefiting most from CGM/is-CGM, were analyzed through a narrative synthesis.
Results
As summarized in Figure 1, 1374 records were identified in the literature search. A total of 302 unique references remained after the automatic de-duplication in Covidence. After the title and abstract screening, 136 papers were selected for full-text screening, of which ten studies were identified eligible for the systematic review.
The total number study participants were 4006 among all ten studies. Four studies were randomized controlled trials (RCTs), one was a nonrandomized controlled trial (NRCT), three were cohort studies, and two were pre/post uncontrolled interventions. All participants were nonpregnant and 18 years or older. One study solely looked at type 1 diabetes mellitus (T1DM), five exclusively evaluated type 2 diabetes mellitus (T2DM), and four studies had a mixed population of T1DM and T2DM. Only two studies used is-CGM (FGM) and only two studies had prolonged and sustained CGM/is-CGM use. The characteristics of each study are compiled in Table 1 and the pertinent outcomes of all included studies are summarized in Table 2.
Summary of Characteristics of Included Studies.
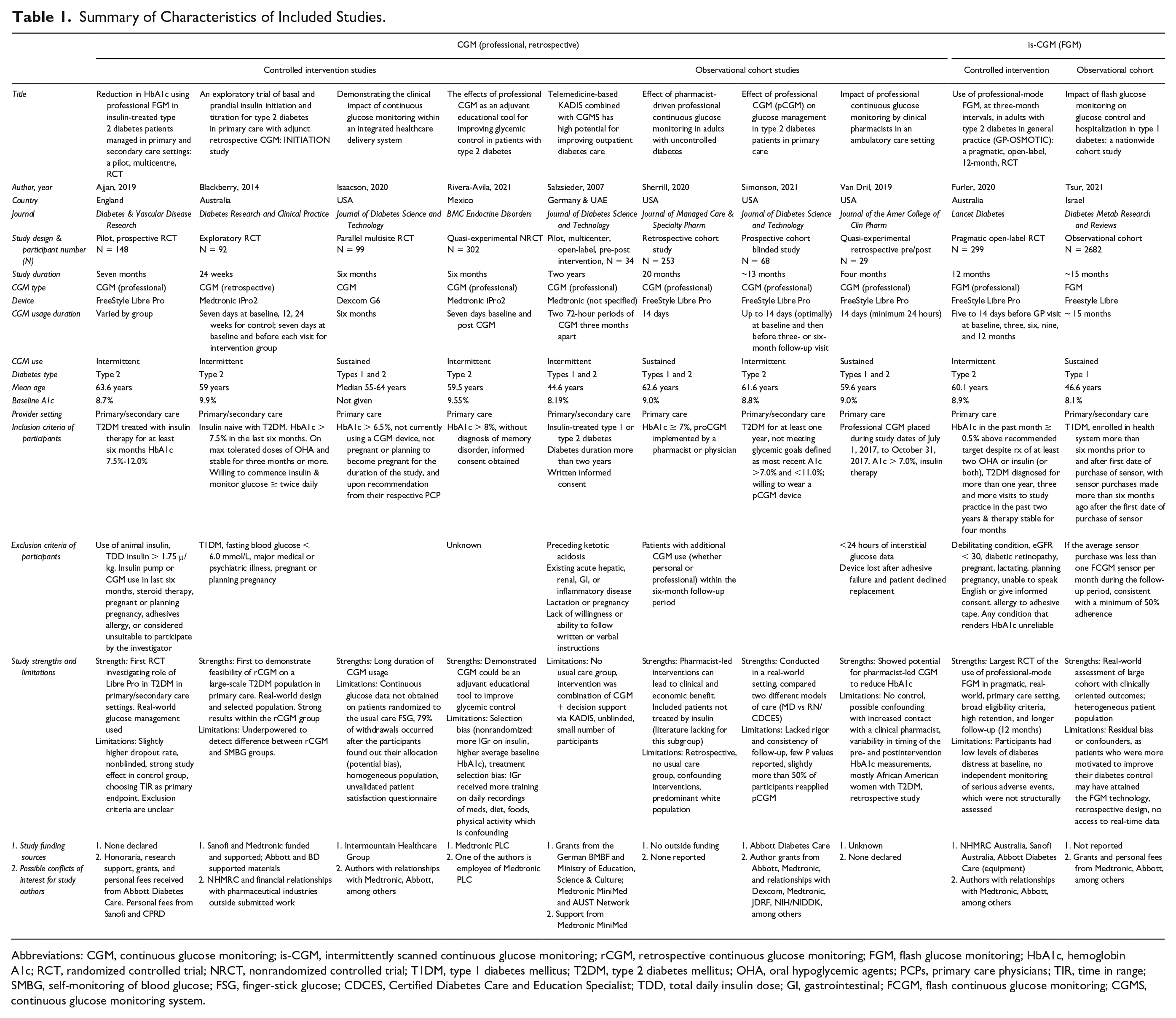
Abbreviations: CGM, continuous glucose monitoring; is-CGM, intermittently scanned continuous glucose monitoring; rCGM, retrospective continuous glucose monitoring; FGM, flash glucose monitoring; HbA1c, hemoglobin A1c; RCT, randomized controlled trial; NRCT, nonrandomized controlled trial; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; OHA, oral hypoglycemic agents; PCPs, primary care physicians; TIR, time in range; SMBG, self-monitoring of blood glucose; FSG, finger-stick glucose; CDCES, Certified Diabetes Care and Education Specialist; TDD, total daily insulin dose; GI, gastrointestinal; FCGM, flash continuous glucose monitoring; CGMS, continuous glucose monitoring system.
Summary of Outcomes of Included Studies.
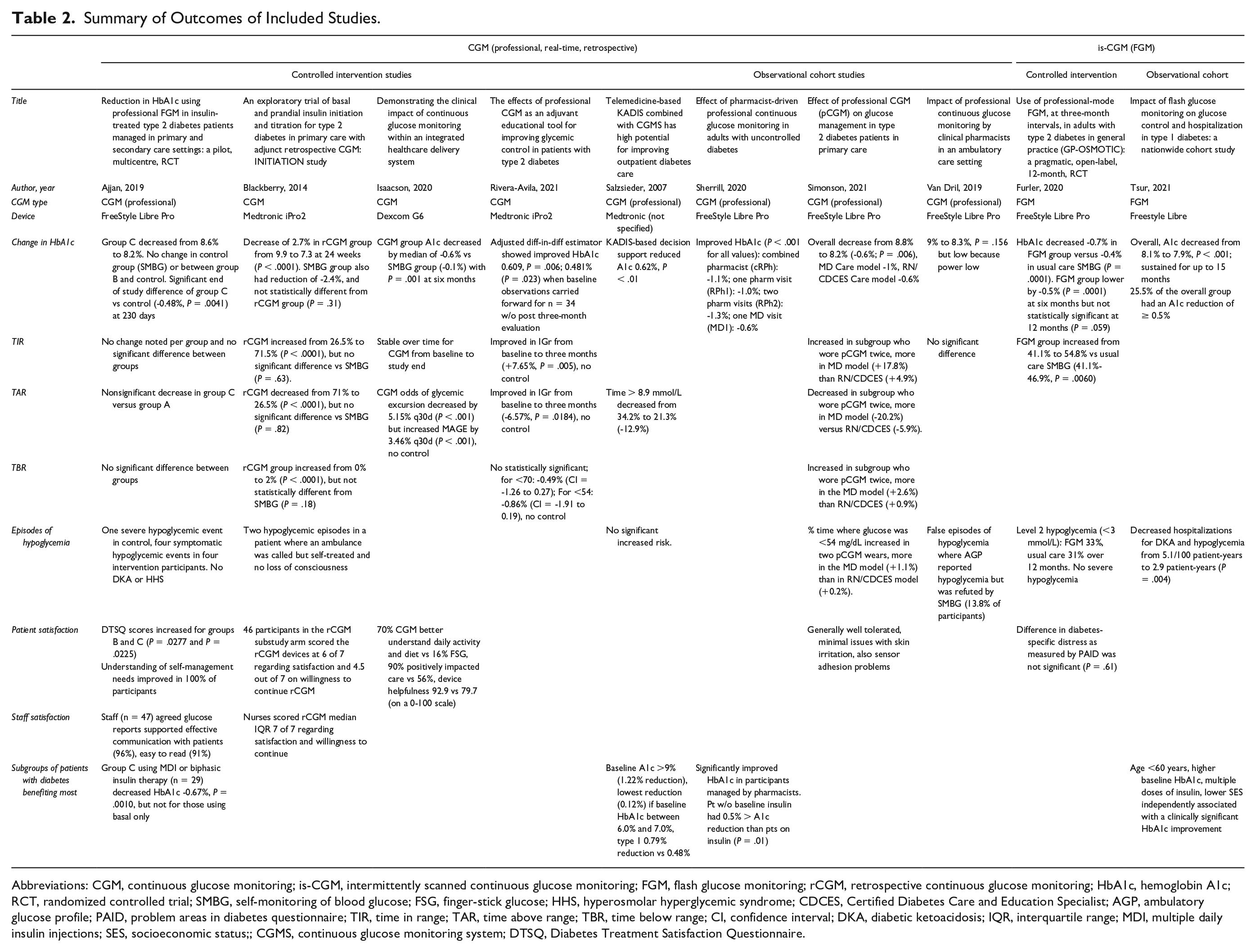
Abbreviations: CGM, continuous glucose monitoring; is-CGM, intermittently scanned continuous glucose monitoring; FGM, flash glucose monitoring; rCGM, retrospective continuous glucose monitoring; HbA1c, hemoglobin A1c; RCT, randomized controlled trial; SMBG, self-monitoring of blood glucose; FSG, finger-stick glucose; HHS, hyperosmolar hyperglycemic syndrome; CDCES, Certified Diabetes Care and Education Specialist; AGP, ambulatory glucose profile; PAID, problem areas in diabetes questionnaire; TIR, time in range; TAR, time above range; TBR, time below range; CI, confidence interval; DKA, diabetic ketoacidosis; IQR, interquartile range; MDI, multiple daily insulin injections; SES, socioeconomic status;; CGMS, continuous glucose monitoring system; DTSQ, Diabetes Treatment Satisfaction Questionnaire.
Glycemic Control
Our results suggest that CGM/is-CGM may be more effective at lowering HbA1c than usual care by a WMD of −0.43% (12 mg/dL, 5 mmol/mol) from the RCTs.27-31 Figure 2 depicts the mean differences with 95% CIs in the five controlled interventional trials (four RCTs and one NRCT).27-31 Only one of three RCTs showed that CGM/is-CGM improved TIR compared with usual care27-29 and neither of the two RCTs comparing TAR and TBR of CGM with usual care showed a significant difference.27,28 The certainty of evidence found in the RCTs is moderate and details of our quality assessment are found in Supplementary Figure 1 and Table 3.
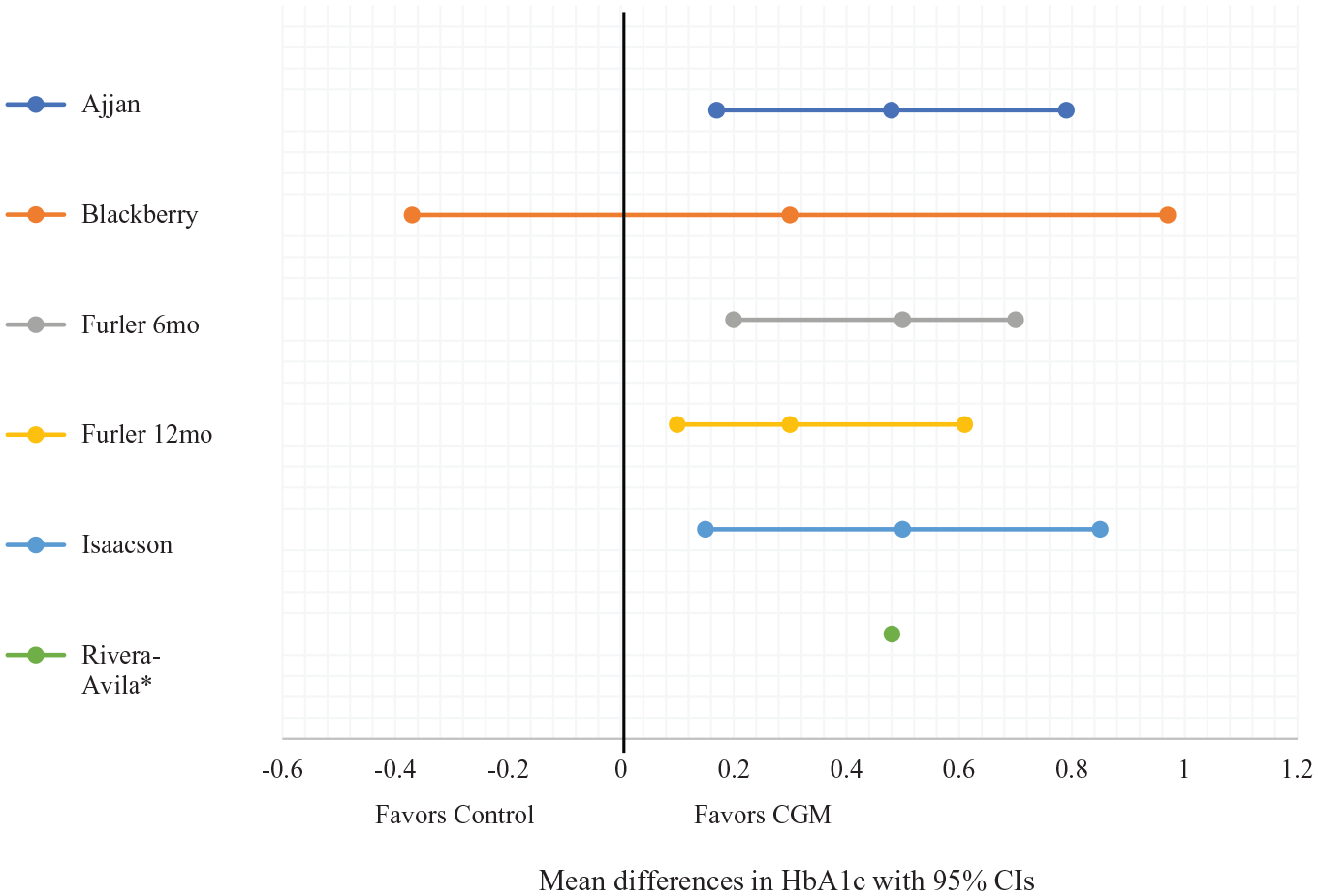
Forest plot of mean differences with 95% CIs of HbA1c at study end between the intervention (CGM) and control groups.
Summary of GRADE Assessment.
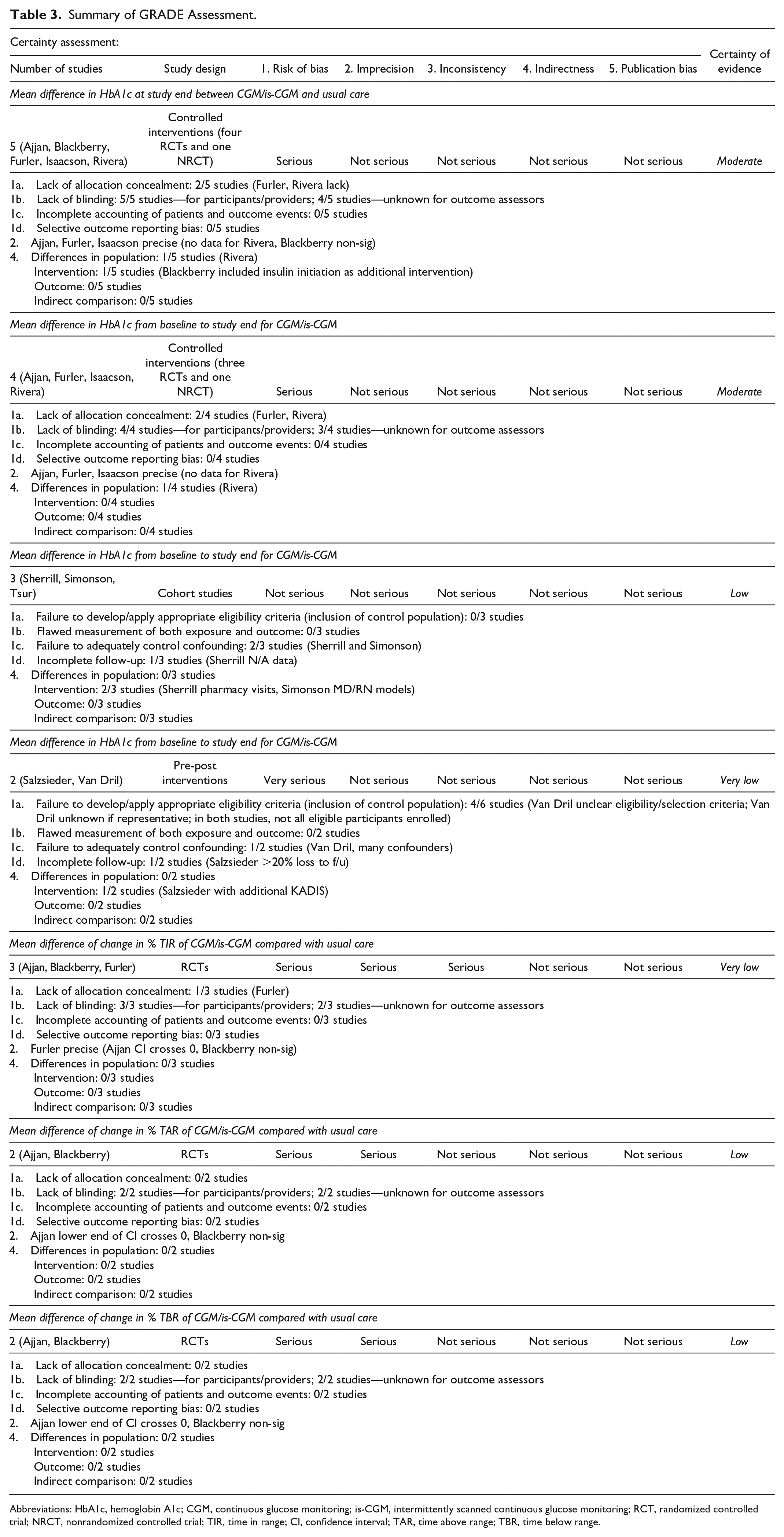
Abbreviations: HbA1c, hemoglobin A1c; CGM, continuous glucose monitoring; is-CGM, intermittently scanned continuous glucose monitoring; RCT, randomized controlled trial; NRCT, nonrandomized controlled trial; TIR, time in range; CI, confidence interval; TAR, time above range; TBR, time below range.
Inclusive of all studies (RCTs, cohort, pre-post), without comparing to usual care, eight of ten studies demonstrated CGM/is-CGM significantly reduced HbA1c from baseline to study end by a WMD of −0.31% (9 mg/dL, 3 mmol/mol).27-36 However, the certainty of evidence is low to moderate, depending on the study design, which is summarized in Supplementary Figure 1 and Table 3.
We have grouped the analysis of each outcome by diabetes type to better assist the reader in navigating the body of existing literature.
Type 2 diabetes
Two RCTs demonstrated CGM/is-CGM improved HbA1c at 230 days after implementation (8.6%-8.2%, P = .004) 27 and six months (P < .001) 29 respectively, but not at 12 months (P = .059). One NRCT showed improved HbA1c in CGM than control by 0.481%, P = .023 (using adjusted diff-in-diff estimator) after three months. 31 Although one RCT suggested is-CGM (FGM, Freestyle Libre Pro) can improve TIR (P = .006), 29 another exploratory RCT concluded no statistically significant difference between CGM and SMBG in HbA1c, TBR, TIR, and TAR. 28
One cohort study demonstrated a HbA1c reduction of 0.6% (P = .006) at three to six months post-CGM and improvement in TIR and TAR (+17.8% and −20.2% in MD model, +4.9% and −5.9% in RN/Certified Diabetes Care and Education Specialist [CDCES] model, respectively). 34
Type 1 diabetes
A large observational cohort study found that HbA1c declined from 8.1% to 7.9% after three months (P < .001) and was sustained for up to 15 months. In addition, about 25.5% of the overall group recorded a HbA1c reduction of ≥0.5%. 34
Studies including both T1DM and T2DM
One RCT demonstrated CGM can reduce HbA1c an additional −0.5% compared with SMBG (P = .001) 30 and one cohort study also demonstrated reduced HbA1c after six months of CGM use. 33
One pre/post study showed CGM can decrease HbA1c by 0.62% (P < .01) and TAR from 8.2 to 5.1 hours a day (P < .05), 34 but the other did not record any significant difference. 36
Decreased Rates of Hypoglycemia
Three studies looked at TBR. Two RCTs did not find a significant difference in TBR between CGM and usual care,27,28 but one study reported that their subgroup of participants who wore CGM for an additional time period increased their TBR (+2.6% in MD model and +0.9% in RN/CDCES-model). 34
One cohort study found is-CGM (FGM) use reduced overall hospital admissions for hypoglycemia (from 5.1/100 patient-years to 2.9, P = .004), as well as hospitalizations for diabetic ketoacidosis (DKA)/hypoglycemia (P = .004). 35 One RCT reported no episodes of DKA or hyperosmolar hyperglycemic syndrome, although a greater percentage of their participants on CGM experienced hypoglycemia (4.2% vs 1.9%). 27 Two more studies demonstrated no significant increased risk of hypoglycemia with CGM 32 or is-CGM (FGM) use compared with usual care over 12 months. 29
Patient and Staff Satisfaction
Patient satisfaction
A variety of patient satisfaction questionnaires were used between the studies. The Diabetes Treatment Satisfaction Questionnaire reported CGM helped participants improve their understanding of self-management needs (100%), glucose abnormalities (96%), treatment changes (99%), and how therapies work (99%). 27 The Audit of Diabetes Dependent Quality of Life questionnaire found participant satisfaction was higher for the CGM group, scoring 6 out of 7 (P = .031). 28 One study found a nonsignificant difference between the is-CGM (FGM) group and the usual care group in the Problem Areas in Diabetes, a diabetes-specific distress scoring scale. 29 Another study found patient satisfaction was higher in their CGM arm (90%) compared with SMBG (56%) and 70% in the CGM group reported better understanding of daily activity and diet compared with 16% for SMBG. 29
Staff satisfaction
Most health care professionals in one RCT reported that the CGM reports assisted in effective communication with patients (96%) and they were easy to read (91%) and understand (85%). 27 The staff nurses in the INITIATION study scored CGM at 7 out of 7 in terms of both satisfaction and willingness to continue CGM use. 28
Subgroups Benefiting From CGM/is-CGM
Certain subgroups benefited more from CGM/is-CGM. Participants using MDI therapy were independently associated with decreased HbA1c (P < .001). 35 Another study similarly showed that their participants with four CGM wears using MDI or biphasic insulin showed a larger decrease of HbA1c (0.67%, P = .001). 27 Participants with higher baseline HbA1c demonstrated that CGM/is-CGM can result in greater reductions in HbA1c (baseline HbA1c >9%: −1.22% vs HbA1c 6%–7%: −0.12% 30 and baseline HbA1c ≥8%: −0.6%, P < .001). 35 However, one cohort study found that patients not treated with insulin had a larger reduction in HbA1c than those treated with insulin (difference of 0.5%, P = .01). 33
HbA1c decreased for participants with low and medium socioeconomic status (SES, which is not defined in the study, P < .001) but not for high SES (P = .187). For age, HbA1c decreased in all ages (P < .001) except 61+ (P = .115). 35 In another study, participants with T1DM had a greater benefit of CGM use (−0.79% HbA1c reduction vs −0.48% in T2DM). 32
Discussion
Summary
Our review suggests, with moderate certainty of evidence, that CGM/is-CGM may be more effective at lowering HbA1c than usual care by a WMD of −0.43% (12 mg/dL, 5 mmol/mol)27-31 in the RCTs. However, according to our quality and risk of bias assessment, these five trials had notable biases, limiting our certainty of evidence. In addition, most of these trials were of short duration; only one trial evaluated the effects of is-CGM (FGM) beyond seven months and that study did not find significant HbA1c reduction at 12 months. 29 It is worth noting that CGM was not the main intervention in one of the studies; CGM was used to evaluate insulin initiation, but within the study design, participants using CGM were compared with participants using SMBG. 28
Regarding TIR, our review of three RCTs shows very low certainty of evidence that CGM/is-CGM is superior to usual care.27-29 Similarly, from our review of two RCTs, there is low certainty of evidence that CGM use results in improved TAR compared with usual care.27,28 For hypoglycemia, only one of four studies found that is-CGM (FGM) could decrease hospitalizations for DKA and/or hypoglycemia 35 and there is low certainty of evidence that CGM can reduce TBR compared with usual care.27,28
Studies have highlighted that only consistent use of CGM yields improved clinical outcomes,37-39 which suggests patient satisfaction is clinically relevant. Based on our review, CGM/is-CGM appears to have high patient satisfaction as all four studies measuring this outcome recorded generally favorable responses.27-30 Moreover, critical components of success with CGM/is-CGM are appropriate patient selection and adequate clinician training and support. Although our review of staff satisfaction with CGM was limited to two studies, both studies demonstrated positive responses.27,28
MDI therapy,27,32 higher baseline HbA1c,32,35 and T1DM 35 were variables resulting in more significant reductions in HbA1c. One study, however, did demonstrate greater HbA1c reduction in non-insulin-treated diabetes, but this study had significant heterogeneity among participants along with many confounding interventions influencing their results. 33
The included studies that used is-CGM utilized first-generation is-CGM devices that only allowed alerts for actual hypoglycemia and hyperglycemia. The advent of second-generation is-CGM allows the device to provide alerts for anticipated out-of-range values, which allows the patient to adjust their diet, exercise, and medication in real time. Further research on second-generation is-CGM is needed to evaluate benefits in glycemic control and avoidance of hypoglycemia.
Strengths and Limitations
To our knowledge, this analysis is the first to systematically review the clinical benefits of CGM/is-CGM specifically in primary care. The strengths include a comprehensive literature search; a clinically relevant summary of the benefits of CGM/is-CGM, including staff/patient satisfaction; an analysis of multiple diabetic subgroups; and the use of validated quality assessment tools. Acknowledged limitations include heterogeneity of study designs, study outcomes and participant baseline therapy which precluded rigorous meta-analysis, exclusion of non-English-language sources, and underpowered studies. Only two studies used is-CGM (FGM) and only two studies had prolonged and sustained CGM/is-CGM use, so we were unable to compare CGM with is-CGM and sustained use with intermittent use. In addition, we observed performance biases as no study blinded participants, detection biases as minimal studies blinded outcome assessors, and seven of ten studies were either funded by industry or disclosed possible conflicts of interest.
Although four studies yielded favorable patient satisfaction scores, no study specifically evaluated whether or to what extent individualized patient training was provided. Because adequate patient education is paramount for CGM/is-CGM benefit, future studies can evaluate how the quality and quantity of individualized patient training affects outcomes.
Comparison With Existing Literature
Our findings are consistent with Maiorino et al’s systematic review and meta-analysis of RCTs, which found that CGM modestly reduces HbA1c by 0.17% in unmasked short-term studies among persons treated with intensive insulin regimens. 40 Also complementing Maiorino’s et al’s findings, our review suggests that CGM/is-CGM may be more suitable for persons on intensive insulin therapy. 40 We cannot conclude whether SES has an association with CGM/is-CGM benefit as Tsur et al indicate low SES (SES not defined in their study) results in improved HbA1c, 32 but Tan et al’s baseline analysis of the GP-OSMOTIC study showed the opposite. 41
Interestingly, our review has shown that CGM/is-CGM can help lower HbA1c; however, similar benefit was not seen in two of three RCTs for TIR and both RCTs for TAR and TBR. This is inconsistent with both Maiorino et al and Beck et al’s findings.40,42 Ajjan et al attributed this discrepancy to the Hawthorne effect 27 and Blackberry et al’s study was not powered sufficiently to find a significant effect of CGM on HbA1c, TIR, TAR, or TBR compared with usual care. 28 Additional research is needed to determine whether this observation is related to study design or an actual difference in effects is present between CGM in primary care compared with specialty care.
Conclusions
Primary care providers should familiarize themselves with this new technology and utilize it in patients who would benefit from more rapid titration of insulin. Shared decision-making with the patient can set the appropriate shared expectation of modest benefit of glycemic control with minimal risk of hypoglycemia. In addition, with the acceleration of a shift to telemedicine, CGM technology can support both patient-centered out-of-office care and collaboration between the patient, the primary care provider, and, if needed, an endocrinologist in consultation.
As the complexity of diabetes management in the primary care setting continues to increase, 43 CGM/is-CGM is an attractive tool. This increasingly common technology has demonstrated benefit in T1DM and, to a lesser extent, T2DM. Because diabetes, particularly T2DM, is most commonly treated in the primary care setting, 44 this review focuses on CGM/is-CGM’s efficacy in a clinic environment where the attention and focus are not primarily on diabetes but also on screening, prevention, and the care of non-diabetes-related conditions. This review acknowledges the short-term benefit of CGM/is-CGM. However, before this promising technology becomes widely adopted into primary care practice, more research is required to confirm its long-term benefits of both improving glycemic control and reducing adverse events.
Supplemental Material
sj-docx-1-dst-10.1177_19322968211070855 – Supplemental material for The Benefits of Utilizing Continuous Glucose Monitoring of Diabetes Mellitus in Primary Care: A Systematic Review
Supplemental material, sj-docx-1-dst-10.1177_19322968211070855 for The Benefits of Utilizing Continuous Glucose Monitoring of Diabetes Mellitus in Primary Care: A Systematic Review by Alexander Kieu, Jeffrey King, Romona Devi Govender and Linda Östlund in Journal of Diabetes Science and Technology
Supplemental Material
sj-docx-2-dst-10.1177_19322968211070855 – Supplemental material for The Benefits of Utilizing Continuous Glucose Monitoring of Diabetes Mellitus in Primary Care: A Systematic Review
Supplemental material, sj-docx-2-dst-10.1177_19322968211070855 for The Benefits of Utilizing Continuous Glucose Monitoring of Diabetes Mellitus in Primary Care: A Systematic Review by Alexander Kieu, Jeffrey King, Romona Devi Govender and Linda Östlund in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
We thank Ms Mariam Al Ahbabi for her support in locating all full-text articles and for verifying the nonpredatory status of all included open access papers with the help of Cabell’s Predatory Report.
Abbreviations
CDCES, Certified Diabetes Care and Education Specialist; CGM, continuous glucose monitoring; CI, confidence interval; DKA, diabetic ketoacidosis; FGM, flash glucose monitoring; HbA1c, hemoglobin A1c; is-CGM, intermittently scanned continuous glucose monitoring; MDI, multiple daily injection (of insulin); NRCT, nonrandomized controlled trial; PCPs, primary care physicians; PRISMA, Preferred Reporting Items of Systematic Reviews and Meta-Analyses; rt-CGM, real-time continuous glucose monitoring; RCT, randomized controlled trial; SD, standard deviation; SES, socioeconomic status; SMBG, self-monitoring of blood glucose; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; TAR, time above range; TBR, time below range; TIR, time in range; WMD, weighted mean difference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Given this manuscript is a systematic review, an ethics approval was not obtained.
Registration and Protocol
This review was registered under PROSPERO, the international database of prospectively registered systematic reviews in health and social care (Registration No. CRD42021229416). A protocol was submitted and is currently under review.
Availability of Data,Code,and Other Materials
Data extracted from included studies and the data used for all analyses were obtained directly from each study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.