
Abstract
Aims
To estimate the global burden of chronic obstructive pulmonary disease (COPD) by age, gender and socioeconomic status from 2000 to 2021, and make a prediction until 2030.
Methods
Data were obtained from the Global Burden of Diseases, Injuries, and Risk Factors Study 2021. The burden of COPD, referred to absolute numbers of COPD case and age-standardized rates (ASRs) per 100,000 individuals per year. The temporal trends from 2000 to 2021 were examined using Joinpoint models. Bayesian age-period-cohort models were introduced to project the burden until 2030. Finally, a decomposition analysis was conducted to reveal the contributions of aging, population growth and epidemiological changes to trends in COPD burden.
Results
The crude numbers of incident cases, prevalent cases, deaths, and disability-adjusted life years (DALYs) for COPD remained increasing from 2000 to 2021, and until 2030, worldwide. ASRs of incidence, prevalence, deaths, and DALYs were in decreasing trends, and would continue to decline until 2030. Additionally, in 2021, the ASR of COPD burden was higher in males than females, while the age-specific rate increased with age. The disease burden varied across different regions, with a high burden in low development-level regions. The increasing burden of COPD was primarily driven by rapid aging and population growth.
Conclusions
The global ASRs of COPD burden would remain declining, but the crude burden would continue to increase until 2030. This study has public health implications for population-based interventions against COPD with consideration of residents’ age, gender and residing area as well as economic status.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common progressive pulmonary condition, characterized typically by chronic respiratory symptoms and irreversible airflow obstruction.1,2 COPD can significantly increase the susceptibility for patients to experience other unfavorable health-related consequence, such as heart failure, which is the main cause of hospitalization or/and death for COPD patients.3,4
According to estimates from the World Health Organization (WHO), COPD ranked the fourth top single cause of death worldwide, and accounted for 3.5 million deaths in 2021. 5 Moreover, of these deaths, nearly 90% occurred among individuals aged 70-years in low- and middle-income countries (LMICs). 5 Previous systematic reviews have reported that among adults aged 40+ years, the global prevalence of COPD surged from 7.6% in 2004 to 12.6% in 2022.6,7 Based on United Nations’ Sustainable Development Goals (SDGs), it is a primary target to reduce premature mortality from non-communicable diseases (including COPD) by one-third by 2030. 8 To align with the timeline of the United Nations’ SDGs, it is critically needed and particularly important not only to conduct ongoing and dynamic assessment of the global COPD burden but also to make projection of the burden until 2030.
Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) provides publicly available global data on disease and injury incidence, prevalence and mortality, allowing researchers to assess disease burdens worldwide. 9 Although the global burden of chronic respiratory diseases, including COPD, has been documented,10,11 all the existing literature estimated COPD burden over a period spanning the late 20th and early 21st centuries (e.g., 1990-2019), without a prediction until the future. Additionally, as major drivers of COPD incidence, population growth and aging, their contribution to COPD burden was not investigated worldwide,10,11 while the association of environmental risk factors with COPD burden has been examined well.12,13 Actually, from last century up to date, rapid economic development, lifestyle and behavior transition and changes in environmental risk factors occurred throughout the world, particularly in some specific countries. 14 Thus, it is of public health necessity and importance to systematically assess COPD burden based on data limited to this century and make a prediction for the next decade of this century.
To address this gap, using data from the GBD 2021 study, we conducted this comprehensive analysis with aims to estimate the burden of COPD at the global, regional and national levels over a period from 2000 to 2021, predict the global burden until 2030, and explore the contributions of aging, population growth and epidemiological change to the trends in COPD burden.
Methods
Data sources
Data on COPD were extracted from GBD 2021 study (https://vizhub.healthdata.org/gbd-results/). 9 The GBD study provides standardized estimates of incidence, prevalence, mortality and disability-adjusted life years (DALYs) in terms of annual case number and rate per 100,000 persons. 9 All of the estimates were reported with 95% uncertainty intervals (95%UI). 9 Details on measurement method and data topology of the GBD 2021 study were described elsewhere.9,15 (Data Source: Institute for Health Metrics and Evaluation. Used with permission. All rights reserved.)
Study participants
The global residents aged 15 years and older during the study time period were our participants, and the information on their age and gender was also obtained from the GBD 2021 study. 9 All the COPD patients recorded in the GBD study were defined as participants with outcome event in this study. These data sources used for estimating the burden of COPD were downloaded from the Global Health Data Exchange source (https://ghdx.healthdata.org/gbd-2021/data-input-sources) on request. Ethics approval was waived for the present study, as all data analyzed were de-identified and publicly available from GBD 2021 study.
Study variables and definitions
Outcome variable
The outcome variable referred to disease burden caused by COPD, which was specifically indicated with absolute numbers of incident cases, prevalent cases, deaths and DALYs, and their age-standardized rates (ASRs) per 100,000 individuals per year. DALY referred to the sum of years lost due to premature death and years lived with disability.9,15 One DALY represents one year loss in full health.9,15 In GBD 2021, COPD was determined using forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) based on post-bronchodilator spirometry test. 16 A person with the value of FEV1/FVC< 0.7 was defined as a COPD patient. 16 Additionally, COPD cases were recorded with International Classification of diseases (ICD) codes: 491-492 and 496 from ICD-9, or J41-J44 and J47 from ICD-10.9,17
Explanatory variable
The explanatory variables included socio-demographic index (SDI), sex, age, country and geographic region. Participants were categorized as men or women. Because GBD studies recorded data just for those aged 15+ years, participants were then categorized into 17 age-groups with a 5-year interval in the analysis. Age-specific rates (the crude rate of each metric within 5-year age groups) were examined to demonstrate the trend in COPD burden in age-strata. Countries and geographic regions were, respectively, adopted directly from the official list of country and the classification of geographical region by WHO (Table S1).
SDI is a widely-used community-level composite indicator, which comprises income per capita, mean years of schooling over the age of 15 years and the fertility rate. 18 It ranges from 0 to 1, with higher values indicating greater development of a community. 18 WHO classified the 204 countries and territories into five quintiles based on SDI value (Table S2).
Statistical analysis
Firstly, we described the epidemiological distribution of COPD by sex, age, region and country. Then, with Joinpoint software (version 5.0.2), annual percent change (APC) and average annual percent change (AAPC) were calculated to investigate the periodical and total trends in ASR of COPD over the past 22 years, respectively. The statistical significance of trend fluctuations was assessed by comparing the APC or AAPC to zero. Additionally, to examine the effect of SDI on AAPC of COPD, the Spearman rank order correlation method was used. 19 All results were treated as statistically significant at p value < 0.05.
Next, we predicted the incident cases, prevalent cases, deaths and DALYs’ number as well as the corresponding ASRs of COPD from 2022 to 2030 based on Bayesian age-period-cohort (BAPC) model, which was constructed under the integrated nested Laplace approximations (INLA) framework using “BAPC” package with R software. The BAPC model with INLA has an outstanding performance of prediction.20,21 Briefly, the age-period-cohort model estimated the outcome variables based on a log-linear model with cumulative effects of age, period and cohort.21,22 Then, since the cumulative effects in adjacent periods might be similar, posterior distribution could be estimated by Bayesian inference nested Laplace approximations. 21
Finally, a decomposition analysis was conducted to disentangle the total change in the incident cases, prevalent cases, deaths and DALYs of COPD into aging, population growth, and epidemiological change.23,24 Epidemiological change refers to the combined contributions of all factors other than aging and population growth in the study. 24
Results
Global burden of COPD from 2000 to 2021 and the projection until 2030
Figure 1 and Table S3 presents the global burden of COPD from 2000 to 2021. Increasing trends were examined in crude numbers of incident cases, prevalent cases, deaths and DALYs of COPD from 2000 to 2021, whereas decreasing trends were observed in ASRs, with corresponding AAPCs (95%CI) of -0.15 (-0.18, -0.12), -0.13 (-0.16, -0.11), -1.74 (-1.96, -1.53) and -1.65 (-1.76, -1.55), respectively, worldwide. Similar scenarios of trends in numbers and ASRs were identified for men and women, separately. Interestingly, the increase in numbers of incident cases and prevalent cases was higher in women than men, with women’s totals surpassing men’s by 2021. The decrease in ASRs was contributed mainly by men, but the ASRs were higher in men than women in 2000 and 2021. Number and age-standardized rate of incident and prevalent cases, deaths and DALYs for COPD by sex from 2000 to 2021. (A) Number of incident cases, prevalent cases, deaths and DALYs and age-standardized rate of incidence, prevalence, deaths and DALYs in males; (B) Number of incident cases, prevalent cases, deaths and DALYs and age-standardized rate of incidence, prevalence, deaths and DALYs in females. DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease.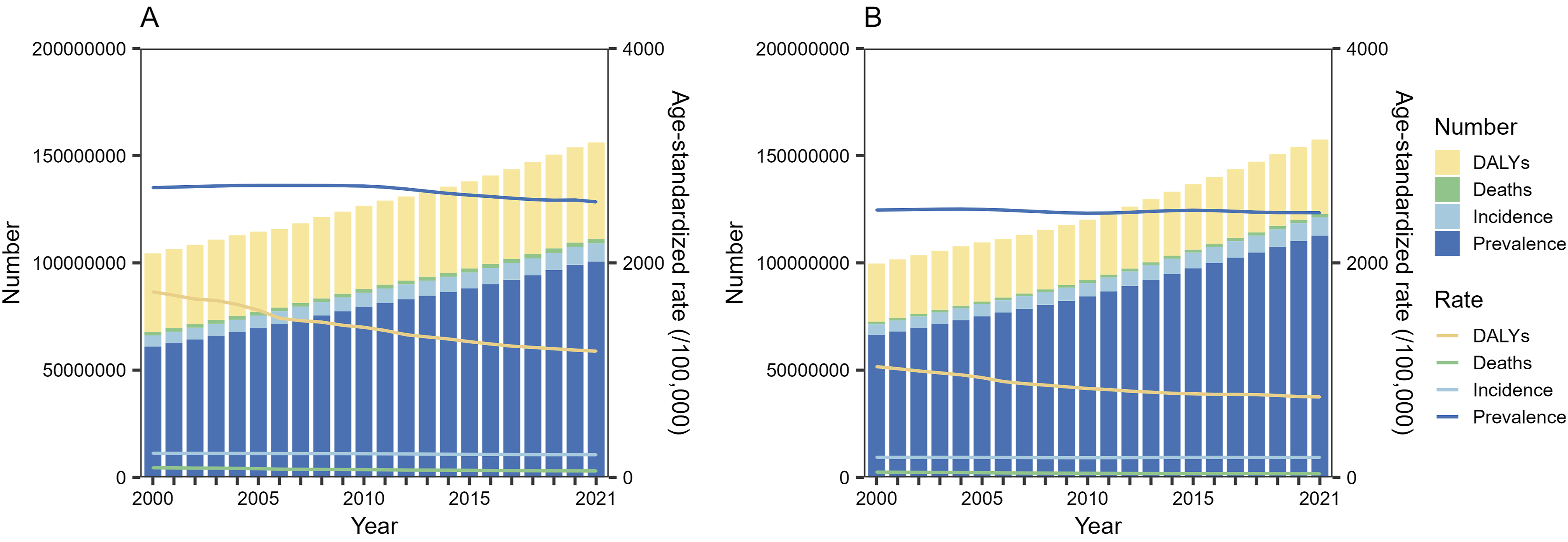
Figure 2 shows COPD burden by age. The highest number of incident cases, prevalent cases and DALYs of COPD was found in the age-group of 70-74 years in either 2000 or 2021. However, the highest death number of COPD was examined in population aged 75-79 years in 2000 and those aged 80-84 years in 2021. Age-specific prevalence rate increased gradually with age in both 2000 and 2021. Moreover, an initially increasing and subsequently decreasing trend was identified in age-specific rate of incidence, mortality and DALYs, with the peak in those aged 90-94 years in 2000, while a gradually increasing trend was observed in 2021. Number and age-specific rate of incident and prevalent cases, deaths and DALYs for COPD by age groups in 2000 and 2021. (A) Number of incident cases, prevalent cases, deaths and DALYs and age-specific rate of incidence, prevalence, deaths and DALYs in 2000; (B) Number of incident cases, prevalent cases, deaths and DALYs and age-specific rate of incidence, prevalence, deaths and DALYs in 2021. DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease.
In the prediction analysis, the estimated ASRs of prevalence, incidence, deaths and DALYs would continue to decline until 2030 (Figure S1). Notably, the numbers of incident cases, prevalent cases, deaths and DALYs of COPD were projected to rise rapidly until 2030 (Figure S2).
Burden of COPD from 2000 to 2021 by SDI and geographical regions
Table S4 displays burden of COPD by SDI region in 2000 and 2021. Among the five SDI regions, increasing trends were observed in either the incident or prevalent case number of COPD from 2000 to 2021, with the greatest increase in the middle SDI region. The number of deaths and DALYs increased from 2000 to 2021 in all but the high-middle SDI region, with the greatest increase in the low-middle SDI region.
Interestingly, ASRs of COPD incidence and prevalence increased only in the low SDI region, while decreasing in all others (Figure 3). Moreover, declining trends were found in the ASRs of COPD deaths and DALYs within all the five SDI regions. The lowest AAPC of all ASRs was identified in the high-middle SDI region. Additionally, SDI was negatively correlated with AAPC for ASR of incidence (R = −0.25, p < 0.001), prevalence (R = −0.40, p < 0.001), deaths (R = −0.26, p < 0.001) or DALYs (R = −0.27, p < 0.001) worldwide (Figure 4). Trends in age-standardized rate of incidence, prevalence, deaths and DALYs for COPD in global and five SDI regions from 2000 to 2021. (A) Age-standardized rate of incidence; (B) Age-standardized rate of prevalence; (C) Age-standardized rate of deaths; (D) Age-standardized rate of DALYs. DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease; SDI, socio-demographic index; APC, annual percent change. *Indicates that the APC is significantly different from zero at the alpha = 0.05 level. The correlation between SDI and AAPC of age-standardized rate of incidence, prevalence, deaths and DALYs for COPD. (A) SDI and AAPC of age-standardized incidence rate; (B) SDI and AAPC of age-standardized prevalence rate; (C) SDI and AAPC of age-standardized deaths rate; (D) SDI and AAPC of age-standardized DALYs rate. Each dot represents one of the 204 countries used in the study. The R indicates correlation coefficient and p value is estimated using Spearman rank order correlation method. SDI, socio-demographic index; AAPC, average annual percent change; DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease.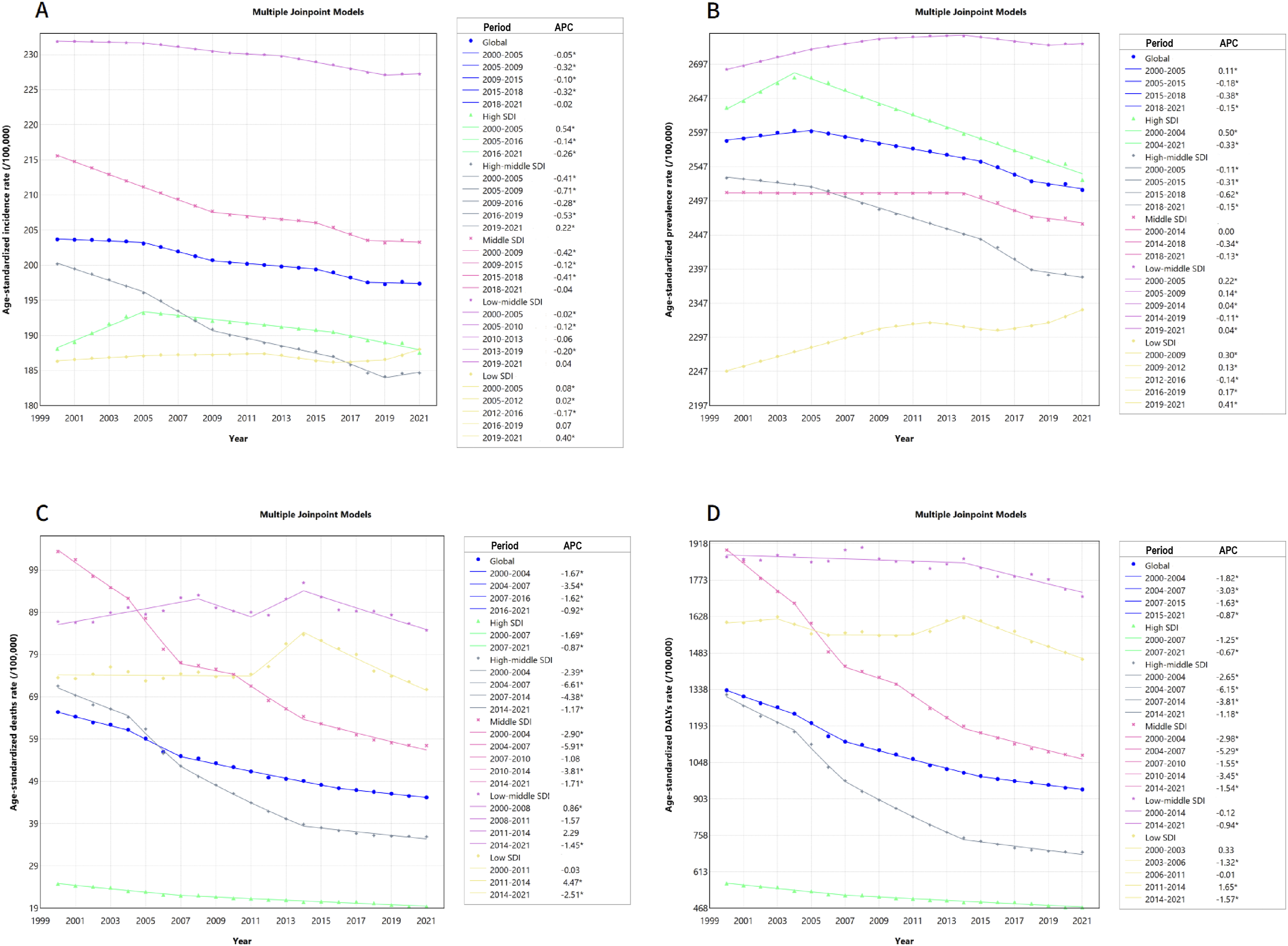
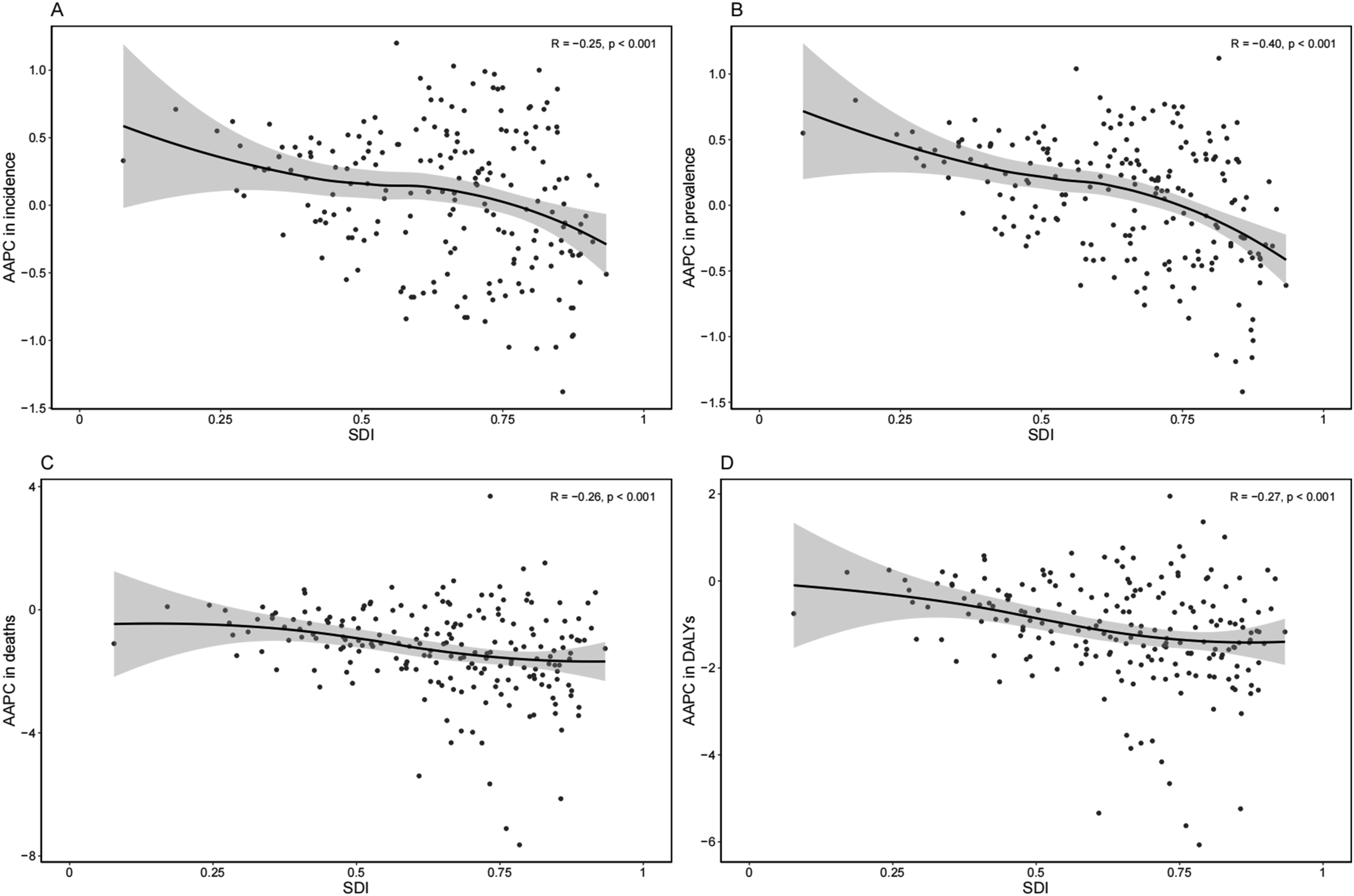
Table S5 demonstrates COPD burden by geographical region in 2000 and 2021. Both the numbers of incident and prevalent COPD case increased from 2000 to 2021 in all the 21 geographical regions. The peaks of increase were recorded in East Asia. For the ASRs of COPD incidence and prevalence, the highest AAPCs were, respectively, examined in North Africa and Middle East and Western Sub-Saharan Africa, but the lowest in Australasia. The number of deaths and DALYs increased separately in 18 and 19 regions over the past 22 years, with South Asia witnessing the greatest increase for both. Additionally, ASRs of deaths and DALYs decreased in all the 21 geographical regions. The lowest AAPC in ASRs of deaths and DALYs, separately, was observed in Eastern Europe and East Asia.
Burden of COPD from 2000 to 2021 by country/territory
Figure 5 and Table S6 illustrate the burden of COPD by country/territory in 2000 and 2021. At the national level, the top two ASRs of COPD incidence were recorded in Nepal (ASR = 310.58; 95%UI = 300.58, 319.70) and Papua New Guinea (ASR = 279.71; 95%UI = 263.93, 294.94) in 2021. In terms of ASR of prevalence, The United States of America ranked the top first (ASR = 3445.29; 95%UI = 3263.49, 3602.42), and followed by The United Kingdom (ASR = 3270.26; 95%UI = 2957.04, 3570.38). Additionally, the highest ASRs of both deaths (ASR = 156.82; 95%UI = 123.55, 197.43) and DALYs (ASR = 3004.36; 95%UI = 2404.29, 3732.82) were observed in Papua New Guinea in 2021. More details on analysis stratified by country/territory are available at the public repository Figshare (https://doi.org/10.6084/m9.figshare.28082135) for free and straightforward re-use. Age-standardized rate of incidence, prevalence, deaths and DALYs for COPD in 204 countries and territories in 2021. (A) Age-standardized rate of incidence; (B) Age-standardized rate of prevalence; (C) Age-standardized rate of deaths; (D) Age-standardized rate of DALYs. DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease; ASR: age-standardized rate.
Decomposition analysis of COPD from 2000 to 2021 at the global and regional levels
Figure 6 presents the decomposition analysis results concerning the total changes in incident cases, prevalent cases, deaths and DALYs of COPD contributed to population aging, population growth and changes of epidemiology at the global level and by SDI category. The increasing trends of COPD burden among total world population over the past 22 years could be explained primarily by aging and population growth. The similar scenario was observed for either men or women (Table S7). Changes in incident cases, prevalent cases, deaths and DALYs number of COPD according to three population-level determinants and by SDI from 2000 to 2021. The total change was decomposed by population aging, epidemiological change and population growth, with the number in 2000 as the reference for each year. DALYs: disability-adjusted life-years; COPD: chronic obstructive pulmonary disease; SDI: socio-demographic index.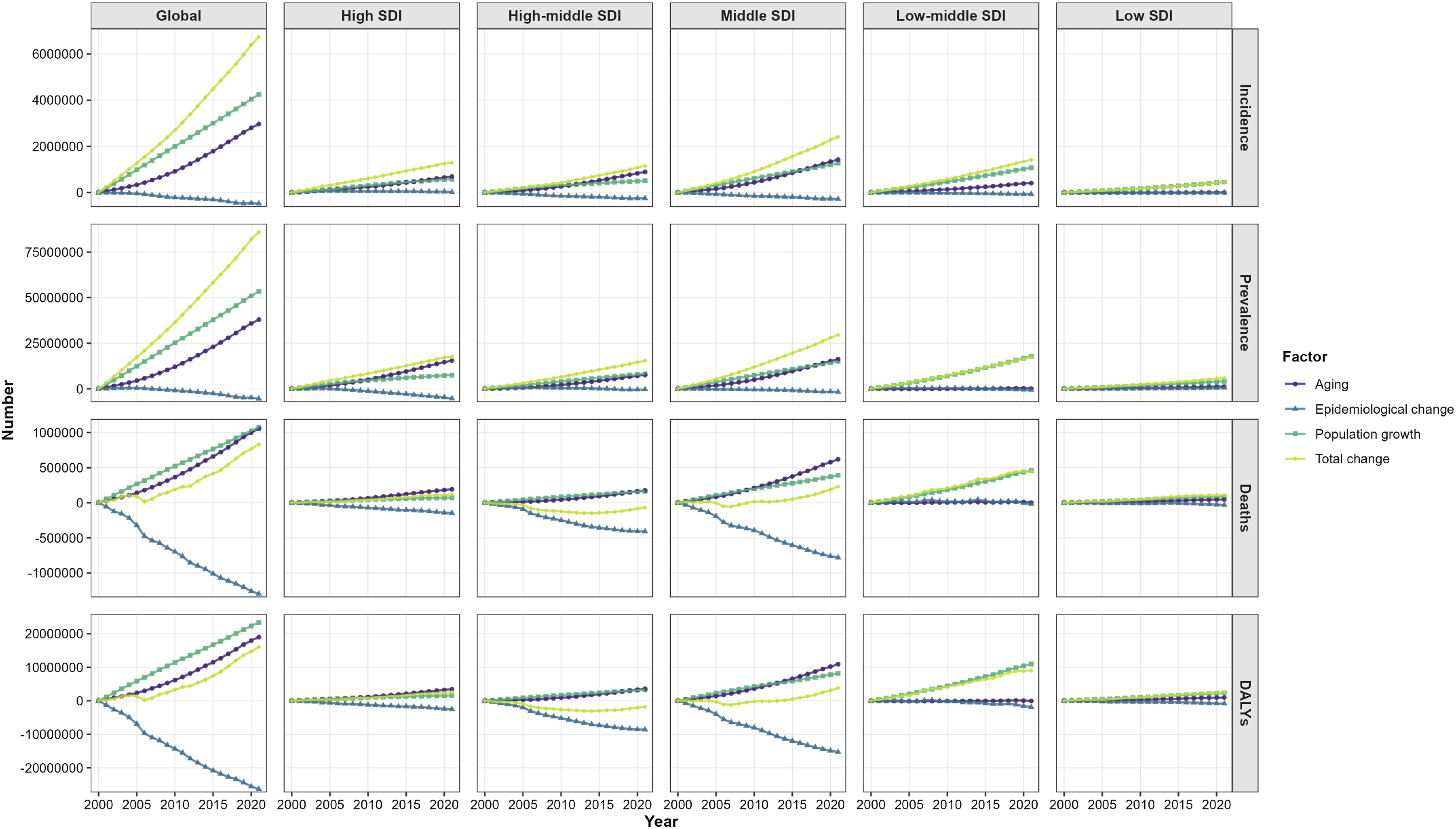
By SDI category, the largest increases in both COPD incident and prevalent cases from 2000 to 2021 were found in the middle SDI region, driven mainly by population aging and growth. Moreover, the greatest increases in COPD deaths and DALYs occurred in the low-middle SDI region, primarily resulting from rapid population growth. Only the high-middle SDI region witnessed a decline in total COPD deaths and DALYs with decreasing epidemiological changes over the time period. Compared to 2000, population aging and growth contributed more significantly to the COPD burden in all five SDI regions by 2021, whereas the contribution of epidemiological changes declined.
For geographical regions, the largest increases in COPD incident and prevalent cases from 2000 to 2021 were observed consistently in East Asia, driven largely by aging (Table S7). Moreover, the largest increases in COPD deaths and DALYs from 2000 to 2021 occurred in South Asia, driven largely by population growth and aging. Decreases in COPD deaths and DALYs were found in Eastern Europe, which were mainly due to the decreasing population growth and epidemiological change over the time period.
Discussion
Based on GBD 2021 data, increasing trends were observed for COPD in crude incident cases, prevalent cases, deaths and DALYs from 2000 to 2021 globally, with majority of the increases in incident cases and prevalent cases contributed by women. After consideration of population growth and aging over the time period, decreasing trends were examined in ASRs worldwide. Moreover, such a declining trend would be expected to continue until 2030.
The absolute numbers of incident cases, prevalent cases, deaths and DALYs for COPD were projected to rise worldwide by 2030 in this study, which was in line with those reported in previous studies.25,26 The increasing COPD burden was likely due to that the increased effect of population growth and aging substantially surpassed the reverse effect of epidemiological changes, as per the decomposition analysis. Additionally, this was also supported by long-term trends of expanding global population size alongside a marked increase in the proportion and number of older adults.27,28 On the other hand, the decreasing trend in age-standardized COPD burden might be explained by population-level control of the risk factors and advanced technologies of symptomatic treatment for the patients over the past decades. 25
Age-specific rates of COPD incidence, prevalence, mortality and DALYs substantially increased with age. Physiologically, lung function, such as lung elasticity, respiratory muscle strength and chest wall compliance, will reduce gradually with age. 29 The lung has unique susceptibility to environmental factors such as smoking and air pollution, and long-term exposure to these risk factors usually leads to diverse lung pathologies.30,31 Thus, rapid industrialization and urbanization in developing countries over the past decades increased COPD risk.32–34 Additionally, COPD is associated with many comorbidities, which increases the risk of death for older people with COPD. 35 Given an accelerated process of aging nowadays, attention on tackling the development and progression of COPD should be paid particularly to older individuals.
Moreover, ASRs of COPD were higher in men than women in 2000 and 2021. Such a sex disparity might be explained by differential exposure to occupational pollution and smoking.36,37 However, the numbers of incident and prevalent COPD cases were observed increasing more rapidly among women than men, with women’s totals surpassing men’s by 2021. This sex disparity might be due to that women had increasing exposure to passive smoking and/or indoor air pollution, such as biomass from cooking and heating.38,39 Meanwhile, female smokers showed greater susceptibility to airflow obstruction than males. 40
At geographical region level, the highest increase in ASRs of COPD incidence and prevalence was, respectively, found in North Africa and Middle East and Western Sub-Saharan Africa, while the ASRs of deaths and DALYs were identified decreasing in all the 21 geographical regions. These could be explained by the relatively high exposure to biomass fuels and smoking, and the long-term impact of some communicable diseases (e.g. HIV/AIDS) in Africa, and increasing attentions paid to early diagnosis and treatment of COPD worldwide.16,41,42
When data were analyzed by SDI region, the crude COPD burden increased from 2000 to 2021 in all SDI regions, with an exception of deaths and DALYs numbers in the high-middle SDI region. Meanwhile, all SDI regions witnessed decreasing trends in the ASRs, with an exception of ASRs of incidence and prevalence in the low SDI region. At the national level, Papua New Guinea and Nepal, from the low SDI region, had the highest ASRs of COPD incidence, deaths, and DALYs. These findings suggested that the majority of global COPD burden was produced by LMICs, which was consistent with prior studies.43,44 This scenario might be explained by the following reasons. Firstly, LMICs tended to witness the risk factors of COPD, including smoking, air pollution, inadequate healthcare access, and rapid population aging.45–47 For example, LMICs accounted for approximately 80% of the world’s smoking-related deaths. 48 Additionally, in LMICs, policy priorities and limited healthcare resources were still placed on prevention and treatment of infectious diseases, which implies comparatively less focus on non-communicable diseases. 49 Finally, explosive population growth in regions like sub-Saharan Africa has outpaced the development of healthcare systems and other COPD mitigation measures.43,50 Thus, tackling COPD poses a significant and growing challenge to health systems in these regions. LMICs need to intensify efforts by engaging physicians and other healthcare workers to raise awareness for both patients and providers, to use standardized diagnosis and management, and to improve the availability of inhalation therapies for COPD patients.
This is the first study to systematically assess the burden of and its trend in COPD from 2000 to 2021 at the global, regional and country level, and further make a prediction until 2030 using GBD 2021 data. However, there were some limitations. Firstly, as the second-hand data from GBD study used in our study, the bias regarding GBD study also existed in the present one. For example, COPD might be misclassified due to poor healthcare access and different diagnosis criteria, particularly in lower SDI regions. 51 Secondly, the GBD dataset provided estimates on diseases/injuries based on mathematical modelling. Those modelled estimates for data-sparse regions relied particularly on COPD-associated covariates and trends in neighbor countries/societies,9,15 which implied potential inaccuracy of the estimates. Thirdly, it is notable that the projections of COPD burden until 2030 were based on pre-COVID-19 data and might not explicitly account for the potential long-term effects of the pandemic on COPD burden. Thus, it is necessary and meaningful to make comparison between the estimates projected using pre-COVID-19 data and the post-pandemic real-world COPD burden in future. Fourthly, only participants aged 15 years and older were included in the analysis, which might not capture congenital cases under 15 years older, thereby implying potential under-estimate of COPD cases. Fifthly, GBD study collected data only at population-based level, which could not allow us to make further analysis on individual-level differences. Lastly, limited risk factor data in the GBD study restricted our analysis to the effects of population growth, aging, and epidemiological change on COPD trends, rather than identifying more specific contributing factors.
In conclusion, the crude number of incident cases, prevalent cases, deaths and DALYs of COPD increased from 2000 to 2021 worldwide, and would continue to increase to 2030, mainly attributed to aging and population growth. However, a decreasing trend was observed in the ASRs of all COPD burden indicators. Further, men, older adults, or population residing in low SDI regions bore substantial burdens of COPD. These findings underscore the need for precision public health interventions tailored to age, sex, geographic location, and socioeconomic status to effectively combat COPD.
Supplemental material
Supplemental Material - Global, regional and national trends in burden of chronic obstructive pulmonary disease from 2000 to 2021 and the prediction for 2030
Supplemental Material for Global, regional and national trends in burden of chronic obstructive pulmonary disease from 2000 to 2021 and the prediction for 2030 by Jian Xu, Huiqing Xu, Dandan Zhang, Xiaojing Deng, Yeping Bian, Yunting Xu, Guofeng Ao, Jiannan Liu and Fei Xu in Chronic Respiratory Disease.
Footnotes
Acknowledgments
The authors thank all staff for their contributions to the GBD database.
Ethical considerations
All data analyzed in the study were publicly available and de-identified. Therefore, ethics approval was waived for this study. The methods performed in the study were in line with recommendations by the Declaration of Helsinki.
Author contributions
JL and FX conceived, designed and supervised the study. JX, HX and ZD were responsible for data acquisition. HX was responsible for data analysis. JX, HX, DZ, XD, YB, YX, GA, JL and FX wrote and critically reviewed the manuscript. Each author approved the final version for submission and was also responsible for all aspects of the work presented in this manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received support from Jiangsu Province Chinese Medical Science and Technique Development Foundation (QN202223, recipient: DZ).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data underlying the results of this study have been deposited on figshare (![]() ).
52
).
52
Role of the funder/sponsor
The funder had no role in this work and the decision of submission.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.