
Abstract
The aim of this article is to investigate which global initiative for chronic obstructive lung disease (GOLD) classification (B-C-D or II-III-IV) better reflects the functionality of patients with moderate to very severe chronic obstructive pulmonary disease (COPD). Ninety patients with COPD were classified according to the GOLD B-C-D and II-III-IV classifications. Functionality was assessed by different outcomes: 6-min walk test (6MWT), activities of daily living (ADL) (London Chest ADL Scale), and daily life activity/inactivity variables assessed by activity monitoring (SenseWear armband, Pittsburgh, Pennsylvania, USA). The 6MWT was the only outcome significantly associated with both the GOLD classifications. Good functionality as assessed by the 6MWT was observed in 80%, 69%, and 43.5% (GOLD B, C, and D, respectively) and 81%, 59%, and 29% (GOLD II, III, and IV, respectively) of the patients. Association (V Cramer’s) and correlation (Spearman) coefficients of 6MWT with GOLD B-C-D and II-III-IV were V = 0.30, r = −0.35, and V = 0.37, r = −0.25, respectively. Neither GOLD classification showed V or r ≥ 0.30 with any other functionality outcome. Both the GOLD B-C-D and II-III-IV classifications do not reflect well COPD patients’ functionality. Despite low association and correlation coefficients in general, both GOLD classifications were better associated with functional exercise capacity (6MWT) than with subjectively assessed ADL and objectively assessed outcomes of physical activity/inactivity.
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the major causes of morbidity and mortality in the world, 1 and there is increasing evidence showing that there is large heterogeneity within patients’ characteristics. 2 –4 Because of this marked COPD heterogeneity in terms of clinical outcomes, disease severity and progression, the 2011 update of the global initiative for chronic obstructive lung disease (GOLD) 5 proposed a multidimensional clinical evaluation that classifies patients into one of four groups (A, B, C, and D) according to exacerbation history, level of symptoms, and severity of airflow obstruction. This was in contrast with the traditional unidimensional GOLD classification (I, II, III, and IV), which takes into account only the severity of airflow obstruction. 6
The GOLD classification was developed to reflect disease severity, its impact on patient’s health status and the risk of future events (such as exacerbations, hospital admissions or death) in order to help guiding therapy of patients with COPD. 7 A number of recent studies have investigated the association between the multidimensional GOLD A-B-C-D classification and health outcomes 8 –14 as well as compared the traditional GOLD classification with the new multidimensional GOLD classification concerning hospitalizations, 11 mortality, 11 –13 and health-related quality of life (HRQOL). 14 These studies demonstrated that the unidimensional and multidimensional GOLD classifications do not differ significantly in terms of ability to predict hospitalization and mortality, except for HRQOL in which GOLD A-B-C-D is more closely associated with this outcome than GOLD I-II-III-IV due to the nature of the A-B-C-D classification involving a measure of HRQOL. Concerning the unidimensional GOLD classification, it is known that the forced expiratory volume in the first second, on which the classification is based, is not strongly associated with physical activity level. 15 However, it remains unknown whether the multidimensional GOLD classification correlates with functionality indicators such as functional exercise capacity, activities of daily living (ADLs) (self-reported limitations during day-to-day activities) and physical ADL (quantification of the amount of activities performed). Taking this into account, it is expected that the functionality will be better associated with multidimensional index than the unidimensional index. For this reason, it is interesting to know whether these two GOLD classifications reflect differently the functionality of patients with COPD.
The objectives of this study were to investigate the association of different functionality outcomes with the new multidimensional GOLD B-C-D groups, and to identify which GOLD classification (II-III-IV or B-C-D) better reflects the functionality of patients with COPD.
Methods
Subjects
All patients taking part in this study were recruited from the initial assessment for admission to the Pulmonary Rehabilitation Program at the University Hospital of Londrina, Universidade Estadual de Londrina (Brazil). No patient had already started the rehabilitation program by the time of his/her data collection. Data were collected from July 2006 to February 2014. This study was approved by the ethics committee of Universidade Estadual de Londrina (Brazil) and all patients gave written informed consent.
The diagnosis of COPD was established according to the current GOLD criteria. 16 In addition to the diagnosis, patients’ inclusion criteria were: clinical stability (i.e., no infection or exacerbation for at least the 12 previous weeks) and absence of severe or unstable heart disease or any other comorbidities that might influence the performance of the assessments. Participants were be excluded if they were unable to understand or perform any assessment procedure or if they wanted to leave the study for any reason.
Participants were classified according to the traditional unidimensional GOLD classification (based on the forced expiratory volume in the first second (FEV1) in percentage of the predicted values) from moderate to very severe stage (GOLD II-III-IV) as well as according to the new multidimensional GOLD classification from group B to group D (GOLD B-C-D). The number of patients classified as GOLD I and GOLD A assessed during the data collection period was too small to include these patients in the statistical analysis. The study was approved by the institution’s Ethics in Research Committee and all patients gave their written informed consent to participate.
Assessments
Lung function
Pre and postbronchodilator spirometry was performed following the American Thoracic Society/European Respiratory Society guidelines 17 by using the SpirobankG® spirometer (MIR, Italy). Brazilian reference values were used. 18
Symptoms and exacerbations
Symptoms and exacerbation history were assessed for the GOLD B-C-D classification. Dyspnea during daily life was assessed using the modified Medical Research Council (mMRC) scale that describes five grades of breathlessness ranging from 0 to 4. The low or high-symptom burden of the GOLD B-C-D was based only on the mMRC scores (<2 or ≥2, respectively) 5 since the COPD assessment test (CAT) questionnaire was not applied in this sample of patients.
The history of exacerbations was retrospectively recorded from the year before inclusion in the study. Exacerbation was defined as an acute event characterized by a sustained worsening of the patient’s condition, from the stable state beyond normal day-to-day variations, and leading to change in regular medication. 19 The individual patient’s history of two or more exacerbations in the preceding year indicated high risk, whereas less than two exacerbations indicated low risk. 5
Functional exercise capacity
Functional exercise capacity was assessed by the 6-min walk test (6MWT), which was performed twice in a 30-m corridor, with a resting period between tests of at least 30 min, according to international standards. 20 Patients were instructed to walk as fast as they can during 6 min and the best of the two walks was used for analysis.
Moreover, for the classification of functionality, two groups were formed according to the walked distance in percentage of predicted values: ≥80% of the predicted was considered as better functionality and <80% of the predicted as worse functionality. 21 The reference values used were those by Britto et al. 22 for Brazilian subjects.
Activities of daily living
Self-reported limitations during ADL were assessed using the London Chest ADL (LCADL) scale, which is a short disease-specific scale with 15 items divided into four domains: self-care (four items), domestic (six items), physical (two items), and leisure (three items). 23,24 This scale is used to grade how intensely dyspnea (and consequently the disease) impairs the performance of various ADL in a Likert-type scale of 0–5 points per item. A total score ranging from 0 to 75 is calculated by summing the domains, with higher values indicating more marked limitation in ADL.
A LCADL total score higher than 22 was considered as indicative of a limited level of ADL performance according to Vilaro et al. 25 Therefore, in this study, a total score of ≤22 was considered as better functionality and >22 as worse functionality.
Physical (in)activity in daily life
Physical (in)activity in daily life (PADL) was assessed by wearing the SenseWear Armband monitor. All subjects were instructed to use the monitor for two consecutive week days, 26 during 12 h/day (from the moment the patient wakes up until 12 h after that), and the average of the 2 days was used for analysis.
Patients were classified as physically active (better functionality) or inactive (worse functionality) according to achieving or not more than 80 min/day of nonbouts moderate intensity activities as described by van Remoortel et al. 27 Moderate physical activity intensity was considered as activities above the threshold of three metabolic equivalents of task (MET). 28
In addition to physical activity, sedentary behavior (i.e., physical inactivity) was also analyzed in terms of time spent per day below a certain MET threshold criteria (<3 MET) that was denominated as inactive time per day in this study. To calculate the inactive time per day, we considered the total assessment time (12 h) minus the time spent on moderate, vigorous, and very vigorous activities. The median of inactive time per day was calculated in order to classify the patients into two functionality groups: better functionality (below the median) and worse functionality (above the median).
Statistical analysis
The softwares used for data analysis were Statistical Package for the Social Sciences Version 20.0 and GraphPad Prism Version 3.01. Normality in data distribution was checked with the Shapiro–Wilk test. Data were expressed as mean ± SD or median (interquartile range 25–75%).
To investigate the association between functionality variables and GOLD classifications, the Chi-square test and the Cramer’s V coefficient were used to identify the strength of association. The Cramer’s V ranges between 0 and 1, and in the context of this study, higher values are indicative of stronger relationship between functionality outcomes and GOLD classification, whereas lower values indicate weaker relationship. The Spearman correlation coefficient was also used to analyze the association between functionality outcomes and GOLD classifications. The level of significance was set at p < 0.05.
Results
Demographic and clinical characteristics of the 90 patients included in the study are shown in Table 1. According to the new GOLD B-C-D classification, the majority of patients was classified in group D (68%), whereas according to the traditional GOLD II-III-IV classification the majority of patients was classified as grade III (51%).
Clinical characteristics and demographics of the sample (n = 90).a
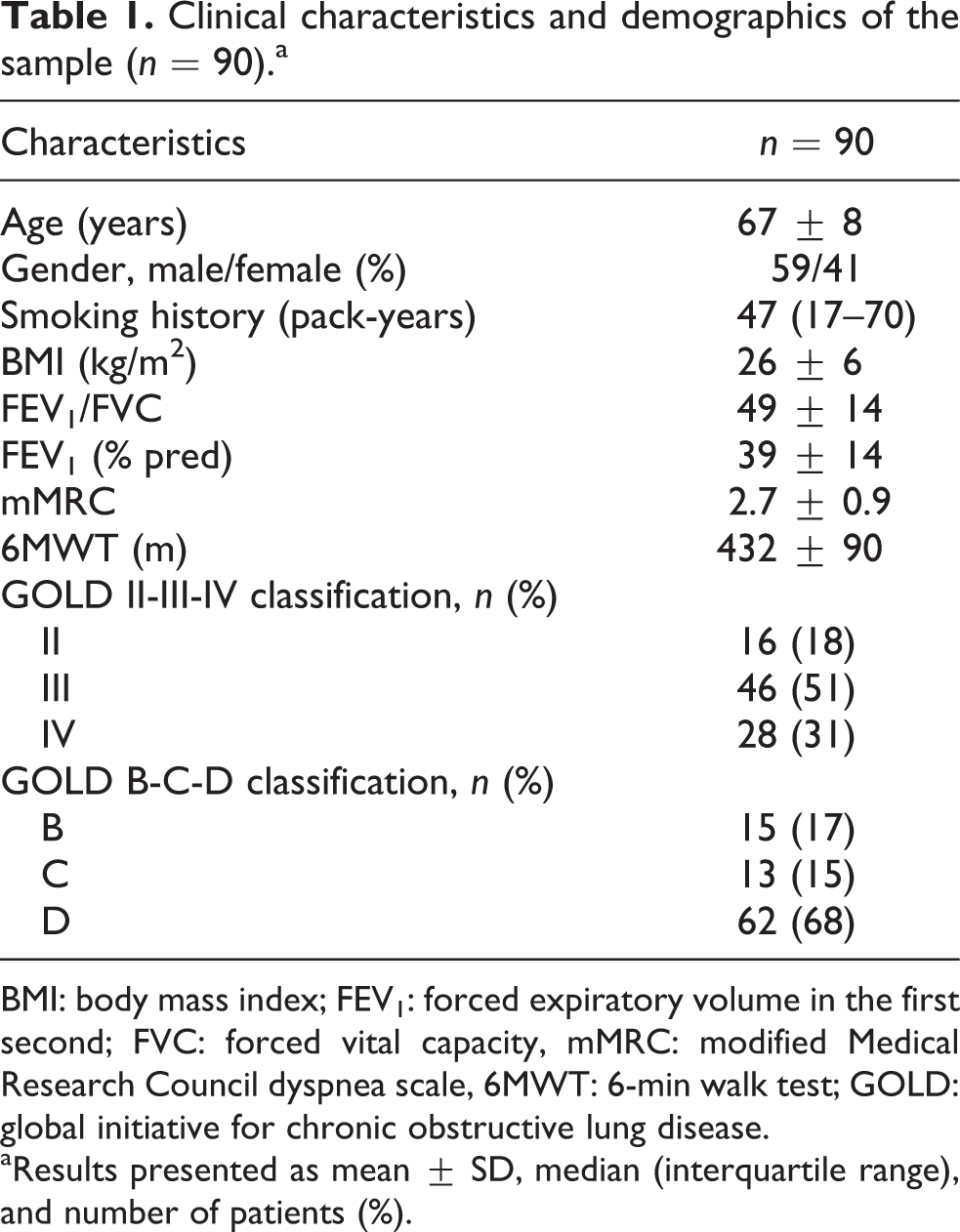
BMI: body mass index; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity, mMRC: modified Medical Research Council dyspnea scale, 6MWT: 6-min walk test; GOLD: global initiative for chronic obstructive lung disease.
aResults presented as mean ± SD, median (interquartile range), and number of patients (%).
Tables 2 and 3 show the distribution of patients’ functionality outcomes according to the multidimensional B-C-D and unidimensional II-III-IV GOLD classifications, respectively, as well as their association with functionality outcomes. Functional exercise capacity assessed by 6MWT (in percentage of the predicted values) was the only functionality outcome significantly associated with the multidimensional and unidimensional classifications. However, in general, the value of V Cramer’s coefficient was low (Tables 2 and 3), indicating weak associations between both GOLD classifications and 6MWT, and even weaker with the other functionality outcomes. Comparison of the 6MWT results among multidimensional GOLD groups showed shorter distances when comparing group D versus B and C, both for absolute values (p = 0.003) and for results in percentage of the predicted value (p = 0.005). Concerning the unidimensional GOLD, similar results were observed for group IV versus II and III in percentage of the predicted values, with a strong trend for results in absolute values as well (Figure 1).
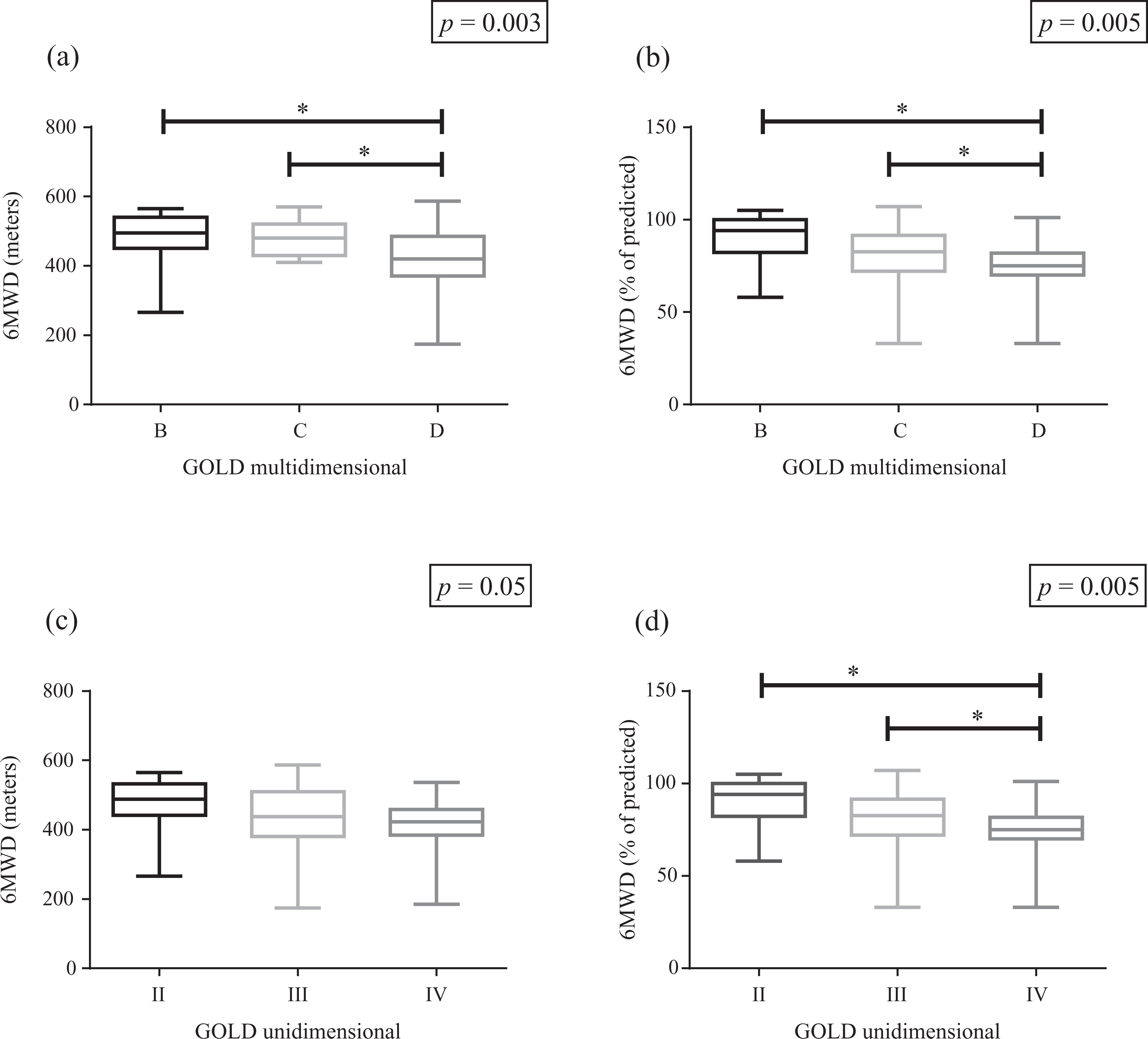
Comparison of 6MWT results in patients classified according to the GOLD multidimensional index (a and b) and the GOLD unidimensional index (c and d) (both in meters (left panels) and in percentage of the predicted values (right panels)). 6MWT: 6-min walk test; GOLD: global initiative for chronic obstructive lung disease. *p < 0.05.
Distribution of patients’ functionality outcomes and association with the new GOLD B-C-D classification.

Results presented as number of patients (%).
6MWT: 6-min walk test; PADL: physical activity in daily life; MET: metabolic equivalent of task; LCADL: London Chest Activity of Daily Living scale; GOLD: global initiative for chronic obstructive lung disease.
Distribution of patients’ functionality outcomes and association with the GOLD II-III-IV classification.a

aResults presented as: number of patients (%).
6MWT: 6-min walk test; PADL: physical activity in daily life; MET: metabolic equivalent of task; LCADL: London Chest Activity of Daily Living scale; GOLD: global initiative for chronic obstructive lung disease.
When comparing the median values of physical activity or inactivity outcomes among different patient groups (B vs. C vs. D and II vs. III vs. IV), there were no significant differences in active or inactive time (Table 4). A further analysis was performed with two MET as the threshold for inactivity instead of three MET, and results were similar.
Comparison of active or inactive time (in minutes) in patients with COPD classified according GOLD B-C-D and GOLD II-III-IV.
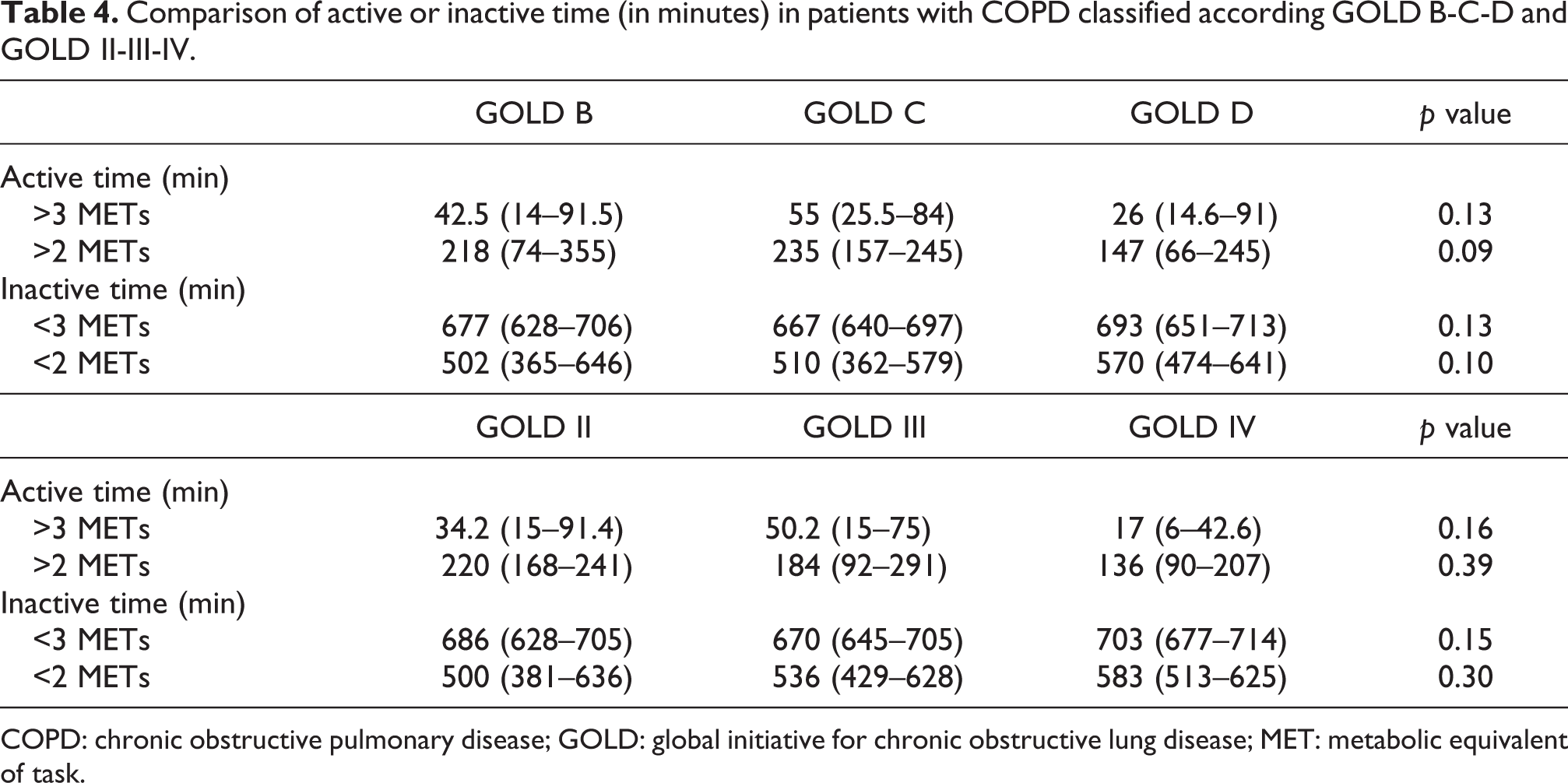
COPD: chronic obstructive pulmonary disease; GOLD: global initiative for chronic obstructive lung disease; MET: metabolic equivalent of task.
Spearman coefficients showed that the B-C-D and II-III-IV GOLD classifications were weakly but significantly correlated with the 6MWT (r = −0.43 and −0.41, respectively; p < 0.001 for both). Furthermore, the LCADL total score showed a statistically significant but even weaker correlation only with the GOLD B-C-D classification (r = 0.26, p = 0.01) and no correlation with the GOLD II-III-IV classification (r = 0.04; p = 0.68). For the PADL activity and inactivity variables, no correlation was found with either GOLD classifications: for activity, r = −0.18 (p = 0.08) with both classifications; and for inactivity, r = 0.17 (p = 0.1) with the B-C-D classification and r = 0.19 (p = 0.07) with the II-III-IV classification.
Discussion
Regarding the functionality outcomes assessed in this sample of patients with COPD, only the 6MWT was associated with the new GOLD B-C-D classification as well as with the traditional GOLD II-III-IV classification. However, the association was weak suggesting that the combined assessment proposal (A-B-C-D) does not reflect well the functionality of patients with moderate to very severe COPD, similarly to the unidimensional assessment based only on the FEV1. Additionally, we found differences in the 6MWT between the severe groups (D and IV) in comparison to the less severe classifications (B, C and II, III).
Dyspnea sensation, exacerbation frequency, and FEV1 are well-known risk factors for poor prognosis in patients with COPD. 29 Despite this, some studies have shown that the combination of these three components that compose the multidimensional GOLD A-B-C-D classification is not different from the unidimensional classification to predict long-term COPD outcomes such as hospitalization 11 and mortality. 11 –13 The same was observed in this cross-sectional study concerning functionality of patients with COPD, the results of which are in agreement with these studies. It is interesting that even the new GOLD A-B-C-D classification, which considers aspects other than airflow limitation alone, does not reflect well COPD patients’ functionality. Therefore, according to the previous literature and the present results, the multidimensional GOLD index may be superior to the unidimensional GOLD classification for staging the disease and for guiding individualized management, but not for reflecting functionality. Hence, the usefulness of the multidimensional GOLD classification in clinical practice remains unclear in some points and more data with this proposed approach are needed.
It is known that the use of different tools to evaluate symptoms (mMRC versus health status with CAT or clinical COPD questionnaire) significantly influences the grading assignment in the multidimensional GOLD. 30 In this study, only the mMRC was used. The new GOLD strategy recommends that is it not necessary to use more than one of these self-reported tools for symptom evaluation. However, this is not supported by strong scientific evidence and it is still unclear whether they can be used interchangeably.
The only statistically significant association of both GOLD classifications with the functionality outcomes proposed in this study was with functional exercise capacity, and a weak one. Nishimura et al. 31 found significant correlations between the new GOLD A-B-C-D classification with maximal exercise capacity evaluated by the peak volume of oxygen intake (VO2), as well as with the modified BODE index. However, the authors did not present the correlation coefficient values and only highlighted that the peak VO2 was stratified by the new GOLD classification, showing a severity gradient from GOLD A to GOLD D, although no difference between groups B and C was observed. In this study, when analyzing the functionality assessed by the median of 6MWT (expressed as percentage of predicted values) between groups B-C-D and grades II-III-IV, both classifications discriminated group D from B and C and grade 4 from 3 and 2, without significant differences among the other groups. A study which compared the two GOLD classifications concerning HRQOL and health costs concluded that the multidimensional GOLD classification had better discriminative capacity than the unidimensional GOLD classification 14 ; on the other hand, this study concluded that this does not apply to patients’ functionality.
The absence of association between the new GOLD classification and PADL can possibly be related to the fact that daily physical activity involves a complex interaction affected not only by physical components but also by psychosocial, personal, and environmental factors 32,33 which are beyond the scope of the GOLD classification. Additionally, data from a systematic review showed that association between physical activity and clinical outcomes such as FEV1 and dyspnea were lacking consistency and quality of evidence, which was rated as low to very low. 34 Therefore, the multidimensional GOLD A-B-C-D classification, as already demonstrated for the unidimensional I-II-III-IV classification, 15 is not a proper way to reflect the level of PADL in patients with COPD, as well as functionality of these patients in a broader sense.
Scientific attention has also been recently given to sedentary behavior or physical inactivity, 35 and therefore inactive time per day was also included among the outcomes proposed to assess and classify functionality in this study. However, results of inactivity were similar to those found for activity, that is, no association between inactive time and both GOLD classifications, what does not suggest advantage of an inactivity outcome over an activity outcome in the context of this study.
The relationship between LCADL total score and the multidimensional GOLD classification was weak and its association with the unidimensional classification was even less evident. The study describing the original development of the LCADL found no association between the scale and the FEV1, 23 whereas only a modest relationship between the two outcomes was observed in the validation study of the Portuguese LCADL version. 24 In addition, a study that investigated the association of different multidimensional indices with the LCADL showed that, among all multidimensional indices studied, only the SAFE index was an independent contributor to the self-reported limitations in ADL. 36 Although the LCADL is used to grade how intensely dyspnea impairs the performance of various ADL and the GOLD A-B-C-D classification involves the limitations due to dyspnea in daily life as assessed by mMRC scale, no association was found regarding the LCADL 22-points cut-off and a very weak association was found when considering the Spearman correlation coefficient (r = 0.26). Future studies can aim at investigating if the assessment of symptoms using the CAT questionnaire may find different results, since the CAT is an instrument which reflects more globally the health related quality of life of patients with COPD and can be considered as more comprehensive.
An interesting finding from this study is that the majority of patients had a 6MWD exceeding 80% of the predicted value, what appears to reflect a sample with well-preserved functional status. However, according to the previous literature, Brazilian patients with COPD present higher values of 6MWT when compared to European patients. 37 Furthermore, healthy Brazilian subjects present higher values of 6MWT when compared to patients from the United States and even from other countries in Latin America. 38 For this reason, we believe that this sample is indeed a reflection of the population studied.
As limitations of this study, the absence of patients in group A and grade 1 can be firstly mentioned. Because of the patient profile in our rehabilitation center, we did not have a reasonable number of patients in this group or grade, which made their analysis not feasible. Secondly, a previous study 39 showed that the choice of symptom assessment tool (mMRC or CAT) directly influences the category assignment in the GOLD A-B-C-D classification, suggesting that both tools could be applied and the higher value should be used to classify patients according to their level of symptoms. However, we did not collect data of the CAT in our sample, and therefore it is possible that we may have underestimated symptom severity for patients that were included in group C by using only mMRC scale. However, the ideal symptoms questionnaire and associated cut-points are still a matter of debate, and at this moment either of the two instruments can be used as recommended by the 2011 GOLD document. 5 Daylight time can be considered as a confounder of physical activity assessment; 26 however, these data were not available and therefore could not be taken into consideration in this study. Nevertheless, we believe that this fact does not hinder our results since the region where this study was developed presents nonmarked variations of daylight time throughout the year. And finally, in this study the history of exacerbations was self-reported and this may have underestimated the risk in case patients were classified as GOLD B, since exacerbation self-report by patients with COPD to health care professionals may not be optimal. 40
In conclusion, both the GOLD B-C-D and II-III-IV classifications do not reflect well patients’ functionality in a broad sense. Despite low association and correlation coefficients in general, both GOLD classifications were better associated with functional exercise capacity (6MWT) than with subjectively assessed ADL and objectively assessed outcomes of physical activity/inactivity. Future longitudinal studies can be performed to identify the impact of improving functionality on the distribution of the GOLD A-B-C-D groups.
Footnotes
Author note
Joint first authorship: Both authors contributed equally to the study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.