
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is a heterogeneous and chronic condition characterized by irreversible airflow obstruction. Health literacy may influence the use of complementary and alternative medicine (CAM). This study aims to investigate the role of health literacy in the use of CAM among COPD patients.
Methods
This cross-sectional study was conducted at Ankara University School of Medicine, Department of Chest Diseases, involving patients with COPD between August 2024 and June 2025. Clinical COPD Questionnaire (CCQ) and Health Literacy Scale-Short Form (HLS-SF) were used to assess disease severity and health literacy, respectively.
Results
Among 190 patients, inadequate and limited health literacy was more common among CAM users compared to non-users (n = 54/89, 61% vs n = 37/101, 37%, respectively, p = 0.007). CAM users were also more likely to have insufficient social support (n = 24/89, 25%, p = 0.047), cough (n = 79/89, 89%, p = 0.049), history of ICU admission (n = 19/89, 21%, p = 0.02), use of long-term oxygen therapy and noninvasive ventilation (n = 50/89, 56% p = <0.001; n = 26/89, 30%, p = <0.001, respectively), had higher rates of GOLD E classification (47/89, 55%, p = <0.001), and had higher median CCQ total scores as 2.78 [Interquantiler Range (IQR): 1.4-4.1, p = 0.002]. Inadequate and limited health literacy was significant predictors of CAM use (OR: 3.78; 95% CI: 1.25-11.4, p = 0.018; OR: 6.78, 95% CI: 1.63-28.0, p = 0.008, respectively), as well as GOLD E classification (OR: 2.71, 95% CI: 1.14-6.45, p = 0.024) and insufficient social support (OR: 2.56, 95% CI: 1.00-6.50, p = 0.048) after adjusting for age, sex, education, and comorbidities.
Discussion
This study revealed the association between COPD symptom severity and frequent exacerbation, insufficient social support, along with lower health literacy and the use of CAM.
Introduction
Chronic obstructive lung disease (COPD) is a heterogeneous lung disease characterized by airflow obstruction and consists of a major cause of morbidity with significant disability, and mortality. 1
Complementary and alternative medicine (CAM) is a collection of various medical and health systems, therapies, and products that are not currently recognized as part of conventional medicine. 2 The reports reveal that the frequency of the use of CAM increased over time, however, the prevalence and associated factors remain unclear. 3 Factors associated with the use of CAM could include patient education, disease severity, comorbidities, concerns about side effects, and potentially health literacy. Most of the existing studies on CAM use have focused on patients with asthma, rheumatologic conditions, or cancer, while evidence specific to COPD is still lacking.4,5 The existing evidence on CAM use in COPD management predominantly stems from studies highlighting the anti-inflammatory potential of herbal therapies rooted in Traditional Chinese Medicine. 6 Nonetheless, these approaches are generally absent from clinical guidelines, primarily because of methodological challenges in conducting randomized controlled trials on CAM therapies.
Health literacy refers to the extent to which individuals can acquire, interpret, and comprehend health information and services necessary for making informed health decisions and taking appropriate actions. 7 Conflicting evidence in the general population makes the interaction between health literacy and CAM difficult and potentially bidirectional. Studies conducted in different regions, from Iran to Australia, suggest that good health literacy supports CAM use by enabling better understanding and navigation of treatment alternatives.8,9 A previous study from Türkiye focusing on cancer patients revealed a potential association between low eHealth literacy and the use of CAM. 10 Another study reported an inverse relationship between health literacy and the use of CAM. 11
Studies have reported inadequate health literacy in a substantial proportion of patients, with prevalence reaching 64% in Türkiye. 12 A study conducted among COPD patients found a high prevalence of low health literacy, which was linked to illness beliefs that negatively influenced treatment adherence. 13 Previous studies have not directly examined the relationship between health literacy and the use of CAM among COPD patients. Türkiye presents a unique cultural and healthcare context where traditional remedies and CAM practices are commonly utilized, yet under-researched in COPD populations. Understanding this relationship could inform patient education strategies and improve individualized COPD management. This study aims to investigate the relationship between the health literacy and the use of CAM among COPD patients in Türkiye.
Material and methods
Study design and setting
This single-center cross-sectional study was conducted at the Ankara University School of Medicine, Department of Chest Diseases. COPD patients admitted to the clinic between August 2024 and June 2025 were enrolled in the study. The study was approved by ethics review boards at Ankara University School of Medicine. (2024/486, 2024000486-3) The study was performed according to the Declaration of Helsinki. All participants gave informed consent before participating in the study and completing the questionnaire.
Population
Patients over 40 years of age and diagnosed with COPD based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2024 criteria (post-bronchodilator FEV1/FVC <0.7) were included in the study. Severe cognitive impairment and inability to communicate were set as exclusion criteria (Figure 1). Study flow diagram for study participants.
Data collection and variables
Data were collected through a face-to-face interview using patient information. Various data such as comorbidities, exacerbation and hospitalization history, medical treatment, and spirometry, were obtained from the medical records.
Sociodemographic factors were evaluated as part of the study. Age was recorded in years, and sex was categorized as male or female. Marital status was documented as single, married or divorced. Place of residency categorized as urban or rural residency. Social support was assessed based on whether a person lives with a relative or has a caregiver present. Education level was classified into four categories: Illiterate, primary school, high school, or university and above. Occupation was categorized as unemployed, public sector worker, blue-collar worker, professional, or farmer. Income level was assessed by comparing income to expenses and was categorized as income less than expenses, income equal to expenses, or income greater than expenses.
Clinical factors were systematically evaluated. Smoking history was recorded in pack-years, and immunization status was documented. Immunisation data covered vaccinations for pneumococcus and influenza. Individuals were classified as having adequate immunisation if they had received both, and inadequate if only one had been administered. Symptoms such as cough, sputum production, and chest pain were assessed, alongside the modified Medical Research Council (mMRC) dyspnea scale. The duration of symptoms and disease was also recorded. The Charlson Comorbidity Index (CCI) was evaluated and classified as mild (1–2), moderate (3–4), or severe (5+). 14 COPD severity was evaluated based on GOLD staging according to FEV1 values, the number of acute exacerbations in the last year, the history of intensive care unit admission due to COPD exacerbation, and GOLD ABE classifications. Exacerbation is defined as “an event in the natural course of the disease characterized by a change in the patient’s baseline dyspnoea, cough, and/or sputum that is beyond normal day‐to‐day variations, is acute in onset, and may warrant a change in regular medication in a patient with underlying COPD”. 1 Spirometry results included Forced expiratory volume in 1 s (FEV1; mL and %predicted), Forced vital capacity (FVC; mL and %), and FEV1/FVC ratio (%). Treatment factors included the type of inhaler combination therapy, duration of therapy, and use of long-term oxygen therapy (LTOT) or non-invasive ventilation (NIV).
The use of CAM was assessed according to the criterion of having used at least one type of CAM to manage COPD symptoms. Participants were asked if they had used at least one type of CAM. The types of CAM classified according to National Center for Complementary and Integrative Health (NCCIH) Classification of CAM therapies as nutritional (special diets, dietary supplements, herbs), psychological (spiritual practices, breath therapy, yoga), and physical (massage, acupuncture, cupping therapy, leech therapy, ozone therapy, salt caves, hot springs/baths).15,16
Questionnaires
The Clinical COPD Questionnaire (CCQ) was used to assess the health status of the patients, with scores reported for total, symptom, functional, and mental health domains, and included the analysis as continuous variables. 17 Health literacy was assessed using the Health Literacy Scale Short Form (HLS-SF), which is based on a 4-point Likert scale. 18 The total score ranges from 0 to 50, with scores <25 indicating “inadequate” health literacy, 25-33 indicating “limited” health literacy, 33-42 indicating “adequate” health literacy, and >42 indicating “excellent” health literacy.15,19 Both forms have been validated in the Turkish population.20,21
Data management and quality
All data was entered into a secure, electronic database in Microsoft Excel, version 2021 program linked using hospital record numbers. All data was de-identified for analysis. Duplicate verification of the records was completed to identify errors and missing data. Implausible entries were verified against the set as missing if incomplete. Diagnoses entered as non-standard abbreviations or symptoms were set as missing if they could not be resolved. Following the initial data entry, feedback was provided to the data collection teams to improve the completeness and accuracy of data entry.
Potential sources of Bias
Potential sources of bias were carefully addressed in the study design and data collection. Selection bias was minimized by consistent inclusion and exclusion criteria. To reduce information bias, data collection was conducted using a standardized questionnaire administered by trained researchers. Social desirability and interviewer biases could have also had a role in the reporting of the use of CAM, but its effect on our comparative analysis should be limited since every patient has the same risk. Recall bias, particularly regarding self-reported data such as symptom duration or CAM use, was mitigated by cross-referencing responses with medical records whenever possible. Additionally, efforts were made to ensure that all participants had equal opportunities to respond, regardless of language barriers or health literacy levels, by providing necessary support during the data collection process.
Statistical analysis
The sample size was calculated based on the difference in the rates of CAM use between groups categorized by health literacy scores as inadequate, limited, adequate, and excellent. A total of 189 patients was determined to be sufficient using a chi-square test, assuming a power of 95%, an effect size of 0.2041 (derived from a pilot study with 20 patients), and a Type II error rate of 20% by using PASS 11 software. 22 A pilot study involving 20 patients was conducted prior to the main study to inform the sample size calculation. These data were collected internally and have not been published. IBM Statistical Package for the Social Sciences (SPSS) software (version 27.0; IBM Corporation, Armonk, NY, USA) was used to perform the statistical analysis.
Descriptive statistics, including measures of central tendency and distribution, frequencies, and percentages, were calculated. The normality hypothesis for continuous variables was evaluated using visual methods (histograms) and analytical tests (Kolmogorov-Smirnov/Shapiro-Wilk). Variables were reported as means with standard deviations if the normality hypothesis was not rejected, and as medians with first and third interquartile values if the normality hypothesis was rejected. Comparative analyses were conducted using chi-square or Fisher’s exact tests for categorical variables, while Student’s t-test and Mann-Whitney U-test were used for continuous variables under and not under the normality hypothesis, respectively, to compare two independent groups. Additionally, multivariate logistic regression analysis was performed to examine the impact of variables on delays, with all predictors initially included and stepwise elimination applied to determine the best-fitting model. A p-value of <0.05 was considered statistically significant for all statistical comparisons.
Results
A total of 310 individuals admitted to the outpatient polyclinic and subsequently treated as inpatients in the ward were assessed for the study. Following the application of exclusion criteria (Insufficient data, n = 54; inability to participate, n = 23; lack of consent, n = 43), 190 patients were enrolled in the study (Figure 1).
Sociodemographic and clinical characteristics
Sociodemographic characteristics of the COPD patients according to use of CAM.
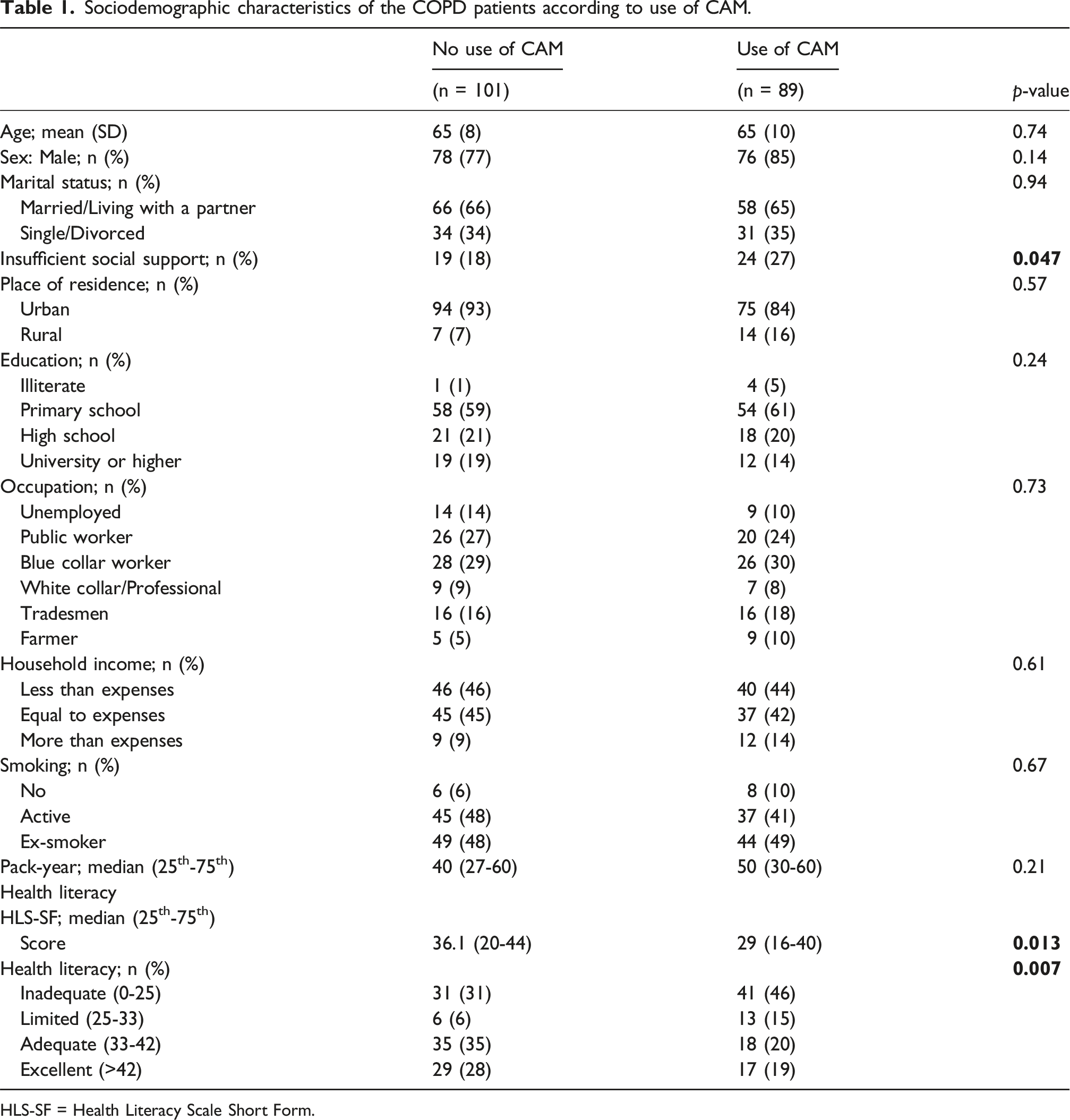
HLS-SF = Health Literacy Scale Short Form.
Clinical characteristics of the COPD patients according to use of CAM.
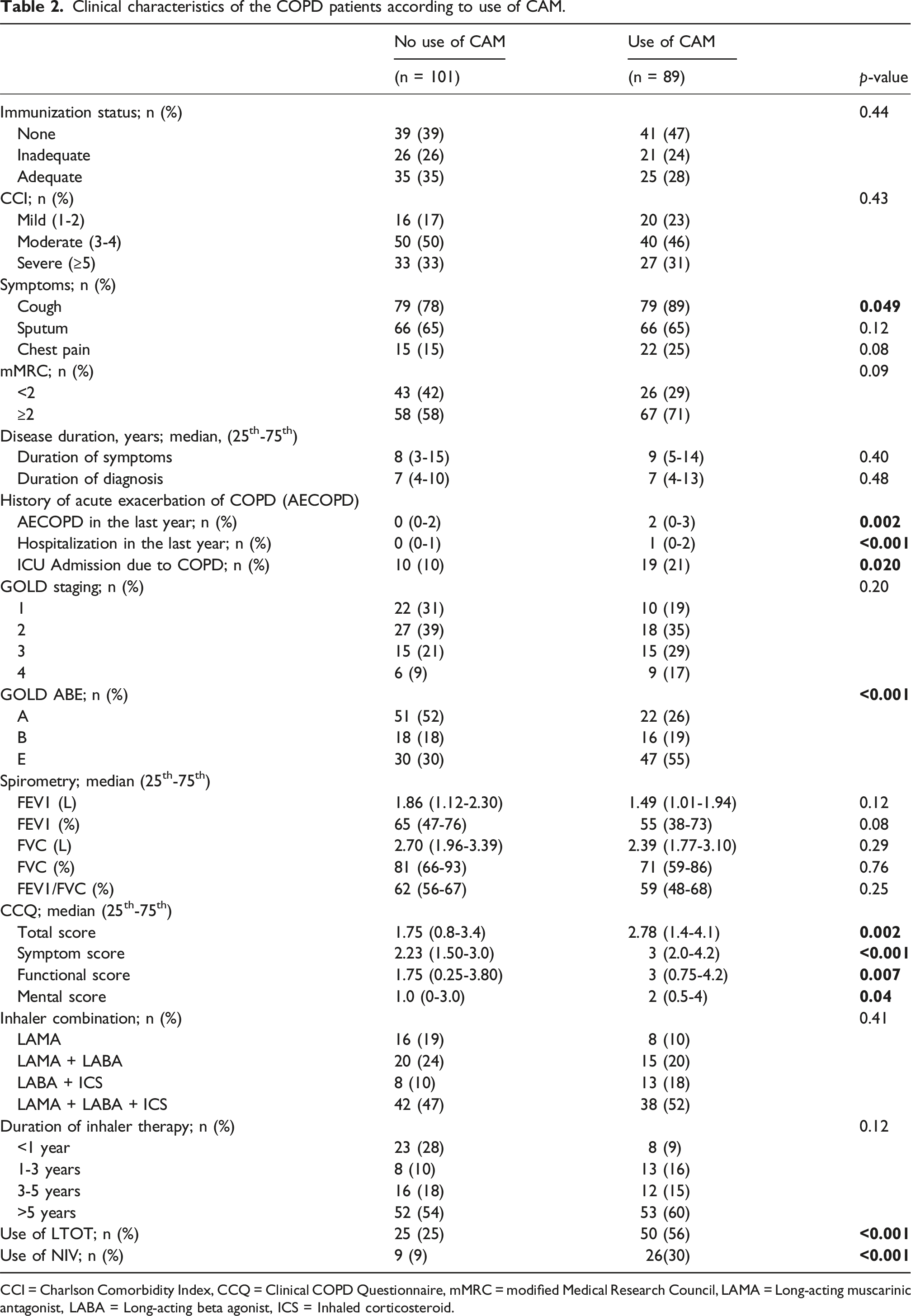
CCI = Charlson Comorbidity Index, CCQ = Clinical COPD Questionnaire, mMRC = modified Medical Research Council, LAMA = Long-acting muscarinic antagonist, LABA = Long-acting beta agonist, ICS = Inhaled corticosteroid.
Types and setting of CAM use
Among the 89 patients using CAM, the most common types of CAM were herbal remedies (n = 67/89, 75%), herbal teas (n = 24/89, 26%), and nutritional supplements/vitamins (n = 17/89, 19%). Less frequently used types included breathing exercises (n = 10/89, 11%), hot springs/baths (n = 6/89, 6%), and other modalities like acupunture, cup therapy, phytotherapy, ozone therapy, and salt caves (all ≤4%). Most patients (n = 73/89, 79%) used CAM at home, while others used it in hot springs/caves (n = 9/89, 10%) or private clinics (n = 2/89, 2%). Only 9% (n = 8/89) consulted a doctor about CAM, and 43% (n = 26/89) reported regular CAM use. Additionally, 7% (n = 7/89) discontinued their prescribed medications while using CAM. Family and friends were the primary sources of CAM knowledge (n = 78/89, 87%), while contributions from the media (n = 2/89, 2%) and from healthcare providers (n = 5/89, 5%) were minimal (Not presented in the table).
Logistic regression analysis
Logistic regression analysis of predictors of the use of CAM.
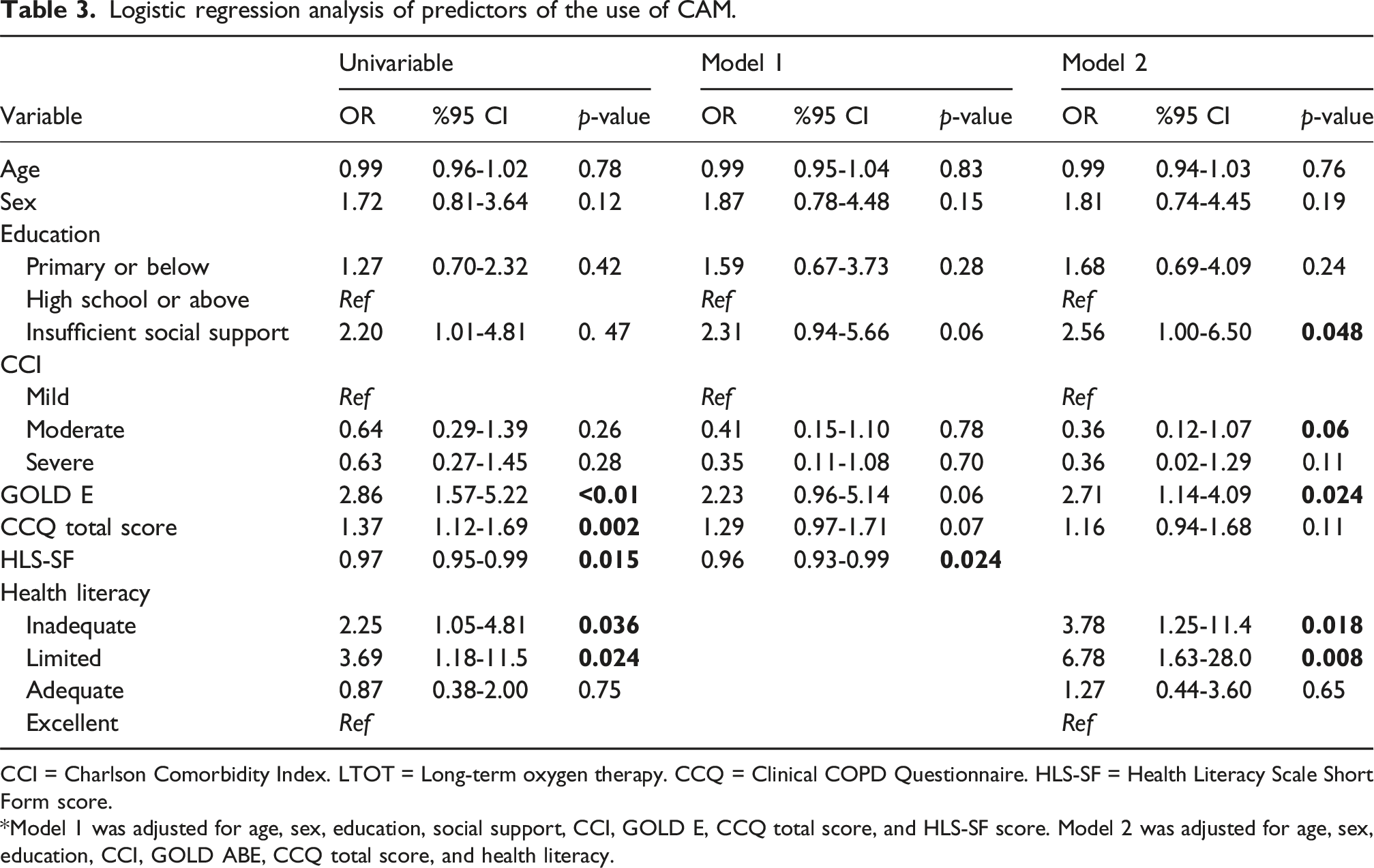
CCI = Charlson Comorbidity Index. LTOT = Long-term oxygen therapy. CCQ = Clinical COPD Questionnaire. HLS-SF = Health Literacy Scale Short Form score.
*Model 1 was adjusted for age, sex, education, social support, CCI, GOLD E, CCQ total score, and HLS-SF score. Model 2 was adjusted for age, sex, education, CCI, GOLD ABE, CCQ total score, and health literacy.
Discussion
The primary objective of this study was to explore the influence of health literacy on the use of CAM in COPD patients. The results indicate that inadequate and limited health literacy is associated with increased CAM use. Additionally, insufficient social support and COPD severity, as assessed by CCQ scores or GOLD classification, were found to be significantly related to the use of CAM.
The use of CAM is widespread, with prevalence rates exceeding 30% in the United States and varying between 0.3% and 86% across European Union countries.16,23 In Türkiye, CAM usage among cancer patients reaches as high as 73%, while prevalence rates among individuals with COPD range from 33% to 86%.24,25 Similarly, a study from Iran found that 95% of COPD patients reported using at least one type of CAM in the past year, with 85.2% favoring medicinal plants, underscoring a strong preference for herbal remedies. 26 Another study reported that 43.2% of COPD patients had previously used CAM, with herbal medicines identified as the most commonly used method, consistent with our findings. 27 Previous studies conducted on different patient groups in Türkiye showed a similar distribution for types of CAM such as the common use of herbal and nutritional products as well as salt caves, and hot springs/baths.28,29 A previous study reported a higher frequency of COPD patients consulting physicians for CAM use (10%) and a similar rate of discontinuing medications during CAM use (8.8%) compared to the present study. 29
Our study observed an association between health literacy and the use of CAM. Addressing the role of health literacy could be crucial, as the low health literacy reported to be associated with poorer self-reported health, increased healthcare costs, more frequent healthcare utilization, higher hospitalization rates, and increased mortality.30,31 A study conducted among chronically ill outpatients identified a significant positive association between health literacy and CAM utilization, with patients possessing higher health literacy being more inclined to adopt CAM methods. 8 The relationship between health literacy and CAM use varies across demographic groups, with some studies showing stronger associations in certain populations than others. 32 The relationship may vary across patient groups, as some studies have found no association for certain diseases. 33 Additionally, understanding the effect of health literacy on the patients’ attitudes could be important since it is a modifiable factor. Another finding of our study, the potential impact of insufficient social support and the use of CAM, is not well-defined and further studies are needed for understand the relationship.
Our study demonstrated that disease severity among COPD patients is associated with the use of CAM. Additional findings, such as an association between frequent exacerbations presented in the GOLD E group, the use of LTOT and the use of CAM could support this association. In general, more severe symptoms are reported to be associated with the use of CAM among patients with different diseases.34,35 Previous studies showed a positive attitude towards the use of CAM associated with disease symptoms, increasing dyspnoea levels and decreased functional status among COPD patients.29,36,37 Various studies reported a statistically significant association between having frequent exacerbation in the last year and use of CAM among COPD patients.27,38 Other studies focused on other chronic lung conditions such as asthma supported the hypothesis on disease severity and an increased use of CAM. 4 These results could indicate an unmet healthcare need as previously mentioned among different patient groups in the literature.4,39
The relationship between education level and the use of CAM is supported by evidence from various studies. Numerous studies have shown a positive association between higher education levels and increased use of CAM. In contrast, our findings indicated an inverse relationship between education level and CAM use. This divergence may be explained by culturally rooted practices, particularly the widespread traditional use of herbal remedies among the Turkish population. For instance, one study found that individuals with higher education, moderate income, living alone, and being employed were significantly more likely to use CAM methods. 26 Similarly, research from Türkiye reported a meaningful difference in the preference for CAM methods based on participants’ educational levels. 40 Another study conducted among cancer patients revealed significant correlations between CAM use and higher education, younger age, and being female, highlighting the role of education in shaping health-related behaviors and decision-making. 41
Strengths and limitations
The strength of this study is its comprehensive approach to the factors potentially associated with the use of CAM, such as sociodemographic features including health literacy, and clinical characteristics. This study has several limitations. The cross-sectional design precludes causal inferences between health literacy, symptom severity, and CAM useMedical adherence to the prescribed medication was not assessed in the study by specific tools and could not be evaluated in terms of the potential effects on the use of CAM. Another limitation is the lack of data on the extent to which CAM was used prior to the onset of reported clinical conditions. Additionally, disease severity may act as a confounding factor in the relationship between health literacy and CAM use, as both variables have been found to be independently associated with disease severity. The assessment of the disease severity was also limited to the CCQ scores, GOLD classifications. Finally, the study population was drawn from a specific region in Türkiye, which may limit the generalizability of findings to other settings or populations.
Future implications
Future research should focus on understanding the prevalence of CAM use among COPD patients through multi-center studies that capture regional and cultural differences. Investigating the factors influencing CAM use, including sociodemographic, clinical, and healthcare system-related variables, is essential to address unmet healthcare needs. Particular attention should be given to health literacy, a modifiable factor, to understand its role in shaping health behaviors and to develop targeted interventions aimed at improving outcomes. Additionally, public health efforts should prioritize educating patients about evidence-based treatments, addressing misconceptions about CAM, and enhancing communication between patients and healthcare providers to mitigate potential risks and promote safe, effective care.
Conclusion
In conclusion, this study identified a notably high prevalence of CAM use among COPD patients and emphasized the potential influence of health literacy, along with the significant impact of disease severity, on the use of CAM. These findings suggest that unmet healthcare needs may play a critical role, and enhancing health literacy and education could help mitigate the potential risks associated with CAM practices.
Footnotes
Acknowledgement
The authors thank the American Thoracic Society and the Turkish Thoracic Society for their collaborative efforts in the MECOR Program, and acknowledge the faculty and teaching assistants of the MECOR Türkiye 2024 Level 3 Program for their valuable contributions.
Ethical considerations
This study was approved by the ethics review boards at Ankara University School of Medicine (2024/486, 2024000486-3).
Consent to participate
All participants provided written informed consent prior to participation. The study was conducted in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.