
Abstract
Polyneuropathy has been observed in patients with chronic obstructive pulmonary disease (COPD). If polyneuropathy occurs as a complication or extrapulmonary manifestation of COPD, one would expect an increased prevalence among patients with a cryptogenic axonal polyneuropathy. This case–control study aimed to investigate the association between COPD and polyneuropathy. We prospectively included 345 patients with cryptogenic axonal polyneuropathy and 465 controls. A standardized questionnaire assessed the presence of COPD and we verified this diagnosis by contacting the family physician. The severity of COPD was based on the Global Initiative for Chronic Obstructive Lung Disease classification. The prevalence of COPD did not differ between patients with polyneuropathy and controls (15/345 vs. 12/465 respectively; odds ratio (OR) 1.7; 95% confidence interval (CI) [0.8–3.7]). Adjusting for age, gender and possible confounders did not affect these results (adjusted OR 1.7, 95% CI 0.7–4.1). The severity of COPD was similar between patients with polyneuropathy and controls. This study does not support the hypothesis that COPD is a risk factor for polyneuropathy.
Introduction
Besides pulmonary manifestations, chronic obstructive pulmonary disease (COPD) has extrapulmonary comorbidities such as cardiovascular disease, metabolic syndrome, and diabetes. 1 –4 There is growing evidence that systemic inflammation plays a role in COPD and comorbid conditions, which is why some consider COPD a systemic rather than just a pulmonary disease. 1,2
Polyneuropathy has been observed in patients with COPD. 5 –7 A typical polyneuropathy presents distally in the feet with sensory symptoms and slowly progresses to a symmetrical “glove and sock” like pattern of sensory loss and muscle weakness of feet and hands. Common causes of polyneuropathy are diabetes mellitus, excessive alcohol consumption, renal insufficiency, vitamin deficiencies, thyroid disease, and toxic medication (especially chemotherapy). In approximately 25% of patients with polyneuropathy, no cause can be found, the so-called cryptogenic axonal polyneuropathy, which is also associated with cardiovascular disease and the metabolic syndrome. 8 –11
In view of shared comorbidities, an increased prevalence of COPD among patients with cryptogenic axonal polyneuropathy may be expected if polyneuropathy truly is a complication or extrapulmonary manifestation of COPD. This prospective case–control study aims to investigate the association between COPD and polyneuropathy.
Methods
The present study is part of a prospective controlled study on the etiology of cryptogenic axonal polyneuropathy initiated in 2008 at the University Medical Center Utrecht (UMCU), which was approved by the Medical Ethics Committee.
Patients
Patients were referred to the UMCU neuromuscular outpatient clinic by their family physician or by a neurologist in a general hospital. After obtaining informed consent, we included all patients (n = 345) in whom cryptogenic axonal polyneuropathy was diagnosed in the UMCU between October 1, 2008 and July 1, 2012. Patients were clinically evaluated for polyneuropathy in a standardized fashion. The diagnosis of cryptogenic axonal polyneuropathy was based on diagnostic criteria as detailed previously. 11 Briefly, patients had to have ‘glove and/or sock’ like distribution of sensory or sensorimotor symptoms (self-reported as well as on neurological examination) compatible with polyneuropathy. The onset of polyneuropathy should have occurred in the feet and after the age of 40, as in younger patients a hereditary polyneuropathy should always be suspected. The diagnostic workup in all patients consisted of protocolled laboratory investigations that had to be normal to exclude underlying causes of the polyneuropathy and standardized nerve conduction studies (NCS) to confirm an axonal polyneuropathy. 11–12
Controls
Persons participating as healthy controls in a prospective population-based ALS study in the Netherlands (PAN) that is currently being carried out in the UMCU were also used as controls for our study. 13 In PAN, family physicians of patients with amyotrophic lateral sclerosis are asked to send out information on PAN to persons listed below the patient in the alphabetized register, matched for gender and age. After giving informed consent, these controls were included in PAN. After exclusion of persons <40 years and those with a known polyneuropathy or common associated conditions (diabetes, thyroid disease, and excessive alcohol consumption) a total of 465 controls were included in this study.
Chronic obstructive pulmonary disease
All study participants completed a standardized questionnaire that addressed general health, medical history, medication use, smoking habits, and alcohol consumption. It specifically questioned about the presence of any chronic pulmonary disease and if present, the diagnosis, the time of diagnosis, and current use of inhalation medication. We contacted the family physician for additional information in all participants reporting a diagnosis of COPD, emphysema, asthma, asthmatic bronchitis, or chronic bronchitis. The Dutch health-care system is organized in such a way that COPD will be diagnosed, treated, and followed up mostly by family physicians, and only severe or complicated cases will be referred to a pulmonologist. There is a clear guideline by the Dutch College of General Practitioners on the diagnostic and therapeutic approach in patients suspected of COPD and includes instructions on performing spirometry and interpreting spirometry results, conforming to international guidelines of the European Respiratory Society and the American Thoracic Society. 14 The family physician was asked about the registered diagnosis, either made by the pulmonologist or the family physician, and spirometry test results were collected. Participants were considered to have COPD only after confirmation of this diagnosis by their family physician and supported by the available spirometry test results. The severity of COPD, expressed by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification system, was based on verification of the most recent available spirometry test results as obtained by the family physician. 15 We defined the duration of COPD as the interval (years) between the patient reported time of diagnosis of COPD and completing the questionnaire. The duration of COPD was compared to the duration of polyneuropathy in patients, which we defined as the interval (years) between the diagnosis of polyneuropathy and completing the questionnaire.
Statistical analysis
Statistical analyses were performed with the Software Package for Social Sciences (SPSS version 20.0/22.0). Characteristics of patients with polyneuropathy and controls were compared using χ2 statistics or Fisher’s exact test (ordinal and nominal variables) and Student’s t-test or Mann–Whitney U test (continuous variables). With the observed prevalence rates of COPD in patients with polyneuropathy and controls, we calculated the odds ratio (OR) with the 95% confidence interval (CI). Multiple logistic regression analysis, adding possible confounders to this model, was used to calculate an adjusted OR with 95% CI. Besides adjusting for age and gender, level of education, lifetime alcohol intake (average number of drinks per week times total number of weeks of alcohol use), hypertension (defined as the use of antihypertensive medication), dyslipidemia (defined as the use of lipid-lowering medication), and body mass index (BMI) were added as possible confounders. We added hypertension, dyslipidemia, and BMI, because these cardiovascular risk factors and the metabolic syndrome are more prevalent in both patients with cryptogenic axonal polyneuropathy and patients with COPD compared to controls. 1 –4,11 Smoking is one of the most important risk factors for COPD, but there is no evidence of an independent association with polyneuropathy. 16 Therefore, smoking was not considered a possible confounder. Collinearity between factors was checked and no factor had to be excluded. The p values <0.05 were considered statistically significant.
Results
Characteristics of the 345 patients with polyneuropathy and 465 controls are shown in Table 1. Patients with polyneuropathy are older and more often men compared to controls, hence results were adjusted for age and gender. Fewer patients with polyneuropathy than controls are current smokers or use alcohol, but percentage of subjects ever smoking, total pack-years, and lifetime alcohol intake are similar. Patients with polyneuropathy more often use antihypertensive and lipid-lowering medication, have a higher BMI, and more frequently report myocardial infarction compared to controls. Severity of COPD could not be retrieved in three subjects: two patients with polyneuropathy had died (in one the cause of death was unrelated to COPD, in the other the cause of death was unknown) and one control did not give permission to contact the family physician.
Characteristics of patients with polyneuropathy and controls.a

BMI: body mass index.
aData are mean ± standard deviation (SD) or median (range) unless otherwise specified.
b χ 2 statistics.
cStudent’s t-test.
dExcluding patients/controls that never smoked.
eMann–Whitney U test.
fExcluding patients/controls that never drank alcohol.
The data on COPD in patients with polyneuropathy and controls are shown in Table 2. The prevalence of COPD is similar in patients with polyneuropathy and controls (4% vs. 3%; OR 1.7; 95% CI: [0.8–3.7]). Adjusting for age, gender, and confounders does not affect these results (adjusted OR 1.7; 95% CI: [0.7–4.1]). None of the patients with polyneuropathy or controls have COPD GOLD III/IV. The duration of COPD in patients with polyneuropathy is significantly longer than in controls. All patients with polyneuropathy had the diagnosis of COPD prior to the diagnosis of polyneuropathy.
Prevalence, severity, and duration of COPD in patients with polyneuropathy and controls.a
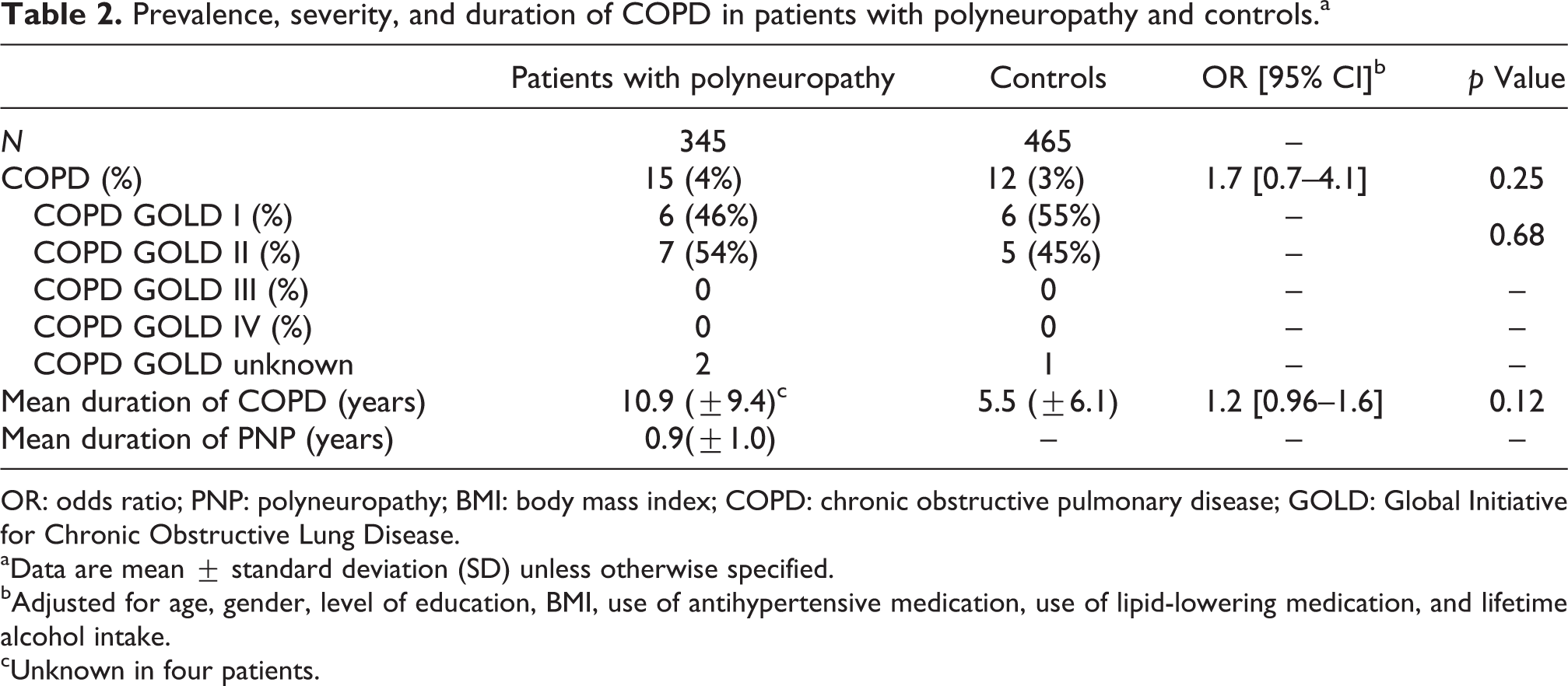
OR: odds ratio; PNP: polyneuropathy; BMI: body mass index; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease.
aData are mean ± standard deviation (SD) unless otherwise specified.
bAdjusted for age, gender, level of education, BMI, use of antihypertensive medication, use of lipid-lowering medication, and lifetime alcohol intake.
cUnknown in four patients.
Data comparing smoking habits of patients with polyneuropathy and controls are shown in Table 3. Seventy-three percent of patients with polyneuropathy and COPD have ever smoked compared to 100% of controls with COPD, and 7% of patients with polyneuropathy and COPD are current smokers compared to 42% of controls with COPD. The median pack-years of smoking of both patients with polyneuropathy and COPD and controls with COPD is significantly higher compared to patients with polyneuropathy without COPD and controls without COPD.
Smoking habits and COPD in patients with polyneuropathy and controls.a
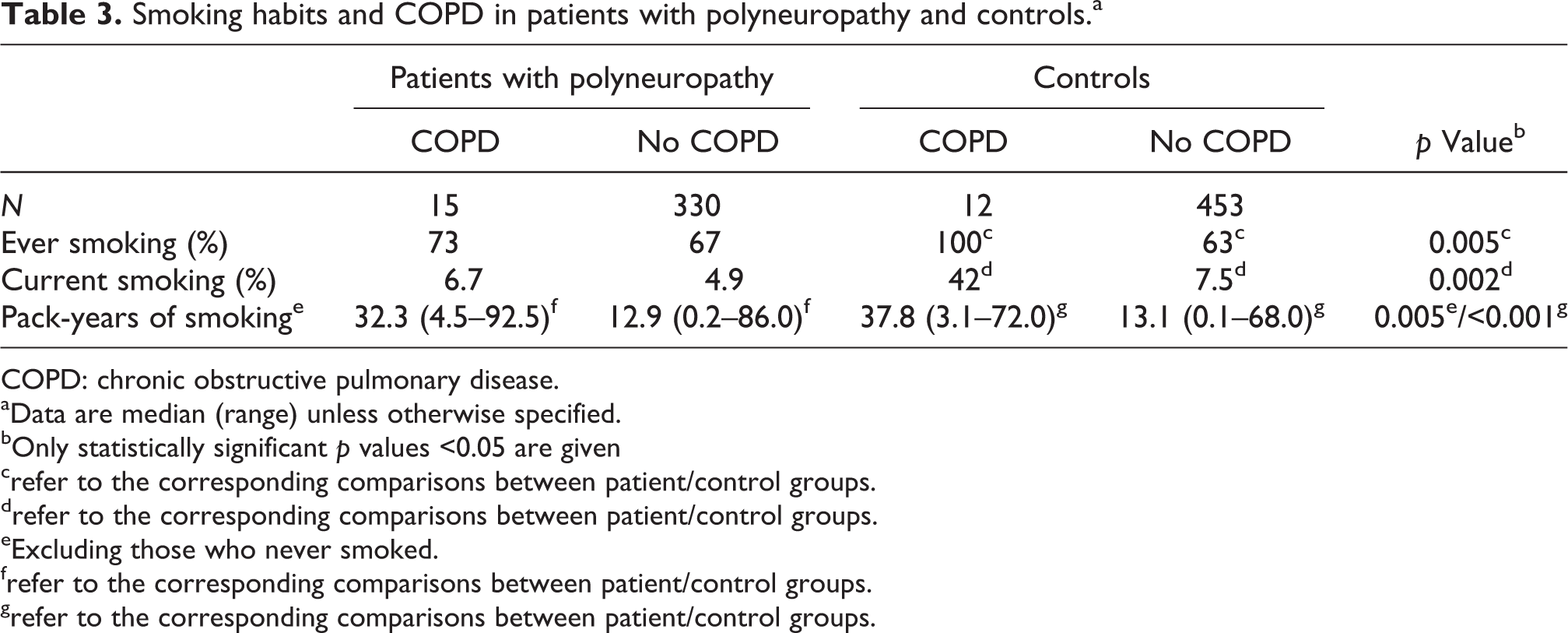
COPD: chronic obstructive pulmonary disease.
aData are median (range) unless otherwise specified.
bOnly statistically significant p values <0.05 are given
crefer to the corresponding comparisons between patient/control groups.
drefer to the corresponding comparisons between patient/control groups.
eExcluding those who never smoked.
frefer to the corresponding comparisons between patient/control groups.
grefer to the corresponding comparisons between patient/control groups.
Discussion
This is the first prospective case–control study to investigate COPD as a risk factor for cryptogenic axonal polyneuropathy, and the results provide no support for an association.
To investigate a possible association between COPD and polyneuropathy, a study population of patients with cryptogenic axonal polyneuropathy is suitable, because this avoids confounding by conditions that are known to be comorbidities in COPD as well as established causes of polyneuropathy. 17 –19 Table 4 gives an overview of three previous small controlled studies that investigated the association between COPD and polyneuropathy, in which an effort was made to exclude common underlying causes. 5 –7 In these studies, the prevalence of polyneuropathy was more than four times higher than in population-based studies in persons ≥40 years old. 20–21 Because electrophysiological confirmation of polyneuropathy by nerve conduction abnormalities in the lower extremities was not required, there was very likely an overestimation of the prevalence of polyneuropathy in COPD and a spurious association.
Overview of the literature on COPD and polyneuropathy.

NCS: nerve conduction study; M: median nerve; U: ulnar nerve; F: fibular nerve; SF: superficial fibular nerve; S: sural; n.a.: not available; COPD: chronic obstructive pulmonary disease.
aOne patient had symptoms and signs compatible with polyneuropathy and six patients had symptoms and signs possibly compatible with polyneuropathy.
bNerve conduction study abnormalities in ≥1 nerve of upper or lower extremities.
cReduced sensory nerve action potential or compound muscle action potential in ≥1 nerve of upper or lower extremities.
dNerve conduction study abnormalities in >1 nerve of upper or lower extremities and vibration perception threshold outside normal limits.
Physician diagnosed COPD based on the presence of symptoms combined with spirometry results according to established guidelines has a reported prevalence of 3–5% in the Dutch population aged ≥40 years, 22 –24 and therefore we consider our study population as a representative sample. We are aware that higher prevalence rates are reported in population-based studies in which COPD is diagnosed based on spirometry test results irrespective of the presence of symptoms. 25 We determined the prevalence of physician diagnosed COPD in a similar fashion in all participants. The degree of underestimation would have been similar in patients and controls, which makes it unlikely that the findings would have been different if all participants had been screened by spirometry. The estimated distribution of physician diagnosed COPD in the Netherlands shows that 27% of patients has COPD GOLD I, 55% COPD GOLD II, 15% COPD GOLD III, and 3% COPD GOLD IV. 26 It is noteworthy that in our study there were no participants with severe COPD (GOLD III/IV). Controls volunteering to participate in research are generally in relatively good health, which makes it understandable that controls with severe COPD are lacking. The absence of patients with polyneuropathy and severe COPD could be the result of them not wanting to participate in a study or not being referred for study participation due to the severity of their pulmonary disease. Alternatively, it could be the presence of comorbidities that are even more prevalent in (very) severe COPD, are also an identifiable cause of polyneuropathy, and precluded study participation.
All of our patients with polyneuropathy had received the diagnosis of COPD prior to that of polyneuropathy, but 4/15 patients reported polyneuropathy symptoms prior to the time of diagnosis of COPD. We did not enquire into the onset of symptoms of COPD, and it is questionable that this could have been ascertained with sufficient reliability. It remains uncertain in these four cases whether COPD symptoms were already present at the debut of the polyneuropathy or the symptoms of polyneuropathy actually preceded the onset of COPD. Exclusion of these four patients would have strengthened the lack of an association between COPD and polyneuropathy.
One of the hypotheses for the underlying mechanism of polyneuropathy in COPD has been the effect of chronic hypoxia on the peripheral nervous system. 5,27 Because chronic hypoxia especially affects patients with more severe COPD, this would mean polyneuropathy would mostly affect patients with more severe COPD. An alternative hypothesis is that polyneuropathy is an extrapulmonary manifestation due to systemic inflammation in COPD. The metabolic syndrome, also a systemic inflammatory condition, is associated with polyneuropathy that is likely a result of microvascular changes. 11 Microvascular changes, like an increased basal lamina area thickness of endoneurial vessels, are known to play a role in the pathogenesis of some polyneuropathies as they are found in sural nerve biopsies of patients with diabetic polyneuropathy as well as cryptogenic axonal polyneuropathy. 28
In summary, our study does not provide evidence for the hypothesis that polyneuropathy is a complication or extrapulmonary manifestation of COPD. In patients with COPD who develop a properly defined polyneuropathy, it is more likely that there is an underlying condition that is associated with COPD as well as an established cause of the polyneuropathy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LHvdB reports receiving personal fees from Biogen Idec (Scientific advisory board) and Baxter (Educational grant, Travel, Scientific advisory board), but no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome. All other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (WAR 07-24) from the Prinses Beatrix Spierfonds.