
Abstract
The objective of this study was to identify the necessary features of pulmonary telerehabilitation (P-TR) from the perspectives of individuals living with chronic lung disease and health care professionals (HCPs) who deliver pulmonary rehabilitation (PR). Focus groups were carried out with patients (n = 26) and HCPs (n = 26) to elicit and explore their opinions about the critical elements of in-person PR and ideas for how these elements could be supported using technology. A questionnaire was used to assess technology use, PR experience, and general health status. Four key elements of PR were identified as critical to P-TR: the social aspect of PR; communicating with HCPs for education and support; using biosensors for monitoring and promoting self-knowledge; and the evolution of support with progress over time. A range of technology-enabled devices and programs were suggested as means to recreate aspects of these integral elements. Consultations with patients and HCPs suggest that users are interested in technology and want to ensure it recreates the important aspects of PR. Patients and HCPs identified similar key elements for P-TR. The opinions and suggestions of patients and HCPs should be the driving force of innovation if P-TR is to succeed in improving health outcomes.
Keywords
Background
Pulmonary rehabilitation (PR) is an exercise and education program for people with chronic lung conditions, including chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, and asthma. 1 –3 PR provides individualized exercise and education sessions to increase activity tolerance, reduce symptoms, and improve skills to manage chronic lung disease. 1 –3 PR is typically provided in person in a group format, with individuals supervised by health-care professionals (HCPs) in a hospital or community setting. 1 –4 Unfortunately, however, there are not enough PR programs to meet the needs of individuals living with chronic lung disease. 4
Telehealth, the remote delivery of health-related services using information communication technology, may support alternative approaches to deliver traditional in-person PR. 5 Pulmonary telerehabilitation (P-TR) may help overcome access barriers for individuals living in nonurban areas and those unable to participate in person due to other commitments, such as employment. It may also be used as an adjunct to in-person PR to support self-management and positive behavioral change. Monitoring bioparameters using technology, known as telemonitoring, as part of P-TR may also enhance preventive management by providing early warnings of deterioration, which may minimize hospitalizations and decrease health care costs.
Telehealth and telemonitoring have demonstrated benefits for self-management in patients living with other chronic conditions 6 –10 and provide opportunities for supporting those living with chronic lung disease. 10 –13 However, several studies in telehealth and telemonitoring in COPD have demonstrated mixed results. Pinnock et al. 14 and Fairbrother et al. 15 explored telemonitoring using quantitative and qualitative methodology and found that telemonitoring of oxygen saturation combined with daily symptom and treatment questionnaires increased patients’ knowledge of their condition and gave them direction on when and how to contact their HCPs. However, the use of telemonitoring for patients with COPD did not impact hospital admissions or improve quality of life. 14
Studies on telehealth and telemonitoring in the context of rehabilitation (tele-rehabilitation) have also been conducted but without consistency in terms of the intervention. A range of P-TR formats have been examined: some trials have delivered education using telehealth but retained in-person exercise training, 13 while others are currently exploring individualized exercise training at home while using telemonitoring and videoconferencing. 16,17 The variability may be due, in part, to the various communication technologies and exercise tracking devices that offer many ways to monitor activity and communicate education materials, advice, and reminders that could support the delivery of P-TR. However, while the technologies and capacity exist, there are many questions about the necessary features of P-TR and how to implement them effectively. Furthermore, acceptance of technologies by patients and HCPs is critical to the success of novel telehealth initiatives. 18 To maximize the likelihood of success, users should be involved in early stages of development of new technologies 19 or work in codevelopment on system design and testing. 20,21 This may be particularly pertinent in an older population, and in more rural settings, where chronic lung disease rates are high. 22,23
Ultimately, to define the requirements of P-TR delivered by HCPs for individuals living with chronic lung disease, we must first determine patient and HCPs needs. In this study, we sought opinions of individuals living with chronic lung disease, and HCPs delivering PR, to determine the critical features of P-TR and how technologies could support these features.
Methods
This study was approved by Providence Health Care/University of British Columbia Research Ethics Board (H14-01329). Participants provided written informed consent. The design included questionnaires and focus groups. Separate focus groups were held with patients and HCPs. Seven focus groups were conducted with patients (n = 26) in hospitals or community health settings and two with HCPs (n = 26, one in person in hospital and one online using web-based videoconferencing).
Individuals with chronic lung disease were recruited to provide perspectives from both people who participated in PR programs and those who did not participate due to difficulty traveling to program locations. Potential patient participants were notified about the study by the hospital-based PR program staff and if interested their contact details forwarded to the study team. The study team was not involved in the patients’ care. Individuals were eligible if they were 35 years or older, diagnosed with a chronic lung condition, and fluent in English.
Eligible HCPs were registered as a physiotherapist, nurse, respiratory therapist, kinesiologist, or physician, with regular experience in treating COPD patients (a consistent component of their patient population within the preceding 6 months); involved in exercise prescription, monitoring, and progression in a PR program; and fluent in English. The HCPs were recruited locally and through a network of PR programs in the province.
Participants completed a questionnaire about their demographics and current technology use (regular use defined as daily or weekly use). Patients identified their lung disease; years since diagnosis; assessment of self-reported health status (5-point scale ranging from Excellent to Poor); and current activity level (recall of activities over the past 7 days). The HCPs were asked questions about their health discipline, years of PR experience, and primary PR responsibilities. Counts and proportions were calculated using R (Version 3.1.1, Vienna, Austria) 24 and Microsoft Excel (2007, Microsoft Corporation, Washington, DC).
The PR expert and lead facilitator (P.G.C.) discussed the potential of using telehealth to deliver PR and demonstrated some portable devices related to health, physical activity, and oxygen saturation: pulse oximeters (Model 8500 Handheld Pulse Oximeter, Nonin™, and Kenek O2 Pulse Oximeter; LionsGate Technologies, Vancouver, Canada), pedometers, activity trackers (Fitbit™), and smartphone applications. A semi-structured, open-ended discussion was cofacilitated by the PR expert and an eHealth content expert (H.N.L. or J.A.I.). The focus group question guide (Appendix 1) included participants’ PR experiences, their vision of technology-delivered PR, and what parameters were critical to P-TR. Focus groups were 1.5 to 2 hours, audio-recorded, and transcribed verbatim.
All identifying information was removed from the transcripts. An inductive approach to the analysis was used; content analysis was performed to categorize the findings according to emergent themes guided by the research questions. First, two research team members coded the transcripts independently with the assistance of NVivo (Version 10.2.1, QSR International, Doncaster, Australia). An open-coding approach was tempered with keeping in mind the broader areas of inquiry as outlined in the focus group questions. The two researchers met to discuss the codes they derived to ensure consistency. Overall, coding was consistent across the two researchers, and codes with the same meaning but to which a different descriptor was applied were renamed for consistency. Units of analysis/excerpts of text to which the codes were applied were scrutinized for discrepancies; where disagreement occurred, the instances were discussed and where appropriate, the codes changed. The researchers reviewed the codes and grouped them into meaningful categories. This process was done iteratively, with researchers meeting to discuss categories, reconcile differences in interpretations, draw broad themes in relation to the research questions, and determine that saturation was met. Once the categorization was established, themes outlined, and all meaningful units of analysis/excerpts grouped accordingly, two randomly selected coded transcripts were read by a third team member to confirm that no codes, categories, or themes were omitted.
Results
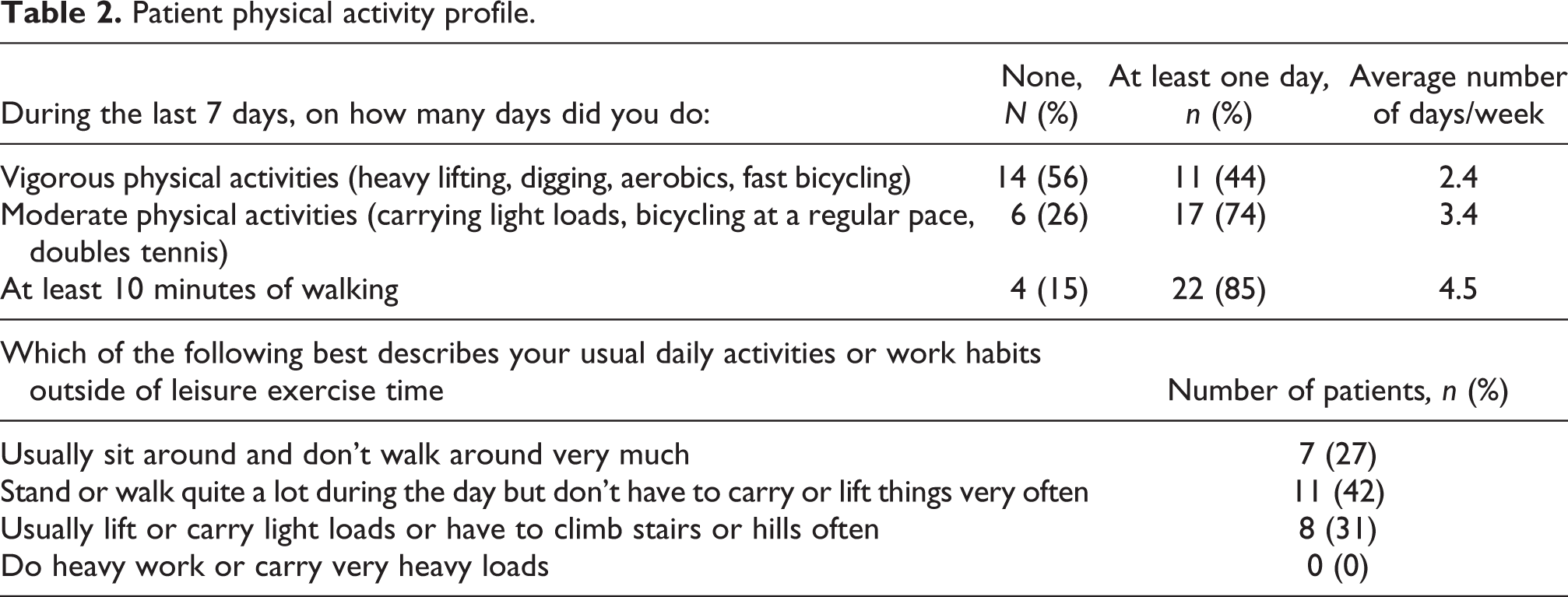
The study involved 52 participants, including 26 patients who participated in 7 focus groups. Patient characteristics are shown in Table 1. Most patients were diagnosed with COPD (73%), followed by asthma, and interstitial lung disease (ILD). Fifteen (58%) participants had participated in PR; three of these participants had challenges attending all PR sessions. Patient physical activity characteristics are shown in Table 2. Twenty-six HCPs participated in two focus groups (one in person and one online). The HCP characteristics are shown in Table 3. Half of the HCPs were respiratory therapists, just under half were physical therapists, and one was a nurse.
Patient characteristics.

Patient physical activity profile.
Health care professional characteristics.

SD: standard deviation.
Patients’ and HCPs’ use of consumer technologies is shown in Figure 1. Most patients were regular users of a home computer, less than half were regular users of cellphones and less than a quarter were regular users of smartphones or tablets, of the patients who weren’t regular users of computers, a majority (6/8) answered they were “not at all comfortable” with the technology. Similarly, a majority of patients who were not regular users indicated that they were “not at all comfortable” with tablets (15/21) or smartphones (11/22). All HCPs used computers on a regular basis, and more than 75% were regular users of tablets and smartphones.

Patients’ and health care professionals’ regular use of consumer technologies. Regular use was defined as daily or weekly use.
The focus groups revealed several elements that both patients and HCPs considered essential for P-TR. Grouped into four major themes, described subsequently, these elements included the social aspect of PR, communicating with HCPs, using biosensors for monitoring and self-knowledge, and the evolution of support with progress over time. The HCPs also raised unique points on technology and scope of practice.
Theme 1: Maintaining the social aspect of pulmonary rehabilitation virtually
Patients and HCPs both identified the social aspect of group exercise and education as a critical component of PR. Patients relayed how the social aspect increased their accountability, motivation, and feeling of belonging to a group. To recreate the social aspect and build virtual networks, patients suggested group video chats with peers, group exercise sessions with individuals in their own home, and interactive video game consoles (Table 4). Others described exchanging contact information and creating a formal buddy system with routine check-ins. In communities where multiple individuals live with lung disease, participants imagined a central gathering site such as a local community center or gym, where PR could be delivered—enabling the social aspect with remote HCP support. I just had visions of a room with equipment where you could actually do the program on a big screen TV and someone could lecture and you could sit down after and do the education portion and have kind of everybody there at once cause I don’t know about you too but I like having people around. I work out better when I’m in a group of people. (Female, 69 years)
Quotes supporting main themes from patient participants and health care professionals.

The HCPs described blogs that facilitate patient interaction and motivation with intermittent moderation by an HCP, noting this strategy has been successful in other diseases. A group blog or messaging service was also suggested for “other patients to contact each other, ‘oh how are you getting on today?’ and that could be their own support group” (HCP, ID1). The HCPs also identified value in smartphone applications that enable activity logging, social interaction, and gamification of exercise to reinforce goal-setting and provide rewards.
Theme 2: Communicating with HCPs for education and support
Traditional PR includes a large amount of face-to-face time with a variety of HCPs; patients receive individual exercise prescription and group education modules with opportunities to ask questions and receive one-on-one counseling. Patients described the encouragement from their HCP as particularly important for their progress in the exercise component, specifically including the importance of having instructors with a caring personality and a personal touch (Table 4).
Patients described how tele-technologies could facilitate their interaction with HCPs. Patients discussed having encouraging messages on tape, such as “you’re doing great”, “get out of bed”, “get your act together,” and other reminders or feedback. For the education component, patients suggested video-sharing programs so that they could watch the videos multiple times including with their families to enhance involvement in their care. One participant noted she would use it to “educate my husband because the more I learn the more I can help him learn what’s wrong with me…help him understand what I’m doing and trying to do” (63 years). The opportunity to ask questions following the videos, and between medical appointments, using technology was also highlighted.
Some HCPs were concerned about the frequency of technology-enabled communication and the boundaries of their role. There were suggestions of having specific times for check-ins, when HCPs are expected to be online and present. Overall, additional opportunities for new ways of communicating with patients were viewed as positive (Table 4).
Theme 3: Using biosensors for monitoring and promoting self-knowledge
Patients and HCPs are accustomed to monitoring bioparameters during PR. The utility and challenge of bioparameters was apparent to patients and HCPs who described the opportunity to learn about physiology, without forgetting to monitor other symptoms (Table 4). Patients identified heart rate and oxygen saturation as key bioparameters to record when exercising at home to inform titration of exercise to an appropriate intensity. Patients described using these parameters to identify their limits, when they should rest or work harder. Above all, patients described that it was empowering to know their bioparameters and observe improvements over time.
Patients described learning to make associations between the numbers they record and how they feel, having to rely on the numbers less as they progress. Patients who described being more confident in identifying how they feel found the bioparameter information less important—they could identify what reaction was necessary and respond accordingly. HCPs also recognized that patients were empowered by their understanding and use of bioparameters.
HPC’s identified that it is important for technology solutions to be customizable to different patients, depending on their goals, medical needs, and exercise activities: “a suite of different things that could be part of the technology that’s based on what the patient’s goals are” (HCP, ID16). Some HCPs identified challenges in having patients consistently record their numbers in inpatient PR and were concerned about ensuring that individuals exercising off-site would record this information: “people are supposed to record their numbers and they consistently forget to so it ends up falling on me to do that. So even when it’s very simple…you’re already supposed to collect it, they just don’t.” (HCP, ID3)
Theme 4: Evolution of support as the patient progresses over time
The changing nature of support that patients require over time was evident in the patient and HCP description of PR. In the early stages of rehabilitation, patients described many individual barriers to exercise, including fear and anxiety, which were alleviated by working with trained HCPs in the hospital setting. Other patients echoed that having a safe environment at the start of their rehabilitation was critical. As patients progressed through the PR program, they developed more confidence (Table 4).
In imagining a remote telehealth-based program, patients and HCPs also identified how technological features could be individualized and support the transition from a formal PR program to ongoing physical activity maintenance. One HCP described how P-TR could evolve and have different tiers of management depending on the patients’ progression (Table 4). Another HCP described how the use of technology at home might promote “more onus on the individual to be active in their rehab…working in their day to day life and so they take it on, integrate it into their own lives” (HCP, ID3).
Health care professional perspectives on technology and scope of practice
HCP’s raised concerns unique to their perspective and scope of practice in an increasingly technical world. The workload implications of incorporating P-TR in addition to their regular duties, and the requirements to be technologically adept, were raised as a concern: “I would want it to not be off the side of the desk of people already working to capacity and beyond. It would need to be some dedicated time, dedicated people…who were…computer savvy” (HCP, ID10). Others reiterated that technology training would also be essential to the success of P-TR.
The HCPs appreciated the value of using technology to increase access to rehabilitation services to underserved communities: “you could see people improve and these are people who otherwise would not have had that…it’s satisfying cause you’ve helped somebody who would have probably just deteriorated” (HCP, ID3). When considering their own practice and job satisfaction, several agreed having a balance of in-person and remote patients was appealing: I wouldn’t want to be just monitoring people from a distance all the time, but it would actually be quite a nice mix if you’re doing in-person pulmonary rehab as well as the distance and there’s sometimes when it’s kind of nice to get a break from the direct interaction occasionally. (HCP, ID6)
Conclusion
Summary of main findings
This study explored patient and HCP perspectives on the format and parameters for delivering PR using telehealth technologies. Patients were less frequent users of consumer technologies than HCPs and appeared less comfortable with them but were still receptive to technological adaptations of PR. Specifically, we identified four themes based on participants’ perceptions and experiences that were critical to P-TR, including social aspects, communication with HCPs, measuring bioparameters, and evolving support. Participants suggested possibilities to recreate these critical elements using technology for application to P-TR. These essential elements were reiterated and supported by HCPs.
Limitations of this study
Patients were purposefully selected to include perspectives from individuals who attended in-person PR and those who did not attend due to distance limitations. We did not recruit urban patients who did not participate in PR, which may limit the breadth of the ideas and generalizability. However, the development of P-TR, and its increased flexibility, will likely benefit urban patients as well. All participants resided in British Columbia, Canada, where there is reliable Internet and cellphone connectivity. In spite of this, less than a quarter of the participants with chronic lung disease were regular users of tablets or smartphones. Currently, this may limit the choice of technologies used and the reach and impact of P-TR programs but would likely change in the future, as technology-savvy patients with COPD are referred to PR. In addition, we did not explore how other factors such as disease characteristics, gender and age, or the presence of comorbid conditions could have impacted our results. Future research should focus on these factors. Finally, the current study does not address patients who declined to participate in PR due to other relevant reasons such as anxiety, motivation, or confidence to exercise. These patients may not be good candidates for P-TR programs or would require a transition to more independent exercise as their program progressed.
Context in existing literature
New technologies and increased individual Internet connectivity provide the opportunity for a telerehabilitation strategy tailored to individual patients and environments. P-TR may help overcome access barriers for individuals living in rural areas. Previous studies have used novel technologies to deliver PR, demonstrating the feasibility of P-TR. 13,25 –27 Self-monitored home-based exercise has been shown to improve dyspnea and health status, 26 and participants’ compliance with accelerometer/smartphone activity monitoring is high and associated with improved activity levels. 25 Longer term studies that observe health outcomes and how people use technology in P-TR remain warranted.
Technology is already a large part of HCPs’ practices. Charting on electronic health records, booking patients online, and communicating with patients using different media mean that most HCPs are required to be familiar with technology; however, HCPs described not wanting to lose the in-person part of their job completely. There was also hesitation about supporting patient technology use and troubleshooting. Assistance from dedicated information technology staff may be necessary to facilitate the implementation and success of P-TR. In turn, it will be critical to clearly outline expectations for patients and HCPs when adopting P-TR—highlighting when communication will or will not be real time.
Telerehabilitation has been used to manage chronic diseases including cardiac disease, 28 stroke, 29,30 multiple sclerosis, 31 and arthritis. 32 –34 In adapting successful in-person rehabilitation programs, the focus has primarily been on the technological requirements, 35 human factors, 36 and barriers to use. 29 The patient experience of rehabilitation is very important, and a variety of needs assessments with patients and HCPs have been used to identify interest in rehabilitation programs and help with their design. 37,38 The ongoing assessment of new programs using qualitative methods also helps to understand the patient experience and identify important issues. 39–41
The next steps for P-TR include addressing implementation costs, staffing, safety, patient referral, and discharge processes. The cost-effectiveness of telehealth for consultation in COPD appears promising, with reduced hospitalizations and acute exacerbations compared to traditional care. 42 Full health economic and health impact analyses of P-TR are currently underway for a web-based PR program. 43 Policies on HCP training and standards will also need to be reviewed; the interdisciplinary composition of PR means that HCPs are under the jurisdiction of different colleges and regulations. These practical considerations will be important for successful implementation.
Implications for clinical practice
Telehealth solutions hold promise to increase access to PR. Our consultations with patients and HCPs suggest that users are interested in technology and want to ensure it recreates the important aspects of PR. The critical elements of PR were identified as the social aspect, opportunity to communicate with HCPs, monitor bioparameters, and have individualized care that evolves with individuals’ progress. The technical aspects and interdisciplinary nature of P-TR raise practical challenges that must be overcome for successful implementation.
The results of this study have implications for the design and implementation of P-TR. Before designing a P-TR program and selecting which exercise and communication devices available on the market will be used, decision makers should determine that the technology supports patient and HCP needs. The opinions and suggestions of patients and HCPs should be the driving force of innovation if P-TR is to succeed in improving health outcomes.
Footnotes
Acknowledgements
We would like to acknowledge the study participants for their interest in discussing their experience in PR and sharing their ideas for telehealth. We would also like to thank Lauren Coxson who assisted with data entry and calculations during her summer student placement.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Canadian Institutes of Health Research [Catalyst Grant e-Health Innovations #316713, 2015]. Drs. Pat G Camp and Christopher J Ryerson are Michael Smith Foundation for Health Research Career Scholars. Dr. Jessica Inskip is supported by a British Columbia Respiratory Rehabilitation Fellowship from the BC Lung Association.