
Abstract
Objective
This study aimed to identify the usefulness and compare three cutoff points of sedentary behavior (i.e., >8.5 h/day in sedentary time [ST], >70% of the awake time spent in ST, and <4300 steps/day) as predictors of all-cause mortality over a 12-years follow-up period in individuals with stable COPD.
Methods
Baseline-only data from 92 individuals with COPD assessed for admission to pulmonary rehabilitation were analyzed.
Results
Cox multivariate regression models identified the cutoff point of ST >8.5 h/day as an independent predictor of mortality after adjusting for confounders (hazard ratio 1.23, 95% CI 1.021 – 1.589, P = 0.02). The other two cutoffs were not significant.
Conclusion
Among different cutoffs indicating sedentary behavior, ST >8.5 h/day was identified as an independent indicator of higher mortality risk in a 12-years follow-up period in individuals with stable COPD, indicating a 23% higher mortality risk in comparison to those who present ST <8.5 h/day.
Introduction
Individuals with chronic obstructive pulmonary disease (COPD) are frequently characterized by marked physical inactivity and sedentarism. 1 Sedentary time (ST) refers to activities requiring very low levels of energy expenditure (i.e., <1.5 METs), characterized by prolonged periods of sitting, reclining or lying down. 2 In individuals with COPD, ST corresponds to the majority of the day and has been described as an important predictor of mortality, since it was shown that spending >8.5 h/day or >70% of the awake time in sedentary behavior (SB) increased significantly the mortality risk in a 5-years follow-up. 3 Furthermore, step count is also a valid indicator for identifying SB in individuals with COPD, with those walking fewer than 4300 steps/day classified as sedentary. 4 Although these cutoffs have been previously used, it remains unknown which of them is able to predict mortality risk in a longer-term follow-up in individuals with COPD. Hence, the aim of this study was to identify the usefulness and compare different cutoff points of SB (i.e., >8.5 h/day, >70% of the awake time or <4300 steps/day) as predictors of mortality in individuals with COPD over a 12-years follow-up period.
Methods
A retrospective study was conducted comprising baseline-only data from individuals with COPD assessed for admission in two institutional pulmonary rehabilitation programs, with data collected from January 2012 to March 2019. Both studies were approved by the institutional Committee for Ethics in Human Research.
Inclusion criteria were: diagnosis of COPD according to the GOLD 5 ; not having performed regular physical training in the 12 months preceding inclusion; clinical stability defined as the absence of exacerbations within the last month; and not presenting conditions that could interfere with the assessment protocol (e.g., orthopedic, rheumatological, neurological or cardiovascular severe comorbidities). Individuals were excluded in case of unavailability of at least four valid assessment days of activity monitoring; a valid day was defined as >480 min (i.e., >8 h) of wear time/day. 6
SB was objectively assessed using the SenseWear® armband activity monitor (BodyMedia, USA) during awake time for seven consecutive days. Vital status was verified through the Center for Information on Mortality, which registers all deaths in the municipality. The study outcome was all-cause mortality.
Normality in data distribution was evaluated using the Shapiro-wilk test. Student’s t-test or Mann-Whitney U test were used to compare differences between the groups of survivors and non-survivors, whereas the Chi-square test was used for the comparison between survivors and non-survivors classified as sedentary and non-sedentary according to three SB cutoff points. Receiver operating characteristic (ROC) curves were used to determine the best sensitivity and specificity of the three SB cutoffs to predict mortality, whereas the standard error and confidence interval of ROC curves were also compared. Kaplan-Meier curves with the log-rank tests were used to analyze survival differences over time according to each SB cutoff. Cox proportional-hazard regressions were used to estimate survival probability of each cutoff (univariate); after confirming the absence of collinearity, models were adjusted for sex, age, FEV1 and time spent/day in moderate-to-vigorous physical activity (multivariate). SPSS 30.0 (IBM, USA) and GraphPad Prism 8.0 (GraphPad Software Inc., USA) softwares were used, and significance level was P < 0,05.
Results
Baseline characteristics of the sample.

Data are presented as mean ± SD or median (interquartile range 25-75%) according to the normality in data distribution. BMI: body mass index; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; 6MWT: 6-min walk test. ST: Sedentary time. Comparison analyses baseline characteristics between survivors and non-survivors were performed by Mann-Whitney or Student’s t-test, according to the normality in data distribution.
Comparison between survivors and non-survivors classified as sedentary and non-sedentary according to three cutoff points.
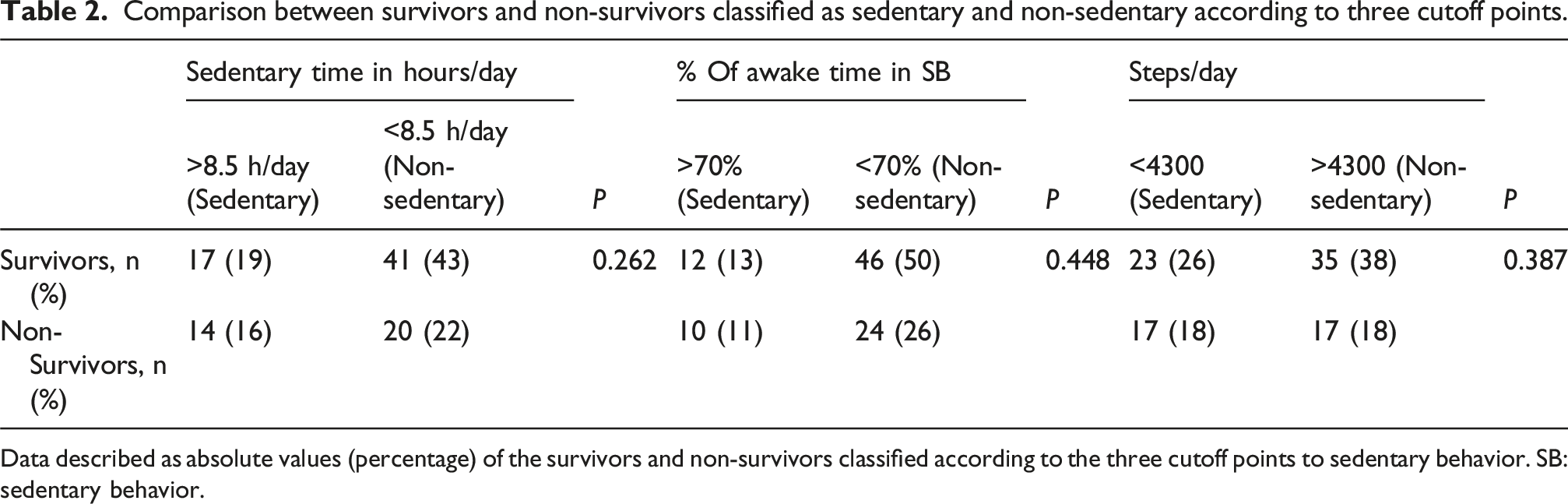
Data described as absolute values (percentage) of the survivors and non-survivors classified according to the three cutoff points to sedentary behavior. SB: sedentary behavior.
For the ST >8.5 h/day cutoff, the area under the ROC curve (AUC) was 0.632 (95%CI 0.510 – 0.754), P = 0.03; sensitivity 41% and specificity 71%. For the cutoff >70% of the awake time, AUC was 0.602 (95%CI 0.478 – 0.727), P = 0.10; sensitivity and specificity 29% and 81%, respectively. Finally, for the <4300 steps/day cutoff, AUC was 0.620 (95%CI 0.499 – 0.742), P = 0.05; sensitivity 58% and specificity 65%. However, when comparing the ROC curves, no significant differences were found between the three SB cutoffs (P > 0.05 for all). Figure 1 shows the Kaplan-Meier curves, with log-rank test comparison for each cutoff over the 12-years follow-up period. Despite considerable visual differences in the survival curves, only borderline non-significant differences were found, which may reflect a lack of sample power. Kaplan-Meier figure of cumulative survival with the log-rank test as separated according to sedentary behavior cutoffs. A) sedentary time >8.5 h per day; B) > 70% of the awake time spent in sedentary behavior; C) < 4300 steps/day.
The Cox regression models identified the cutoff point of ST >8.5 h/day as an independent predictor of mortality after adjusting for confounders (hazard ratio 1.23, 95%CI 1.021 – 1.589, P = 0.02). Each additional hour of SB is associated with a 23% increase in mortality risk. The other two SB cutoff points were not significant. A post-hoc power analysis, based on a moderate effect size (ES = 0,5), estimated the statistical power as 63%.
Discussion
This was the first study to compare cutoff points of SB associated with all-cause mortality over a 12-years follow-up period in subjects with COPD. The identification of useful cutoff points is essential since SB is a strong predictor of all-cause mortality.3,7 They may help identifying modifiable factors that can potentially influence SB, therefore guiding interventions aimed at reducing prolonged periods in ST.8,9
The cutoff point of ST >8.5 h/day has previously shown an AUC of 0.76 in a median follow-up of 5 years. 3 The present findings describe somewhat lower AUC values in the longer-term, although this cutoff showed the highest AUC among the three tested here, and it was the only one which significantly predicted mortality in the Cox regression, after adjusting for confounders (although data on exacerbations and changes in SB over time were not considered). Nevertheless, the present results reinforced the potential of ST >8.5 h/day as predictor of long-term mortality in individuals with COPD. On the other hand, no significant differences were observed between these three cutoff points in terms of confidence intervals and standard errors of the AUC. Moreover, visual analysis of the ROC curves seems to indicate potential in the other two cutoff points as well, therefore suggesting that the study could have been underpowered. These aspects provide reasonable perspectives for future larger studies focusing on these cutoffs, including steps/day. This is a simple PA variable measured by most wearables, which has been classically used to reflect physical inactivity rather than SB, although it has been recently shown to account for 53% of the variation in ST. 10 Finally, a word of caution is required concerning generalizability of the results, since this was a sample referred for pulmonary rehabilitation, which may not reflect the overall population with COPD.
Conclusion
Despite similarities among results of the three cutoff points and their usefulness, the regression analyses showed the cutoff of sedentary time >8.5 h/day as an independent indicator of higher mortality risk in a 12-years follow-up period in individuals with COPD.
Footnotes
Acknowledgments
We are grateful to the colleagues of the Laboratory of Research in Respiratory Physiotherapy for the contribution to the study. In addition, we acknowledge the patients who participated in this investigation. We acknowledge the support of Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Fundação Nacional de Desenvolvimento do Ensino Superior Particular (FUNADESP), Brazil, in the form of individual grants to the authors LS, HS, TMT, LM, KCF and FP.
Ethical considerations
The two projects involved in this study were approved by the institutional Committee for Ethics in Human Research (number 123/09 and number 1.730.247).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.