
Abstract
Background
Health inequalities can affect access and uptake to pulmonary rehabilitation (PR). An individual’s protected characteristics (age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex and sexual orientation) may contribute to health inequalities. Healthcare professionals (HCPs) experiences of the inclusivity and representativeness of PR services and knowledge of protected characteristics are unknown, however are vital for the identification and resolution of health inequalities. This qualitative study explored HCPs understanding of protected characteristics and their perception of the inclusivity, representativeness and equitable benefit of their PR services.
Methods
Semi-structured qualitative interviews were conducted in person or via videoconferencing with HCPs involved in PR from two healthcare providers. Interviews were analysed using reflexive thematic analysis.
Results
12 interviews were conducted with physiotherapists (n = 6), occupational therapists (n = 2), nurses (n = 2) and exercise physiologists (n = 2). Participants had a median (IRQ) age of 43 (13) and 75% (n = 9) were female. Four themes were generated. 1: ‘I don’t really know as much as I should’ [about protected characteristics]; 2: It’s uncomfortable collecting protected characteristics…; 3: ‘I don’t think [service users] are as representative as they could be’; 4: A conventional rehabilitation programme does not meet the needs of all.
Conclusions
This study highlighted several challenges in HCPs understanding of protected characteristics and the representativeness of PR that must be addressed to ensure equity. Strategies, to understand barriers in accessing PR that limit representativeness should be explored.
Keywords
Introduction
Pulmonary rehabilitation (PR) is a highly evidence-based intervention consisting of exercise and education that is gold standard for individuals with chronic respiratory disease.1–3 UK guidance has recently suggested extending PR services to include other conditions such as long COVID and heart failure. 3 It is recommended to offer PR to those that have a diagnosis of these conditions and experience breathlessness (Medical Research Council Dyspnoea score of ≥2).
These services in the UK, delivered by the National Health Service (NHS) are required to offer a comprehensive service for all individuals regardless of their protected characteristics. 4 Protected characteristics are characteristics of an individual that are illegal to discriminate against as a result of the UK Equality Act 2010. 5 The characteristics are age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race (which includes ethnicity), religion or belief, sex and sexual orientation. 5 Protected characteristics are UK specific; however, many other countries have similar legislation.5–13
Knowledge of an individual’s protected characteristics (or equivalent) can facilitate assessment of health inequalities.14,15 Health inequalities are unfair, avoidable and systematic differences in individuals’ health status, access, experiences and outcomes of healthcare 16 and are a major priority for healthcare providers globally.17–19 Health inequalities are driven by systemic factors, 20 often resulting in individuals with certain characteristics experiencing greater inequality. A recent NHS England statement on health inequalities encouraged the collection of data, including some protected characteristics (age, ethnicity and sex), to ensure groups experiencing health inequalities can be identified and assist service development to increase inclusivity and representativeness. 15 Recent scoping reviews found that protected characteristics and social determinants of health are not reported or are inconsistently reported in PR studies, resulting in health inequalities in this area remaining unclear.21,22 This is despite characteristics including age, deprivation, disability, gender, race/ethnicity and sex being shown to impact access, completion and outcomes of PR.3,23–33 The lack and inconsistency of reporting protected characteristics may be due healthcare professionals (HCPs) limited understanding of protected characteristics and their implications.
Currently, there is no research exploring PR HCPs knowledge of protected characteristics and their experiences of the inclusivity, representativeness and equitability of PR. Without this, services cannot accurately assess health inequalities and programmes cannot be effectively adapted to meet the needs of under-represented groups.
Therefore, the aim of this study was to explore HCPs understanding of protected characteristics and their perception of inclusivity, representativeness and equitable benefit of their PR services.
Methods
This study has followed the COREQ reporting framework for qualitative research 34 Ethical approval was granted by the University of Leicester Research Ethics Committee [reference:35782].
Sampling
A purposive sampling approach was used with all qualified healthcare professionals (exercise physiologists, nurses, occupational therapists and physiotherapists) involved in PR at two centres (University Hospitals of Leicester NHS Trust (UHL) and Leicestershire Partnership Trust (LPT), Leicester, UK) eligible for the study. Participants from UHL were peripherally known to the interviewer as they were part of the same institution but different departments. There was no prior relationship with participants from LPT. Potential participants were approached by email in January 2023. Recruitment ceased once all eligible participants had been contacted and a representative sample was recruited.
Data collection
Semi-structured interviews were conducted in person or via Microsoft Teams (based on participant’s preference) by one interviewer (HD), a female physiotherapist trained in qualitative interviewing. Interviews were chosen to allow an in-depth exploration of participants’ experiences of inclusivity, representativeness and equity in PR, which may be considered a sensitive subject. Only the participant and the interviewer were present during the interview. Participants were aware the study aimed to assess and improve health inequalities. The pilot tested topic guide covered knowledge of protected characteristics, the protected characteristics of service users attending PR services and the perceived equity of PR benefit (Supplement A). After discussing participants’ knowledge of protected characteristics, a list was provided for the remainder of the interview. Field notes were made during interviews. Interviews were audio-recorded and transcribed verbatim.
Data analysis
The transcripts were analysed using Microsoft Word and Microsoft Excel following the stages of reflexive thematic analysis outlined by Braun and Clarke (familiarisation with the data, coding, generation of initial themes, development and review of themes, refining, defining and naming themes and writing up) 35 using a phenomenological theoretical framework. Inductive coding was performed independently by two researchers (HD & MWO) to provide an alternative standpoint and themes and quotes discussed with the study team. Reflexive diaries were documented throughout the analysis process to reflect on how personal perspectives and social standpoints may shape the knowledge produced. These included reflecting on how the interviewers’ experience as a clinician allowed them to listen to participants with empathy and understanding.
Results
A summary of the protected characteristics of participants.
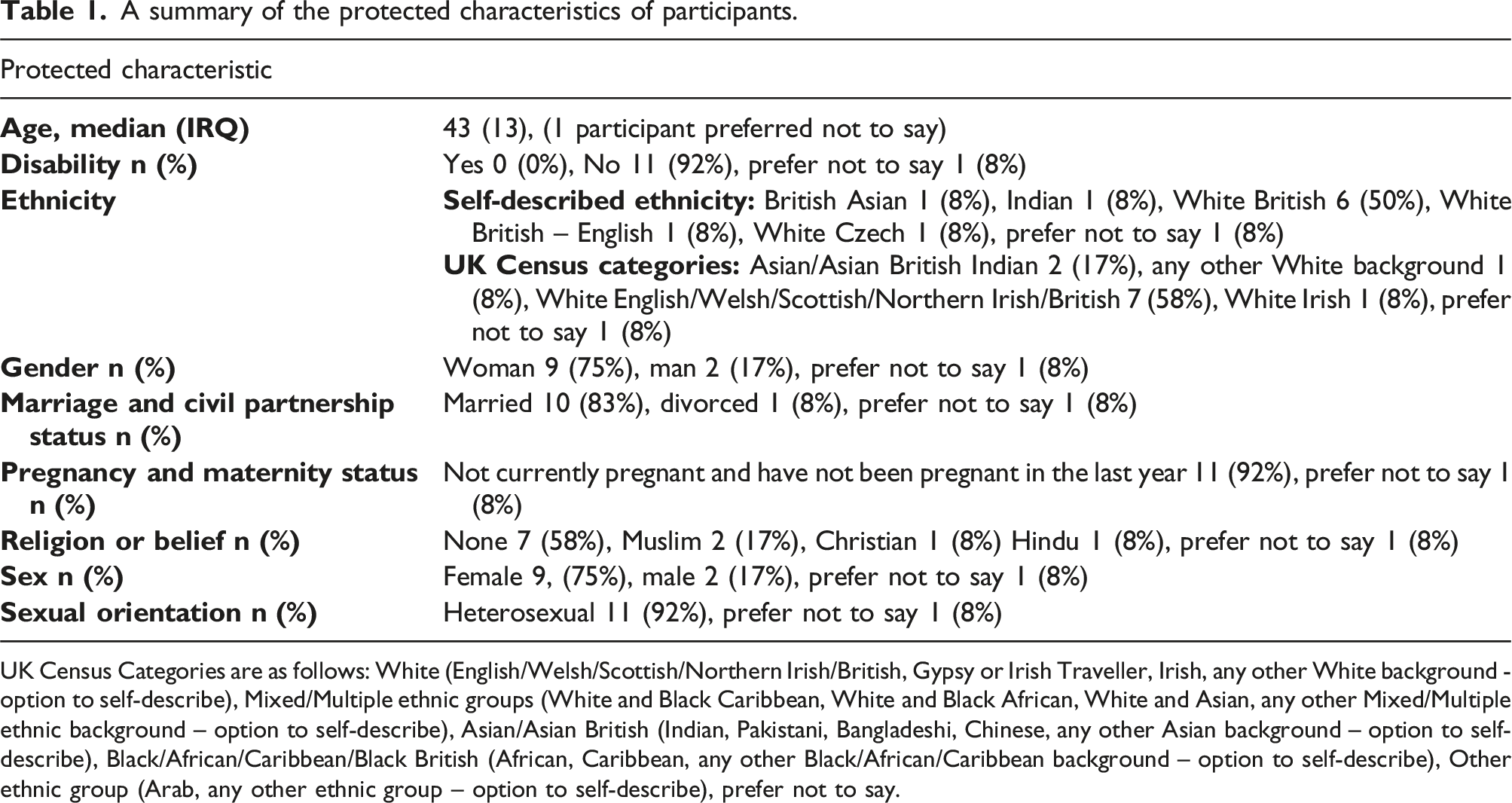
UK Census Categories are as follows: White (English/Welsh/Scottish/Northern Irish/British, Gypsy or Irish Traveller, Irish, any other White background - option to self-describe), Mixed/Multiple ethnic groups (White and Black Caribbean, White and Black African, White and Asian, any other Mixed/Multiple ethnic background – option to self-describe), Asian/Asian British (Indian, Pakistani, Bangladeshi, Chinese, any other Asian background – option to self-describe), Black/African/Caribbean/Black British (African, Caribbean, any other Black/African/Caribbean background – option to self-describe), Other ethnic group (Arab, any other ethnic group – option to self-describe), prefer not to say.
Four themes were generated from the interviews: (1) “I don’t really know as much as I should” about protected characteristics; (2) It’s uncomfortable collecting protected characteristics…; (3) “I don’t think [rehabilitation service users] are as representative as they could be”; (4) A conventional rehabilitation programme does not meet the needs of all (Figure 1). A visual representation of the themes and sub-themes.
Theme 1: “I don’t really know as much as I should” about protected characteristics
Additional quotations for Theme 1.

Subtheme 1.1: Limited knowledge of protected characteristics
The majority of participants reported that they had limited, or inaccurate knowledge of the purpose of protected characteristics:
that’s completely new for me [participant 1, physiotherapist]
Limited knowledge was particularly evident around gender reassignment and marriage and civil partnership, with some participants surprised that marriage and civil partnership was a protected characteristic:
marriage and civil partnerships are actually a bit of a surprise… I wouldn’t have thought that that would have been one [participant 10, physiotherapist]
Several participants were unsure of the classification of disability as the protected characteristic:
when you say disability…does that include physical and psychological? We ask about physical disabilities, we ask, do they feel that they have a disability or not? [participant 10, physiotherapist]
Limited knowledge may have led to some participants voicing misunderstandings about protected characteristics including that they are a ‘new’ concept and a misunderstanding of sex and sexual orientation:
we’re going to add in [collecting] these characteristics because we believe that times are changing [participant 2, nurse]
is there a difference between sex and sexual orientation? [participant 9, physiotherapist]
Despite these misunderstandings, there was an evident appetite from HCPs to develop their understanding on this topic:
I think that’s [protected characteristics] something that we need to learn more about as a team…I’ve asked if someone could do some training [participant 12, occupational therapist]
Subtheme 1.2: Assuming the protected characteristics of service users
Some participants reported that they tended to assume service users’ protected characteristics. These are often collected as part of a telephone assessment which may have contributed towards this. Assumptions occurred for race and gender reassignment:
where it [race] is a bit obvious, I go with what is on the [healthcare] system [participant 1, physiotherapist]
I tend to just assume that they are, their sex is from birth, their gender from birth [participant 3, exercise physiologist]
Assumptions about service users’ protected characteristics may occur due to them expressing frustration that this information had been repeatedly collected, potentially perpetuating hesitancy of HCPs to ask:
“they [service users] start telling you I saw this nurse, she was questioning all this [protected characteristics]. Then it was the doctor coming…he asked me the same questions…then it was the senior doctor supervising who came and started all over again. Why do we have to collect the data that has been already collected [participant 1, physiotherapist]
Assumptions may also have occurred as HCPs felt uncomfortable asking the protected characteristics of service users, which is detailed in the next theme.
Theme 2: It’s uncomfortable collecting protected characteristics…
Additional quotations for theme 2.
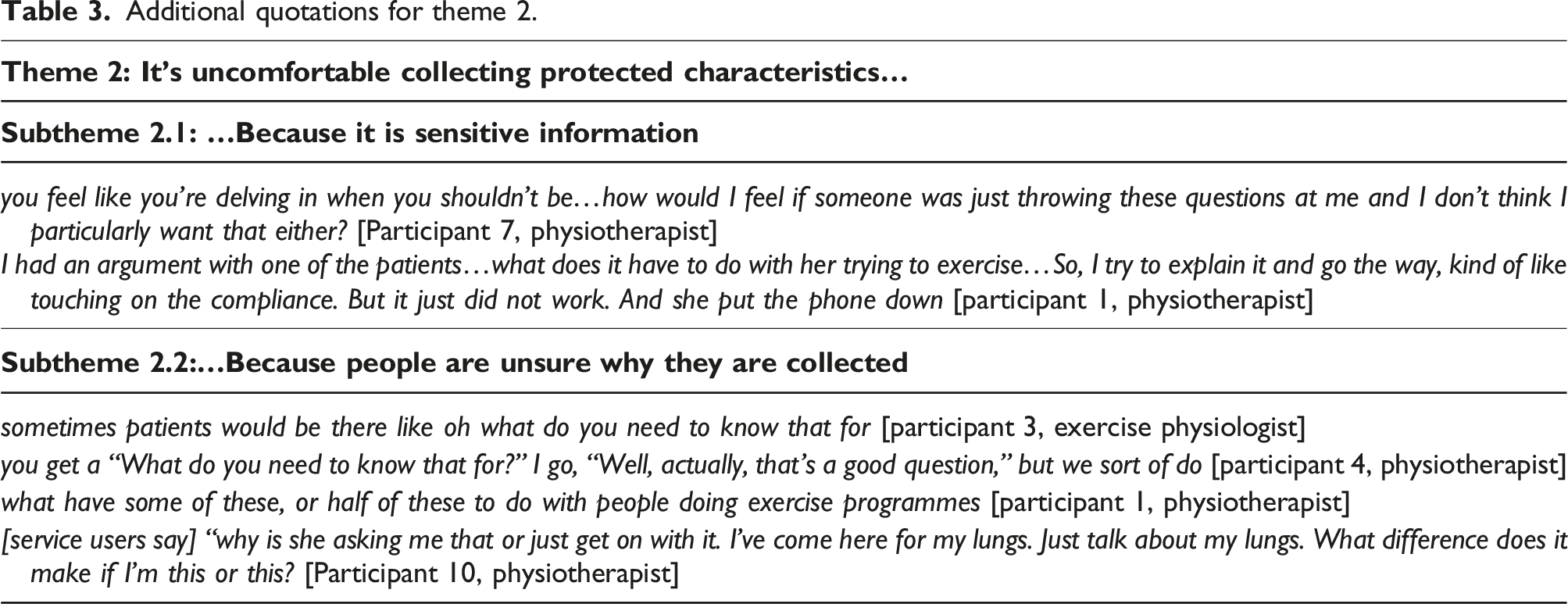
Subtheme 2.1: …because it is sensitive information
This subtheme explored participants experiences of discomfort when asking service users their protected characteristics:
I wouldn’t say I will feel comfortable doing it but I do it [participant 9, physiotherapist]
This was particularly evident when asking perceived ‘intrusive’ characteristics for example, sexual orientation and gender reassignment:
If I were attending something like a rehab programme and somebody said to me, you know, “Are you heterosexual?” ...I’d say, “Well, what business is it of yours? [participant 4, physiotherapist]
you don’t normally look at a stranger and suddenly ask them about their gender reassignment…that seems quite- like intrusive [participant 7, physiotherapist]
Several participants reported that they perceived this discomfort resulted in service users terminating of their appointment:
If it is a more sensitive subject, it closes the whole conversation and they might not want to then enrol in the programme [participant 3, exercise physiologist]
Although this concern was raised by several participants, it is unknown whether all participants had experienced this, however it appeared to significantly impact the participants’ experiences and cautions around collecting protected characteristics. The perception of service users choosing to not uptake PR due to the collection of protected characteristics may impact how HCPs ask these questions to future service users.
Subtheme 2.2: …because people are unsure why they are collected
The subtheme of ‘…because people are unsure why they are collected’ describes HCPs not understanding the reasons for collecting protected characteristics and feeling uncomfortable justifying this to service users:
it's just to collate information…that's how I kind of get out of it, it usually works…some people kind of give me a bit of a dodgy look…I don't want them to think of me differently [participant 10, physiotherapist]
However, HCPs were more likely to collect protected characteristics if they knew why they were collected:
if you’re aware that that information is being used to benefit the service then you're more likely to collect all that data [participant 11, occupational therapist]
HCPs experienced service users querying the collection of characteristics, though an explanation often improved perceived service user comfort:
as long that [why protected characteristics are collected] was relayed to the patient and they understood that, you know, this is why we collect this information, then most people I think would be fine [participant 5, exercise physiologist]
Most participants, and some service users, did not perceive protected characteristics as clinically relevant, particularly marriage and civil partnership and sexual orientation:
I can’t imagine that whether they’re married or in a civil partnership’s going to have any bearing on them- on us [participant 8, physiotherapist]
sexual orientation? ... it doesn't seem hugely important in terms of their rehab [participant 12, occupational therapist]
[service users say] “Why are you asking? What’s that got to do with my COPD?” [participant 7, physiotherapist]
Theme 3: “I don’t think [rehabilitation service users] are as representative as they could be”
Additional quotations for theme 3.
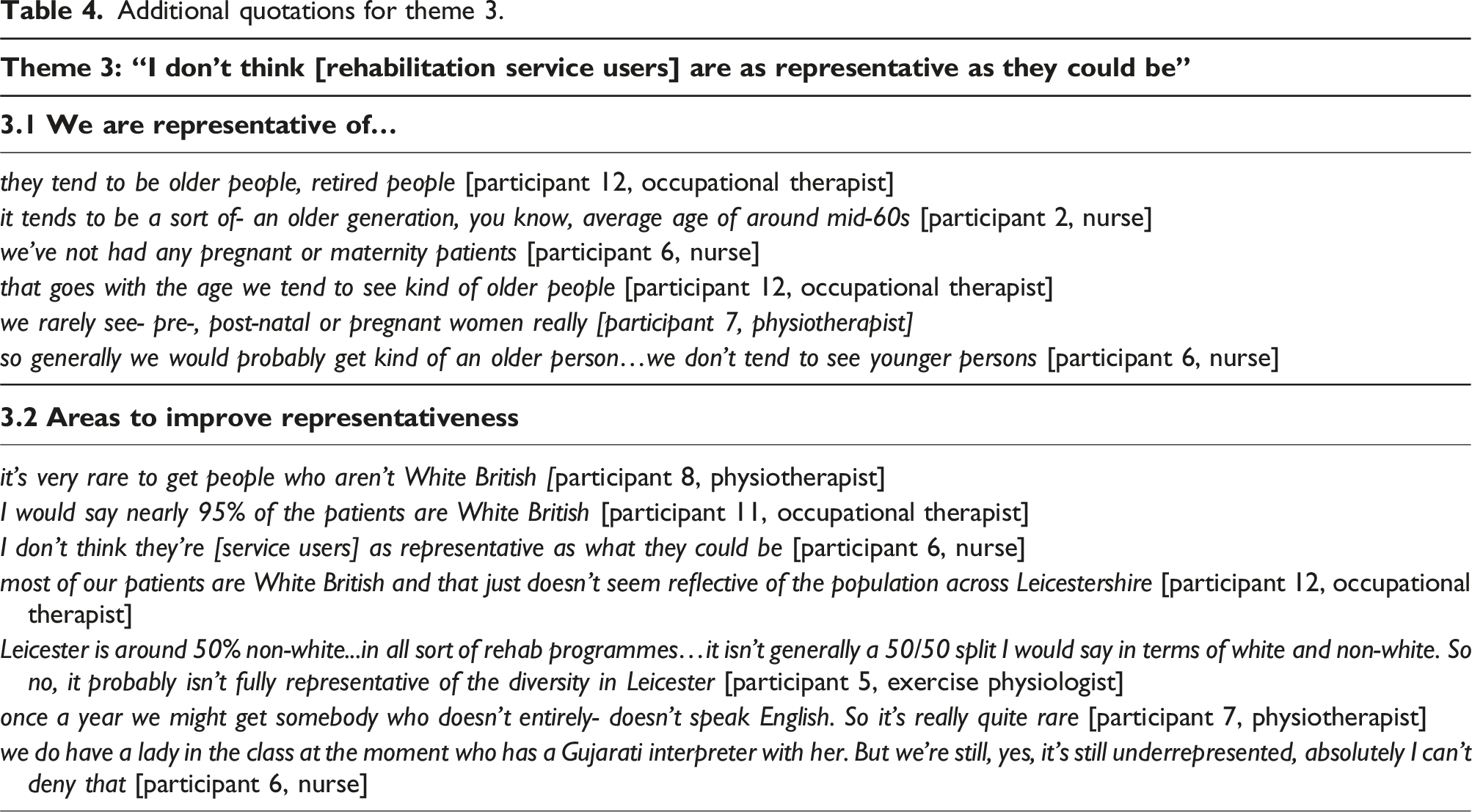
Subtheme 3.1: We are representative of…
The subtheme titled ‘We are representative of…’ covered the participants perceptions that PR was representative of the target population in relation to age and pregnancy and maternity. Most PR deliverers reported that service users were usually older and without the protected characteristic of pregnancy and maternity, but this was representative of the population eligible for PR:
because of the nature of the conditions, they’re usually diagnosed later in life [participant 7, physiotherapist]
zero pregnant or people on maternity leave [participant 8, physiotherapist]
because we have a much older population, you’re not going to see it [pregnancy and maternity] very much [participant 3, exercise physiologist]
Subtheme 3.2: Areas to improve representativeness
This subtheme explored HCPs feelings in relation to under-representation of race and/or ethnicity and the spoken languages within PR services compared to the population they observe geographically.
Participants reported a predominantly White British population with few South Asian service users, which they did not feel was representative of the population of Leicester and Leicestershire:
for the population of Leicester, which is almost like 50/50…against the South Asian…I would say that we’re still seeing mainly White males and females as opposed to South Asian [participant 6, nurse]
They tend to be…more White than you might imagine given where we’re delivering our services [participant 4, physiotherapist]
HCPs displayed uncertainty around services users’ representativeness:
I don't quite know why that's happening, but it doesn't feel like the patients we that we have coming to rehab or are kind of fairly representative of the local populations…it still doesn't feel equitable really across the population [participant 12, occupational therapist]
HCPs reported that service users predominantly spoke English and that this was unrepresentative of the language diversity within the local population:
we have had people before who, again not very often, but where English isn’t their first language…it doesn’t come up often [participant 8, physiotherapist]
Many participants felt that language was a barrier to attending rehabilitation, particularly centre-based rehabilitation:
if any of them don’t speak English or if they don’t have anyone that would translate for them, they tend to not turn up [participant 3, exercise physiologist]
they'd rather uptake take up the programme at home as opposed to classes because obviously in the classes you know they're not sure if there's someone else who can speak the language [participant 10, physiotherapist]
Notably, participants compared a service users’ race, ethnicity and/or language to the local population, however compared a service users’ age or pregnancy and maternity status to the population eligible for PR. This suggests that participants were more confident about age and pregnancy and maternity demographics of those eligible for PR than race, ethnicity and/or language demographics. It is important to consider the demographics of those who are eligible for PR alongside the demographics of the local population, as local population statistics are unlikely to reflect that of the disease population.
The experiences of HCPs in this theme suggested that a conventional rehabilitation programme does not meet the needs of all service users (Theme 4).
Theme 4: A conventional rehabilitation programme does not meet the needs of all
Additional quotations for theme 4.
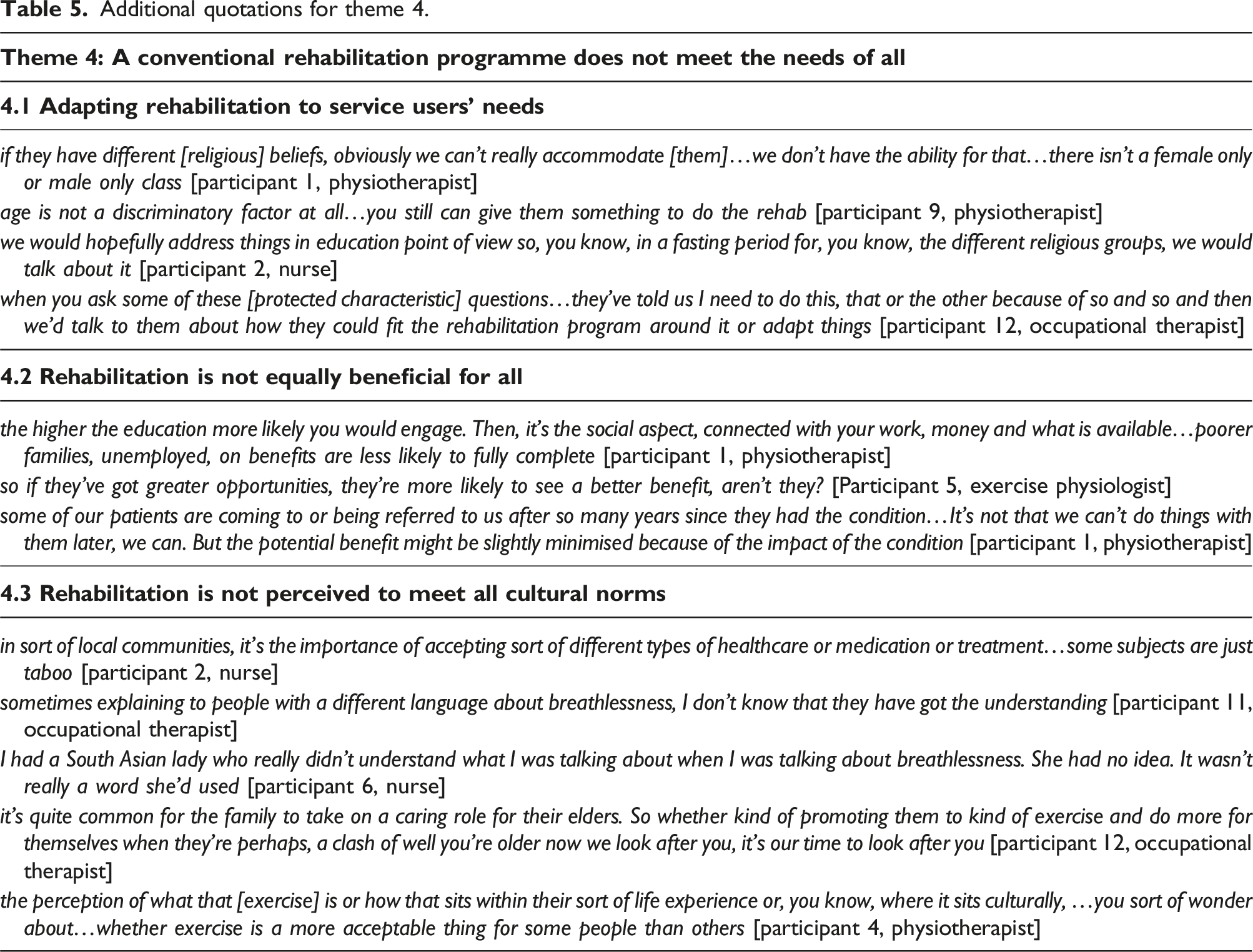
Subtheme 4.1: Adapting rehabilitation to service users’ needs
Participants did not feel that rehabilitation was fully accessible to all as a conventional programme:
with it being exercise-based rehab, there’s a level of ability that they have…you wouldn’t necessarily see many people that would fall under the sort of disability category [participant 5, exercise physiologist]
However, participants did feel that PR could be adapted, particularly for disability:
we make reasonable adjustments for everyone who’s accessing [the service] [participant 6, nurse]
people come in obviously, you know, walking aids, different mobility issues. Sometimes you end up doing total adaptation to seated programme [participant 9, physiotherapist]
Some participants felt that collecting protected characteristics provided an opportunity to measure if PR is accessible for all and make adaptations for under-represented groups based on this:
you can monitor that people are not being excluded to get an idea of who's accessing the services. So we can see…you're not excluding certain groups completely. And plan services as well around what's needed [participant 11, occupational therapist]
Subtheme 4.2: Rehabilitation is not equally beneficial for all
Participants did not believe that PR was equally beneficial for all service users. For example, HCPs did not perceive all service users to have equal opportunities to exercise outside of sessions which resulted in unequal improvements:
it might come down to opportunities to exercise outside of coming to the sessions as well...if you are someone that comes from a certain background [lower socioeconomic status], you might have more chance to stay active…whereas other people that session that they attend with us might be the only chance that they get [participant 5, exercise physiologist]
Although it is not a protected characteristic, participants also expressed views that socioeconomic status impacts PR outcomes:
it makes a difference when people are educated. They can take on board the education… often, they'll go out and buy some exercise equipment so they can carry on exercising at home [participant 11, occupational therapist]
Subtheme 4.3: Rehabilitation is not perceived to meet all cultural norms
This final subtheme explored HCPs perceptions that PR may not meet cultural norms. Several participants discussed their perceptions that accessing management may be more difficult in certain cultures:
for the female part in the Asian population where it would be typical at that age…it’s the woman running the house…we may not get as many of those patients because they will still irrespective run the house [participant 1, physiotherapist]
Participants also discussed that cultural perceptions and understanding of breathlessness may vary by language and ethnicity:
it’s sometimes maybe lost in translation as to the severity of their breathlessness…some patients, because of their condition, will push themselves only so far and think this is it. I must stop because it’s brought on a sensation of breathlessness [participant 3, exercise physiologist]
The perceptions of the acceptability of exercise in different cultures was discussed by HCPs. Many participants believed that exercise was less acceptable in certain cultures than others:
I come from an Asian background, so culturally if I asked my mum to exercise, it wouldn’t happen…culture has a huge influence because they feel it’s wrong to do something deviated from the normal [participant 9, physiotherapist]
This meant that the conventional exercise-based programmes were not perceived to meet the needs of all cultures.
Discussion
This qualitative study has explored HCPs understanding of protected characteristics and their perceptions of the inclusivity, representativeness and equitable benefits of PR within Leicestershire. Participants had limited knowledge resulting in discomfort when assessing protected characteristics, however intended to increase their knowledge. Limited knowledge may lead to misunderstandings and assumptions of service users protected characteristics. Training for HCPs could improve the understanding and assessment of protected characteristics in relation to health inequalities.36,37 Training sessions could include importance and approaches of data collection, how to analyse the data to support service improvement and communicating to service users. 38
Unease experienced by HCPs and perceived discomfort experienced by service users when collecting protected characteristics was frequently discussed by participants. A recent scoping review identifying approaches in healthcare for monitoring health inequalities reported that staff were reluctant to collect health inequality data (including protected characteristics). 39 Comparatively, this was a result of staff reluctance due to a lack of knowledge and concerns of causing offense. 39 Participants viewed sexual orientation and gender reassignment as particularly sensitive information, but research has shown that the majority of service users are comfortable answering these questions within healthcare.40,41 All characteristics add value in assessing health inequalities, and the ways to address them. 42
Most participants perceived that the majority of service users identified as White British which they felt was unrepresentative of the local population. In Leicester (UK), 33.2% of the population identifies as White English/White Welsh/White Scottish/White Northern Irish/White British compared to the national average of 73.5%. 43.4% identify as Asian/Asian British/Asian Welsh compared to the national average of 9.7%. 43 The perception that the majority of service users attending PR were White British is consistent with the UK National Respiratory Audit Programme’s (NRAP) report that 82.5% of service users attending PR are White British 32 ; though this report includes data on people with Chronic Obstructive Pulmonary Disease (COPD), which is predominantly diagnosed in White British individuals 44 and underdiagnosed in ethnic minority groups.45,46 There is a reported underdiagnosis of respiratory diseases among non-White individuals due to race adjustment equations in pulmonary function tests47,48 and access to healthcare.45,46 In one study in London (UK), the prevalence of diagnosed COPD was 1.55% in White individuals, 0.78% in Asian individuals and 0.58% in Black individuals 44 which may present a barrier to referral to PR. However, within UHL access to PR is not dependent on a diagnosis which should improve access to this key intervention. Similarly, in New Zealand and the United States, Maori and Black individuals are significantly less likely to attend PR than European and non-Hispanic White individuals respectively.25,33,49 The differences in attendance could not be accounted for using regional variation in service provision. 25 Several studies suggest ethnic concordance between service users and HCPs may increase a service users’ trust and comfort,50–52 potentially making a service user more likely to attend PR. This suggests strategies such as adapting programmes for under-represented service users and striving for a diverse workforce may be needed to improve the representativeness of PR.
Several participants discussed their perceptions that PR is not inclusive for all, particularly in relation to the cultural acceptability of exercise. An individual’s culture includes their values, beliefs and conventions that influence their behaviour and are shared by a group of people. 53 Exercise is key component of rehabilitation; however, it has been reported that in South Asian communities, exercise can be perceived as detrimental to an individual’s reputation,54–56 and impacting family honour, whereby beliefs prioritise family duties over independence and exercise.54–56 This suggests adaptations to optimise cultural accessibility are required to ensure inclusivity for all, whilst maintaining effectiveness.
This study recruited participants from two NHS trusts in Leicestershire (UK), therefore, the experiences of the HCPs in this study are not transferrable to HCPs at other NHS trusts, or in different countries. However, whilst HCPs experiences will differ depending on location, health inequalities are a global challenge and therefore this work could offer insight into potential challenges. Although this study focused on protected characteristics, there are additional health inequalities that should also be considered, such as socioeconomic status, and some protected characteristics that may be less influential in the context of PR. Frameworks such as INCLUDE 57 and the allied health professionals health inequality action framework 58 may support the exploration of the most relevant health inequalities. The sample consisted of 75% of the eligible population and included a range of professions working in PR, widening the scope of experiences explored. Participants consisted of predominantly White, female participants without a disability and although this reflects the demographics of the professions interviewed,59,60 it may have resulted in similar positionality, views and experiences. To increase the rigour of the study, codes and themes were discussed with the study team to reflect on data that may have been overrepresented or overlooked. Though these findings have limited transferability, they highlight the importance of protected characteristics, and supporting HCPs to explore these in a way that is safe and acceptable in order to evaluate health inequalities.
In conclusion, this qualitative study has highlighted several challenges in HCPs knowledge and understanding of protected characteristics and the inclusivity and representativeness of PR that must be addressed to ensure equity for individuals eligible for PR. Participants reported a limited knowledge of protected characteristics, therefore education sessions for HCPs to improve their understanding, communication to service users and data analysis to support service improvement could be beneficial. Conventional PR programmes were not viewed to be representative of the local population or inclusive of all eligible service users by HCPs. Strategies to understand barriers in accessing PR that limit representativeness should be explored to improve the inclusivity and representativeness of PR.
Supplemental Material
Supplemental Material - Pulmonary rehabilitation healthcare professionals understanding and experiences of the protected characteristics of service users: A qualitative analysis
Supplemental Material for Pulmonary rehabilitation healthcare professionals understanding and experiences of the protected characteristics of service users: A qualitative analysis in China by Holly Drover, Sally J Singh, Mark W Orme and Enya Daynes in Respiratory Disease.
Footnotes
Acknowledgments
The authors would like thank the healthcare professionals for their time given when participating in the interviews. We also thank Dr Amy Barradell for her insight into analysing interview data.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H. Drover reports a role as NRAP Honorary Clinical Fellow on the Pulmonary Rehabilitation workstream. S.J. Singh reports roles as NIHR Senior Investigator, NRAP Clinical Lead for the Pulmonary Rehabilitation workstream and Editorial Strategy Board of Chronic Respiratory Disease. M.W. Orme reports a role on the Editorial Review Board of Chronic Respiratory Disease. E. Daynes reports lecture honoraria from Clinical Physio, honoraria from Neuroscience and Mental Health Institute (funding committee 2023) and roles with the BTS as chair of the Pulmonary Rehabilitation Specialist Advisory Group, Lead Expert Member NICE HTA EVA for Digital Rehabilitation, ATS Pulmonary Rehabilitation Assembly committee member, NRAP steering group, PRSAS steering group, CAHPR East Midlands Hub Lead, NIHR HS&DR funding committee member and Associate Editor of Chronic Respiratory Disease.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Wellcome Trust [204801/Z/16/Z] and as part of the Leicestershire Health Inequalities Improvement Doctoral Training Programme [223512/Z/21/Z]. This study is supported by the National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre (BRC). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.