
Abstract
Keywords
Introduction
Pulmonary rehabilitation (PR) is the primary non-pharmacological treatment recommendation for people with chronic respiratory disease.1,2 A program of exercise and education, underpinned by robust evidence, PR is typically undertaken in a group setting at a healthcare centre over 8-12 weeks. It effectively improves symptoms and function and reduces healthcare utilisation. 3 However, despite robust evidence to support its use and the high burden of chronic respiratory diseases, a lack of available programs 4 together with significant patient-related barriers to attendance 5 means PR is grossly underutilised globally. 2
Models of care that deliver PR remotely (i.e. telerehabilitation, rehabilitation delivery at a distance using information and communication technology (ICT) 6 ) have been demonstrated to achieve equivalent clinical outcomes to traditional centre-based models 6 and may reduce barriers to access. These remote models are associated with similar costs to traditional centre-based programs 7 with greater program completion rates (exceeding 90%). 6 Yet, despite the potential for improved PR access with remote delivery, and the clinical, health system and economic benefits ascribed to greater PR access, 8 remote models of rehabilitation are not widely deployed. Clinical guideline recommendations relating to offering remote PR to patients vary in different jurisdictions,2,9 with a preference for centre-based PR as a first line treatment approach. 9 Pre-COVID-19 remote programs were available in just 4% of Australian services 10 and up to 30% of UK-based programs 11 ; post-pandemic, widespread implementation of telerehabilitation for people with chronic respiratory disease remains limited. 12 While patients report benefits associated with telerehabilitation including flexibility of program location, time and cost savings, 13 healthcare professionals indicate a lack of knowledge and confidence to implement and adapt telerehabilitation programs for their local context as key barriers to effective program delivery. 14
Previous research evaluating the real-word implementation of remote PR delivery has been limited to a select number of high-income countries and their health systems,12,15 with applicability in other settings, especially low-middle income countries, unclear. Such single centre evaluations typically do not account for setting context beyond the local organisation, or identify resources that will support and sustain scale-up processes, crucial factors for expanding intervention implementation to settings or populations beyond those initially studied. 16 For telerehabilitation to be delivered on a broader scale, strategies to support program implementation that are applicable across healthcare jurisdictions may help overcome some barriers to the delivery of remote rehabilitation.
Therefore, the aims of the present work were to understand the factors that health professionals, from a variety of healthcare contexts and geographic regions, believed would support remote delivery of PR; and to develop a targeted intervention to support health professionals in the implementation of remote PR across a variety of healthcare settings.
Methods
A participatory action-research process was employed across 3-phases. This allowed for gathering of practical information and perspective, taking action through intervention development, followed by evaluation. 17 Three study hubs were used for targeting participant recruitment across three countries. These countries (New Zealand, India and USA) represent extremes of remote healthcare availability pre-pandemic ranging from ‘limited adoption, with infrastructure issues, and requiring the establishment of public policy’ [India], ‘telemedicine invention stage, but requiring technological sector support’ [New Zealand] to ‘front runner of telemedicine and technological innovation’ [USA] 18 ; although the actual availability of telerehabilitation is not well documented.
The study hubs (Te Whatu Ora Counties Manukau, New Zealand; Manipal College of Health Professions, India; University of Alabama at Birmingham, USA) represented diverse healthcare delivery contexts, specifically: (i) a high income country with a significant burden of chronic respiratory disease amongst First nations people 19 (New Zealand); (ii) a lower-middle income country where chronic respiratory disease is the second leading cause of disease burden and contributes 32% to global respiratory-related disability adjusted life years 20 (India); and (iii) a high income country in a region with high prevalence of diagnosis, hospitalization and mortality due to chronic respiratory disease 21 (USA). Healthcare professionals working in PR at the three study hubs, and their associated professional networks, were sent an email invitation to participate. Individuals who expressed interest in participating were provided with study information from the lead investigator (NSC) and sent an electronic link for completion of the online consent form. Approval for the study conduct and procedures was provided by the Monash University Human Research Ethics Committee (Project ID: 29483).
Phase I: focus groups with health professionals
Hub-specific focus groups with up to 5 healthcare professionals per group were undertaken between September 2021–August 2022. The aim of the focus groups was to understand factors which clinicians, from a variety of healthcare contexts, felt would support implementation of remote PR. A discussion guide was employed (see Table S1), which was piloted with three PR clinicians (1 senior, 2 junior) from the local health service of the lead researcher in a mock online focus group. Focus group sessions were conducted remotely using videoconferencing and recorded for the purposes of transcribing audio content verbatim. Transcripts were coded to ensure that participants could not be identified from their responses. Focus groups were facilitated by one health researcher (NSC, female, PhD qualified) who is an experienced PR clinician with expertise in the delivery of remote rehabilitation, qualitative methodology, and focus group facilitation. There was no prior relationship between the researcher and participants. Participants were provided with a brief verbal biography of the facilitator prior to the commencement of the focus groups, and provided with an outline of the proposed running of the group and the aims of the session. A second researcher (SC, female, physiotherapist) was an observer for two of the focus groups providing additional perspective.
Focus group data were analysed independently by two researchers (NSC, SR) both experienced in the collection and evaluation of qualitative data. Participant quotes were coded against both the Theoretical Domains Framework (TDF) 22 and the Consolidated Framework for Implementation Research (CFIR). 23 The intent of using two coding frameworks was to identify individual-level (primarily TDF) and local organisational-level factors (primarily CFIR) that influence implementation of remote PR. 24 Coding domains within both frameworks are not mutually exclusive, so a quote may be coded across both TDF and CFIR constructs as well as multiple domains within one framework. A random sample of 35% of the data was cross-coded by both researchers, with differences in framework assignment resolved by discussion. Double-coding was undertaken to ensure all focus groups and participants were represented in the data checking, and to establish intercoder reliability. 25
Phase 2: development of intervention to support delivery of remote PR
Using Phase I results, action points were generated for the development of an intervention. These action points were provided to participants in the form of an executive summary. The development of a free, online toolbox was proposed by the researchers, having considered the Phase I data, that would encompass the broad factors considered to support implementation of remote PR across all three healthcare contexts. Feedback was sought via an online poll (QualtricsXM, Seattle, USA) with respect to executive summary content and proposed intervention development. Expert clinician-researchers then developed content for the online toolbox, and study participants were invited to use and review the online toolbox over a 1-month period.
Phase 3: evaluation of intervention
Participants were invited to participate in a semi-structured, individual qualitative interview to provide their perspectives of the online toolbox intervention (https://prtelerehab.com) and reflect on the determinants of implementing a remote model of PR into their practice. Interviews were undertaken via video-conferencing. Audio recordings of interviews were transcribed verbatim. Transcripts were coded to ensure that participants could not be identified from their responses. Interviews were conducted by a healthcare professional (SR, female) with experience in delivering remote PR and qualitative research methodology, who was not involved in study Phase I nor in the development of the online toolbox. The interviewer was also not known to any of the participants prior to interview. An interview guide using opened-ended questions was designed to elicit information (Table S2).
De-identified interview transcripts were analysed by two researchers independently (SR and NSC). Through a process of reading and re-reading, 26 line by line thematic analysis was performed to identify descriptive codes from the data. 27 A data-driven code book was then developed using an initial sample of four interviews, and codes discussed between the two researchers for consistency of interpretation and reliability of application. 28 The code book was employed for the analysis of remaining interviews, with coding being an iterative process whereby additional codes were added, removed or modified, as required, in keeping with a reflexive thematic analysis. 29 As in Phase I, 35% of the data was cross-coded by both researchers to ensure consistency. 25 On completion of data coding, related codes were collapsed to create major themes and subthemes. Themes, and their descriptors, were discussed between the researchers until consensus was reached. Quotations were extracted from the transcripts to provide supportive data for each theme.
Results
Phases I & II: focus groups and intervention development
Participant characteristics.

A total of 616 individual participant quotes were extracted from the focus group transcripts and mapped to the TDF and CFIR as factors considered to influence remote PR delivery. All 12 domains of the TDF, and 5 domains of the CFIR, were represented including at least one quote attributed to each domain (Figure 1, Table 2). Despite participants working across diverse healthcare contexts, the factors considered to influence implementation of remote PR were consistent, and mutually inclusive across the TDF (see also Supplemental Material) and CFIR. Participants quotes coded to TDF domain by barrier and facilitator. Phase I representative quotes by TDF domain.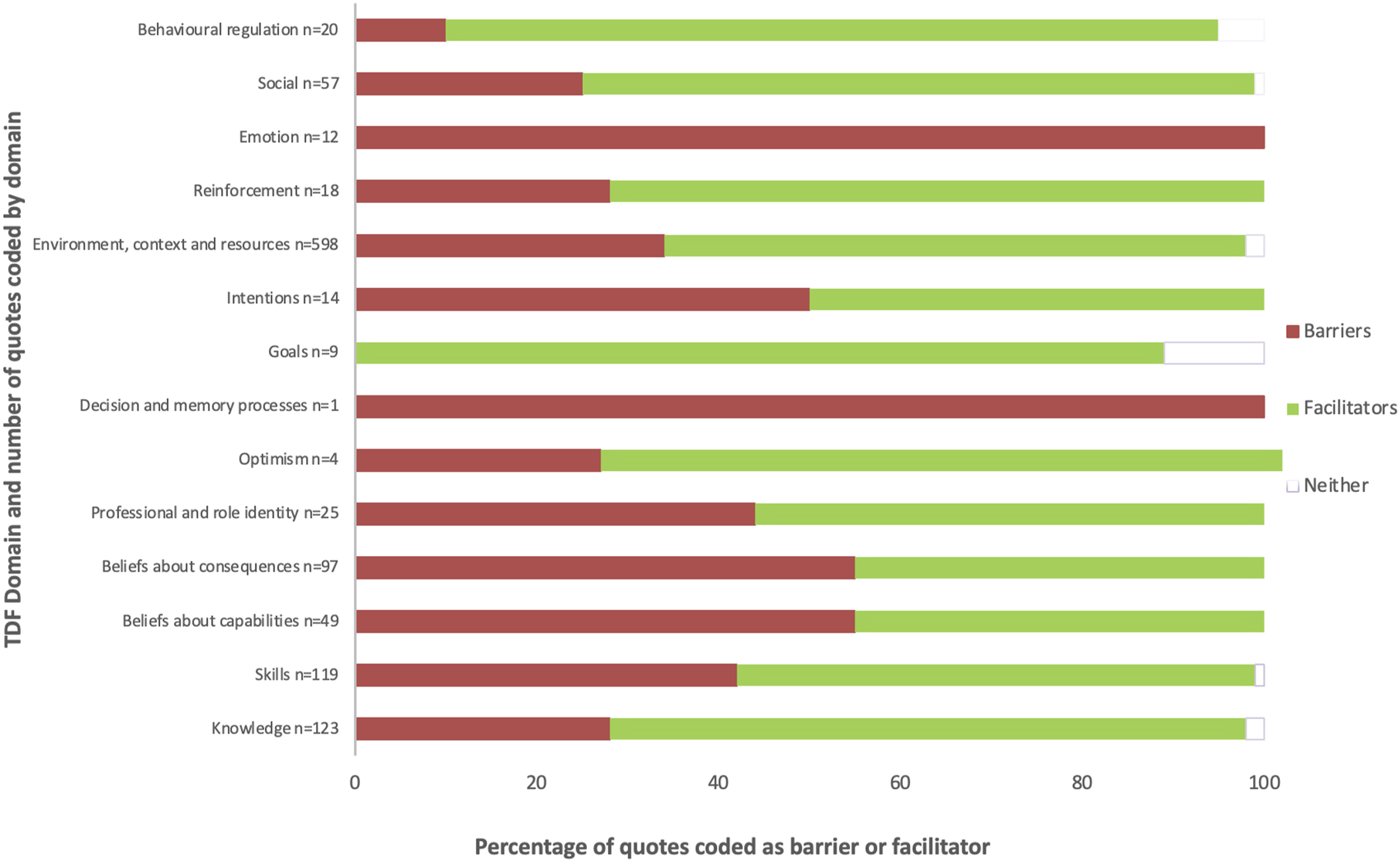

Individual factors associated with delivery of remote PR included sufficient staffing with appropriately experienced personnel. In addition, clinical skills in the management of people with chronic respiratory disease, and PR, were viewed as critical to being able to deliver remote PR effectively and safely. The use of video technology for delivery was felt to improve comfort and confidence of health professionals in their ability to conduct remote exercise sessions, evaluate patients, and monitor safety. Making use of team members or other service providers with previous experience of remote rehabilitation delivery as a learning resource, and ensuring understanding of procedures for managing emergencies or technological issues were key factors to ensuring successful remote delivery. Health professionals identified the need for patients to have an appropriate home environment for exercise, and access to and ability to use relevant technology as crucial.
Organisational factors considered to influence remote PR delivery were adequate program funding or reimbursement, and availability of infrastructure and resources. To support remote PR delivery health professionals would ideally have access to IT support in the form of a ‘technology navigator’ to relieve them of the burden of teaching and troubleshooting technology issues and address the lack of confidence with technology expressed by many participants. Although audio-visual interaction with patients via video was the preferred means of remote PR delivery, it was acknowledged that resources for video interaction were not readily available to all patients or health services.
At the conclusion of the 8 focus groups, no new insights were apparent. An executive summary of these findings was prepared and disseminated to participants for review and feedback (Figure 2). Broad factors considered to support implementation of remote PR across all three healthcare contexts to be considered in toolbox development were categorised as relating to: (i) Equipment – type, availability and use (CFIR domains: Inner, Intervention); (ii) Skills training – for delivery of program components, and using and troubleshooting technology (CFIR domains: Inner, Individual); (iii) Resources – management, financial and practical to support program delivery (CFIR domains: Outer, Inner, Intervention); (iv) Processes – to foster confidence and competence in program delivery and ensure safety (CFIR domains: Inner, Intervention, Process); and (v) Socialisation – considering models that allow for a virtual group environment and visual interaction to create opportunities for peer-support and rapport building (CFIR domains: Individual, Intervention). Executive summary of focus group data mapped to CFIR.
14 participants reviewed the executive summary and provided feedback via the online poll. The concept of an online toolbox to provide clinicians with resources and support for the delivery of remote PR was supported by 93% of respondents. Additional content suggestions included information on assessment strategies, patient monitoring, and locally and culturally adaptable resources.
Phase III: intervention evaluation: individual interviews
The online toolbox (https://prtelerehab.com) was made available to all participants for review. 11 participants (55% total sample) agreed to an interview (New Zealand n = 4, USA n = 2, India n = 4; Physiotherapist/physical therapist n = 7, Exercise Physiologist n = 2, Nurse n = 1). Interview duration was median [IQR] 32 [18 to 46] min and data saturation was achieved.
Individual semi-structured interviews, representative quotes by theme.

All participants reported the toolbox to be easy to use and perceived value for those with and without previous experience of delivering remote PR. The breadth of resources provided, including patient-facing documentation and service development templates as well as links to evidence-based literature, contributed to the perceived comprehensiveness of the toolbox as a training and service development resource. In future toolbox updates, participants recommended language translation capabilities and increased use of video resources as desired content. Despite the perceived usefulness of the toolbox in supporting clinicians to deliver remote PR, participants acknowledged ongoing barriers to remote service delivery including limited staffing resources and variable acceptance of remote rehabilitation by both patients and staff. Although challenges to implementation of remote delivered PR remain, clinicians described future goals for their services to further improve patient access to remotely delivered rehabilitation including offering evening programs and providing individualised coaching within the context of a rehabilitation program.
Discussion
This study reports on factors which healthcare professionals working across different healthcare contexts around the world considered would support the remote delivery of PR. The findings informed the development of a free, online toolbox to support the implementation of remote PR (telerehabilitation). In a group of clinicians, almost all of whom had telerehabilitation experience, key factors that impact delivery of remote rehabilitation were not different across countries. Availability of appropriately skilled staff and sufficient workforce capacity, access to reliable technology and exercise equipment, and resources and support for skills development were all factors perceived to impact the implementation of remote rehabilitation. The online toolbox was well received, and provided clinicians support for enhancing knowledge and confidence, but challenges to remote rehabilitation delivery remain.
The use of two implementation frameworks in this study allowed for detailed exploration of behaviour change factors, within and by organisations and individuals, 30 that could support the implementation of remote PR. That key facilitators of remote PR delivery were common across all healthcare contexts highlights the potential for strategies to support telerehabilitation implementation having application across multiple healthcare environments. To date, evaluation of implementation strategies for remote PR delivery have tended to focus on a single modality or health system model.12,31 The choice of an online toolbox, informed by the findings of study Phase I, as a means of providing implementation support creates an easily accessible resource, irrespective of healthcare jurisdiction, and was considered to act as a ‘one-stop shop’ for remote PR resources. Health professionals have previously described such online resources as being important for making information readily available, and supporting knowledge gain and training across the spectrum of workplace experience but particularly for more junior staff. 32 As well, the concept of an online toolbox can help serve as a catalyst for service change. 33 In a study of health professionals primarily delivering remote neurological rehabilitation, an online toolkit helped participants to demonstrate the utility and importance of remote rehabilitation to organisational management. 33 In this way the toolbox may serve as a means to lobby, in particular, for organisational change by highlighting the resources and program components, with relevant adaptation to local context, identified to support remote PR delivery.
The use of videoconferencing to support remote PR delivery was favoured by participants. The ability to see patients via video was felt to create rapport and encourage clinician confidence by enabling a visual element for monitoring and evaluation. It was, however, acknowledged that videoconferencing was not available to, or preferable for, all patients. There is increasing evidence that patient preference for remote healthcare consultations varies by modality, with people of older age, lower socio-economic status, and female sex along with minority groups and those from non-English speaking backgrounds typically less likely to choose video-based interactions. 34 Perhaps paradoxically, while video for remote rehabilitation was preferable, clinicians lacked confidence with operating and trouble-shooting technology equipment and saw this as a significant barrier to implementation of telerehabilitation. Lack of confidence with technology is a long-standing concern of clinicians for remote service encounters,14,35,36 and affirms that strategies to support remote PR delivery need to not only foster knowledge and skills development but require institutional support for cross-discipline collaboration specifically with ICT providers. While the online toolbox provides theoretical support for the use of videoconferencing to deliver telerehabilitation, its capabilities do not extend to hands-on skills practice. In future, blended learning opportunities, incorporating skills practice, simulation and ‘real-life’ observation, may better support health professionals confidence to integrate telehealth-delivered care into clinical services. 37
The COVID-19 pandemic saw the rapid scale-up of remote healthcare delivery. 38 Despite the pandemic inspired removal of many barriers to remotely delivered healthcare, 39 clinician acceptance of telerehabilitation is key to service implementation,40,41 and highlights the core role of the ‘individual’ in implementation success. Even in the context of increased remote service capabilities in response to COVID-19, 42 clinician reluctance may relate to feelings of limited preparation and training,36,43 or as identified by participants in this study be inherently linked to the training of healthcare professionals in a face-to-face environment with in-person patient interactions. In a survey of telehealth use among healthcare professionals conducted from November 2021–March 2022 of those who had experience using telehealth (n = 491), nearly half had less than 1-year experience. 44 Whether healthcare professional acceptance of remote service delivery models will evolve with increased experience, and/or a future workforce who have received formal training in alternative service delivery, is not clear. The development of core capability frameworks, such as that proposed by Davies et al, to support skills training in the delivery of remote health may encourage greater confidence and acceptability. 43
Key factors to support health professionals to deliver telerehabilitation for people with chronic lung disease were common across different healthcare contexts, suggesting broader telerehabilitation implementation strategies may be applicable across healthcare environments. Health professionals considered an online toolbox a valuable resource that could support individual clinician knowledge and skills and thus confidence and acceptance of remote PR delivery. However, organisational-level issues such as service funding and equipment and technology accessibility still exist. Despite increased remote healthcare service delivery in response to COVID-19, common barriers to the implementation of remote PR remain irrespective of health system or geographical location.
Supplemental Material
Supplemental Material - Supporting delivery of remote pulmonary rehabilitation across different healthcare contexts: A multi-national study
Supplemental Material for Supporting delivery of remote pulmonary rehabilitation across different healthcare contexts: A multi-national study by Narelle S Cox, Sarah Rawlings, Natasha A Lannin, Sarah Candy, Surya P Bhatt, Abraham Samuel Babu and Anne E Holland in Journal of Chronic Respiratory Disease.
Footnotes
Author contributions
Concept and design: NSC, AEH. Procured funding: NSC, SC, ASB, SPB, AEH. Data acquisition: NSC, SR, SC, ASB, SPB. Data analysis and interpretation: NSC, SR, NAL, AEH. Manuscript drafting: NSC, SR. Critical review of manuscript and approval of final version: All.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NSC, SC, SPB, ASB and AEH were all named collaborators on the funding application which underpinned this work. SPB reports grants and fees unrelated to the present work. For all others, nil to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Academy of Science (Regional Collaborations Programme COVID-19 Digital Grants) and the Department of Industry, Science, Energy and Resources [RCP DG Cox]. The following authors receive Research Fellowship support from National Health and Medical Research Council: NSC (GNT2016286), AEH (GNT1197007); and from Heart Foundation Australia: NAL (106762).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.