
Abstract
Introduction
There are early data to suggest that a rehabilitation programme can help with on-going symptoms of COVID-19, including breathlessness, exercise limitation and fatigue. As yet, there are no published data to understand patients’ perceived acceptability of a rehabilitation programme for COVID-19.
Methods
2 focus groups (n = 9) and 4 one to one interviews were conducted with participants who attended a rehabilitation program following COVID-19. Interviews were analysed using reflexive thematic analysis with an inductive approach.
Results
Two overarching themes were generated from the data. The first, The Recovery Journey is sub-divided into five sub-themes of Expectations, Individual and Varied Journeys, Mental and Physical Improvements, Self-values and The Journey Continues. The second overarching theme, The Rehabilitation boat contains five subthemes: Programme Delivery, Safe and Supportive, Validation and Assurance, Shared Reflections and Education.
Conclusion
A rehabilitation programme for post COVID-19 symptoms was considered to be acceptable and viewed positively in terms of improving physical and mental symptoms. The opportunity to share the experience with others in the same boat was highly valued in the context of an unexpected and potentially lonely COVID-19 recovery.
Introduction
COVID-19 can cause on-going symptoms including breathlessness, fatigue, and limited ability for activities of daily living that persist long after the acute event, irrespective of ventilator requirements or length of stay in hospital. 1 Additionally, 70% of patients discharged from hospital following COVID-19 infection did not consider themselves fully recovered at 5 months 2
There is expert consensus that a rehabilitation programme should be offered to support physical and emotional recovery following COVID-19. 3 This is supported by NICE guidelines for long term management of COVID-19 which recommend offering tailored mutli-disciplinary rehabilitation. 4 The commonly reported on-going symptoms such as breathlessness and fatigue overlap with the needs of a pulmonary rehabilitation population. 5 There is a clear rehabilitation need for individuals post-hospitalisation for COVID-19 with 25.1% of all those who had a positive test/clinical diagnosis of COVID-19 as an inpatient identifying rehabilitation needs. 6
Encouraging early data shows that a face to face, supervised, rehabilitation programme can improve symptoms following COVID-19 infection. 7 In a cohort study of 30 participants there were significant improvements in measures of exercise capacity, and symptoms of breathlessness, fatigue and cognition. 8 There are no qualitative data available exploring the experiences of patients taking part in a rehabilitation programme for COVID-19 or how such a programme impacts on recovery. Exploring the lived experience of individuals attending a rehabilitation programme for COVID-19 is important to understand the acceptability of the intervention. In the context of healthcare interventions acceptability can be defined as a ‘multi-faceted construct that reflects the extent to which people receiving a healthcare intervention consider it to be appropriate, based on anticipated or experienced cognitive and emotional responses to the intervention’. 9 Knowledge gained from understanding first-hand experiences of the programme will inform the future development of this and other programmes.
The aims of this research were: 1. To explore lived experience of post COVID-19 symptoms in those who followed a COVID-19 rehabilitation pathway. 2. To understand acceptability of rehabilitation programme for COVID-19.
Methods
A qualitative approach was used to gain an in-depth understanding of individuals’ experience of COVID-19 rehabilitation and its impact on symptoms and activities of daily living. The Consolidated Criteria for Reporting Qualitative Studies (COREQ) have been followed to report this research. 10 Ethical approval was gained from the Leicester South Research Ethics Committee (17/EM/0156).
Interviews
Research team and reflexivity
CG led the interviews, and these were moderated by another researcher (ED, AB or NG). CG was a female, research physiotherapist, undertaking masters-level training in research methods. All other researchers were experienced in conducting qualitative research. The interviewers were not involved in the participant’s direct care, and the first author was not involved in the rehabilitation programme.
Study design
Participants were recruited from the face-to-face COVID-19 rehabilitation programme. The programme offered a symptom titrated exercise programme alongside self-management educational adapted from www.yourcovid.recovery.nhs.uk. The supervised sessions were twice weekly over 6 weeks for 1.5–2 h (aerobic, strength exercises, and education sessions). Details of the programme have been previously reported. 7 The interviews were conducted between February and May 2021. A convenience sampling strategy was used. The first 36 participants who attended the rehabilitation programme were invited to take part in the study and were approached by telephone. 13 people agreed to take part.
An interview guide was developed by all authors, see Online Appendix. All interviews were conducted virtually due to lockdown restrictions, there were no repeat interviews The choices of 1:1 interview or focus group were offered to participants. 1-1 interviews were conducted via telephone, and focus groups via video-call. Both formats were offered to facilitate patient preference and aid recruitment to the study. Field notes were made during the interviews and focus groups by each moderator. Reflexive journals were kept following each interview or focus group. NDespite using a reflexive thematic analysis approach, data saturation was used for pragmatic reasons and was reviewed during the process of data collection. 11 Due to time constraints, transcripts were not returned to participants for comments or correction.
Data analysis
Data were analysed using reflexive thematic analysis, a theoretically flexible approach to interpreting the data by identifying and developing themes across the dataset. 12 An inductive approach was used to generate codes and themes directed by the content of the data. Each transcript was independently coded by two authors. All authors were involved in coding the data. Notes taken during the interviews by a moderator were compared with interview transcripts for accuracy.
Survey
Survey data
Surveys exploring patients’ experience of rehabilitation were completed by patients anonymously at their rehabilitation programme discharge as per normal clinical processes. The survey covered topics including: satisfaction with the program, transport requirements, wait times, comments on what was included in the program. Patients who completed rehabilitation between November 2020 and January 2021 were asked to complete surveys at discharge. The available survey responses from the same cohort of patients approached for interviews were used to triangulate data. Descriptive statistics were used to report the data.
Results
Qualititave interviews
Patient characteristics
36 patients were contacted, of which 13 took part (54% male, 62% white British, 8% white other, 16% Indian, 8% other Asian, 8% black African). One participant was not admitted to hospital. Average mean (SD) length of hospital stay was 15 (18) days, 23% were ventilated. Six participants were healthcare workers and a further five were working. Three participants had a pre-existing respiratory condition, however all subjects were naïve to rehabilitation and no participants had any oxygen requirements during the course.
Themes and subthemes explored
Two over-arching themes were generated from the data: the Recovery Journey and the Rehabilitation Boat. Sub-themes are presented in a metaphorical visual display (Figure 1) to demonstrate the connection to the over-arching themes.
13
A description of each over-arching theme and key illustrative quotes are provided in Table 1. A metaphorical visual display to demonstrate the sub-themes of the two over-arching themes ‘The Rehabilitation boat’ (illustrated as a boat) and ‘The Recovery Journey’ (illustrated as a river). A table to show the over-arching themes, sub-themes and key illustrative quotes.

The Recovery Journey describes the varied journeys through recovery from expectation of rehabilitation through to the on-going journey. This theme is divided into the following five sub-themes:
Expectations
The severity and burden of the acute and longer-term symptoms were unexpected. Many patients had not experienced severe illness before. In addition, it was experienced in the context of significant media attention on the acute COVID-19 crisis. For these patients, at the time of illness there was little focus on the potential long term symptoms burden. “I just couldn’t believe how weak, just my general let alone my breathing. I mean my breathing was appalling. But yeah I just couldn’t believe how poorly I felt really.” (Participant B)
Expectations for the impact of COVID-19 rehabilitation on symptoms were varied and conflicting. Some patients voiced surprise and amazement regarding improvements in their symptoms suggesting the outcome of rehabilitation exceeded their expectation. There was expectation that healthcare services would be too overwhelmed managing the acute pandemic to offer support in the recovery phase. “I just hoped to get stronger and fitter and I got stronger and fitter and I was amazed by how much difference” (Participant D) “So that gave me a bit of hope that I wasn’t just going to be discharged home and just left to get on with it, which is what I was probably expecting just because of how severe the pandemic was.” (Participant B)
Individual and varied journeys
Recovery was considered a long journey with peaks and lows. Journeys were individual with a variety of physical and mental symptoms reported. Participants recognised this variety and the need for a rehabilitation programme to be adaptable. As further described in the ‘Programme Delivery’ sub-theme of the ‘Rehabilitation Boat’, patients perceived the programme to be tailored to their needs and capability. “We were a completely different group with completely different individuals there. So I always felt that the team there was looking at, this is how you arrived and this week see if we, you know, can you do that little bit extra, can you do that little bit extra, and it was very much concentrating of the point where you arrive.” (Participant E) “You’re in a room with six other people that have got different side effects and different experiences.” (Participant A)
Mental and physical improvements
Improvements in physical symptoms included reduced breathlessness, and improved exercise capacity and reduced fatigue. Patients linked the exercise component to improved physical symptoms. Improvements in emotional wellbeing included feeling more confident and less worried. These improvements were mostly attributed to empathy from peers and supportive staff. There was an overall picture of recovery, for some completely. For others there was improvement but a feeling of not being completely back to normal and continuing on the journey of recovery after the programme. “So after the rehabilitation I could go out, I could go out for a walk, for hour’s walk and come back and feel happy without feeling that tired, without feeling exhausted and still carry on doing some things at home.”(Participant F). “The difference is just amazing and able to do what you want to do and feel happy and not worried of what is going to happen. The difference is just mind-blowing” (Participant H).
The journey continues
The journey of recovery continues following rehabilitation. As described in the ‘Expectations’ sub-theme, this was unexpected by many patients where longer term COVID-19 symptoms were surprising. For many, the rehabilitation is the beginning of their recovery journey. Many had maintained the walking exercises and cited using exercise diaries and pacing strategies. There were barriers to maintaining exercise, mostly relating to lockdown restrictions. Overall, it was considered important to maintain exercise behaviours after rehabilitation and this was linked to improvement in symptoms. This links to the following sub-theme in that patients highly valued exercise for its perceived contribution to their improved symptoms. “I believe it’s very important to keep up the exercise and it [rehabilitation] plants it in your mind.” (Participant J) “I have taken it forward, I want to just keep walking, I want to keep getting better, I want to keep doing the exercises.” (Participant G).
Self-values and identity
There was a sense of being a survivor and gratitude for support in recovery. There was a shift in values to prioritising own well-being and leading a healthy lifestyle. For many it was important, after COVID-19, to prioritise health over work. Some patients reported a change in their identity following COVID-19, where there symptoms limited their normal behaviour as explain by Participant C:
“They know I’m one in the world, what I call, I’m a doer. I actually get on and do things and obviously this wasn’t me with what had happened”
These experiences may indicate a change in values around health behaviour and priorities. Exercise was linked to improvement in symptoms and many patients were maintaining exercise after rehabilitation. “You know what, I’m privileged to be a survivor”. (Participant G) “what I’ve taken away from it is really just to encourage others, the importance of the fitness regime today, even if it’s just walking, swimming, whatever it may be, but just to try and get yourself as healthy as possible.” (Participant H)
The Rehabilitation boat refers to the overall feeling of togetherness, support, and safety. This theme is divided into the following five sub-themes:
Programme delivery
The programme was perceived positively. However, there was consensus that a longer programme would be preferable. This may not be surprising given that recovery from COVID-19 was considered a long journey. There was an overall feeling that the programme was tailored to individual needs and abilities and this was important to patients. Patients found that exercises were set to their level and were supported by staff to progress or regress depending on their needs. This suggests the supervised element of the programme was important. “[The] range of exercise, as I say, was exactly the right level and the team were superbly supportive, they really knew what levels to take you to.” (Participant I)
Safe and supportive
Rehabilitation was considered a safe and controlled environment. There was a sense of emotional safety provided by empathetic and motivating staff and peers. Whereas, the physical tests and measurements made patients feel physically safe. It is interesting that patients identified the importance of emotional and physical safety during a rehabilitation programme. At a time of significant media attention on hospitals and acute COVID-19 there was little focus on or understanding of longer term symptoms. In rehabilitation there was a strong sense of sharing, camaraderie and being in the same boat, this phrase was coined by Participant J: “I got to see other people in the same boat as me. I think that made a difference”. “It’s allowed me to push myself more in a controlled way and it’s just been very useful” (Participant K)
Validation and assurance
The emotional support and empathy experienced from staff and peers was valued and provided reassurance. Patients experienced validation of their symptoms from the existence of the service, the staff and their peers. This was important in the context of on-going COVID-19 symptoms being poorly understood or misbelieved by others around them, including family members, friends and healthcare professionals. It is important to remember this cohort of patients experienced the disease early in the pandemic when a lot of focus was around the acute unwell and less was known about longer term COVID-19 symptoms. This compounded a feeling invalidation. “So me coming out there [rehab programme], I felt like somebody who has been released out of the cage and I felt so free.” (Participant G) “They helped us to understand actually it’s OK to feel like this. I had people saying to me, but you had COVID ages ago you must be better now” (Participant L)
Shared reflections
Rehabilitation was a unique opportunity to share true experiences with others in the same boat. Patients endured unpleasant sights and experiences during their hospital stay, as well as significant symptoms even after their discharge home. In some cases, patients did not share these in order to protect family and friends. Opportunity to reflect freely with others who had the same experience was important. Reflecting together during rehabilitation was a unique and valuable opportunity. This experience may explain why there was a strong feeling of emotional support from participants as seen in the previous sub-theme. Patients shared their advice to others with on-going COVID-19 symptoms, in light of the importance identified of sharing experiences with others in the same boat, these are listed in Figure 2. “I didn’t share what I saw in hospital with anyone, or I lie about what I saw in hospital, because you have to protect your family and your people around and there is no point to share what you saw, because you are just going to worry them.” (Participant D) “In the group…we were able to discuss between us other symptoms as well and it was nice to be able to reflect because… sometimes I feel like I’m going mad and it’s just nice to know that other people are actually experiencing similar things to you.” (Participant B) Quotes to illustrate participant’s advice to other patients with on-going COVID-19 symptoms.
Education
Session content was valued by all even when not relevant to the individual. There was an understanding that the rehabilitation programme needed to suit individual patient needs. Education sessions were viewed as an open forum and valued for facilitating discussion. Discussion was considered to facilitate reflections discussed in the previous sub-theme which were important in the context of misbelieved or misunderstood symptoms. “Everything they said I already knew… and it was very much the rest of the group found that very useful and it prompted a lot of discussions within the group.” (Participant F) “There’d been an open forum… it was to get you thinking as to what you’d been through and what you could do to really help yourself.”(Participant J)
Survey triangulation of data with survey responses
Completed satisfaction surveys were available for 38 individuals (Figure 2). 92% of individuals found rehabilitation satisfactory. 87% could do more activities of daily living since completing the programme. 86% agreed their fitness levels had improved since beginning the rehab programme. This supports the sub-theme ‘Mental and Physical Improvements in which patients reported overall improvements in wellbeing and symptoms. 97% found that the rehabilitation programme was worthwhile. 97% found the information in the education talks useful, this supports the sub-theme of ‘Education’ in which the education sessions were highly valued, mostly for the facilitation of shared reflection. 89% found that the programme helped with their recovery. 99% would recommend the program to other with the same condition. (Figure 3) Contingency graph to show rehabilitation satisfaction survey responses.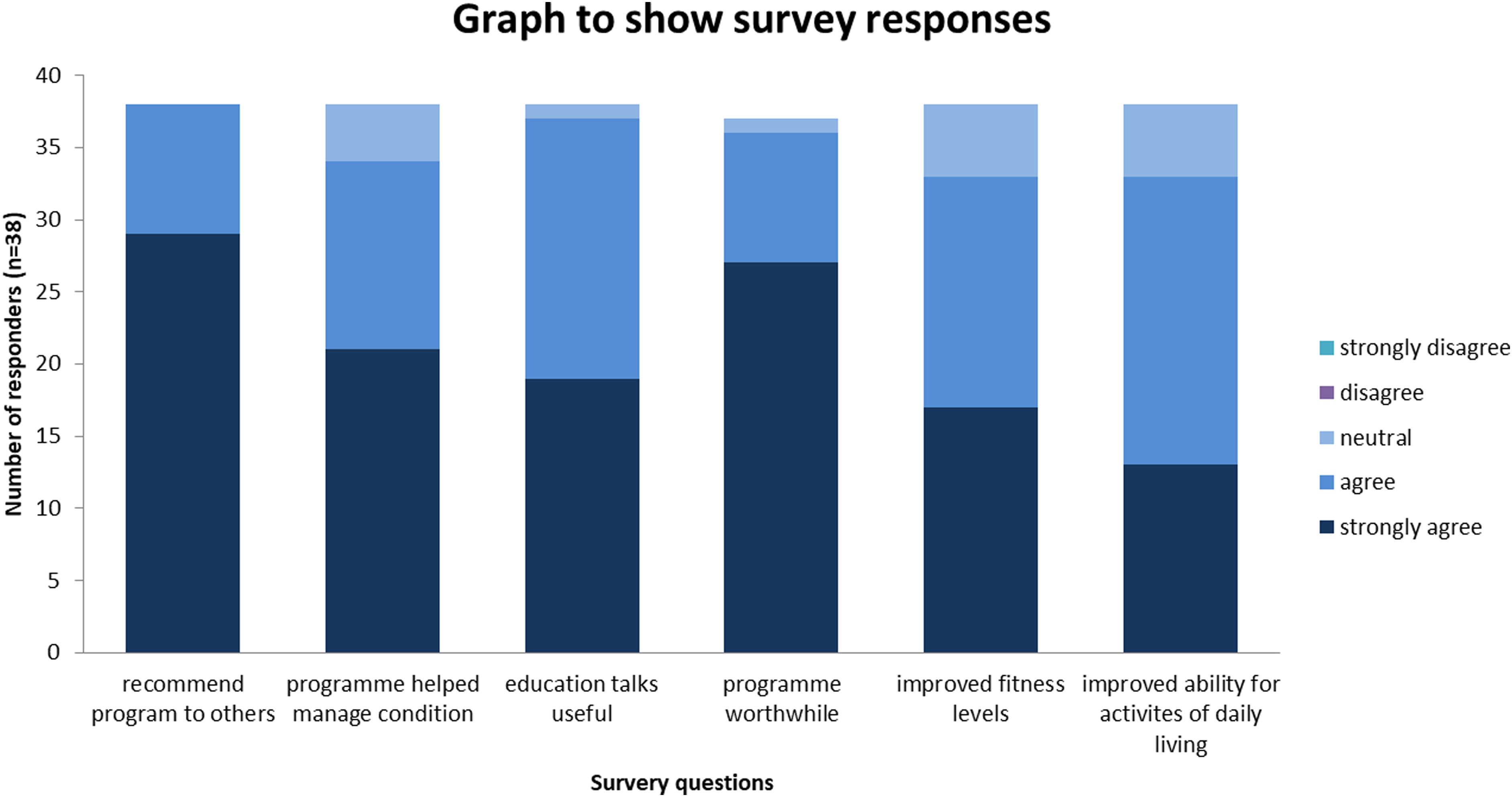
Discussion
Overall, rehabilitation was considered important and worthwhile. This is reassuring for the service providers, considering that the ‘Rehabilitation Boat’ was constructed with little information for its context. The rehabilitation programme was viewed positively and considered to improve symptoms and aid recovery, this is corroborated by the survey results. These findings mirror improvements seen in exercise capacity, fatigue, breathlessness, and cognition in a cohort of patients attending a rehabilitation programme. 7
Specific aspects of the face-to-face programme were highlighted as important. Patients recognised individual journeys through recovery, and this may explain why the tailored nature of the programme was highly valued. This suggests the supervised element of this rehabilitation programme was important. The ‘Validation and Assurance’ and ‘Shared reflection’ sub-themes bring together patients experiences of isolation in recovery. It seems recovery from COVID-19 can be a lonely experience and this may explain why the opportunity to share experiences with people in the same boat was so highly valued.
Clearly, the supportive staff and peer sharing elements of the face-to-face programme are important. Halding and colleagues 14 explored social relationships in pulmonary rehabilitation (PR) for people with chronic obstructive pulmonary disease (COPD) and identified that shared experiences facilitated mutual trust and a sense of belonging through shared understanding. Similarly, these participants identified the program, in particular the education sessions, as a unique opportunity to share and reflect on experiences. If offering virtual rehabilitation options for people with COVID-19, it will be important to consider how the impact of not having the opportunity to share experiences with others may affect outcomes.
Participants described a shift in their values to prioritising their own health and to leading a healthier lifestyle going forwards. There was a strong preference for the program to be longer which may reflect the reported on-going journey through recovery following the program. There is evidence that some interventions designed to maintain the benefits of pulmonary rehabilitation for people with COPD may improve health-related quality of life and exercise capacity at six to 12 months 15 It will be important to consider how patients recovering from COVID-19 can be best supported following rehabilitation and whether there is a need for maintenance support.
Strengths and limitations
There are several strengths to this study. In this reflexive approach, all researchers reflected on their bias prior to the interviews. The interviews and focus groups were moderated for data collection and for generation of codes. Data triangulation was provided in the form of survey responses from the same cohort of patients approached to take part in this research.
There were limitations to this study. Patients involved were mostly those hospitalised for COVID-19, in addition this group were mostly unwell at the beginning of the pandemic when less was known about the disease and stricter lockdown measures were in place. As with all qualitative research, these findings are not generalizable but should help inform future or develop current programmes. Patients are more likely to take up an interview if they have a good or bad experience to share. Measures were taken to mitigate sample bias by inviting all patients and using flexible interview methods. Survey responses were used to provide data triangulation to mitigate this.
Conclusion
Attending rehabilitation following COVID-19 was considered to be a positive experience and an important part of recovery by these participants. Recovery was considered an unexpected, long, and variable journey and the tailored nature of the program was valued. There was a strong preference for the program to be longer, it will be important to consider the need for maintenance options post-rehabilitation. We may see a variety of COVID-19 rehabilitation delivery options to meet expected demand and it will be important to consider that the supervised and peer group elements of the rehabilitation program were highly valued.
Supplemental Material
Supplemental Material - The Recovery Journey and the Rehabilitation Boat - A qualitative study to explore experiences of COVID-19 rehabilitation
Supplemental Material for The Recovery Journey and the Rehabilitation Boat - A qualitative study to explore experiences of COVID-19 rehabilitation by Charlotte Gerlis, Amy Barradell, Nikki Y Gardiner, Emma Chaplin, Amye Goddard, Sally J Singh and Enya Daynes in Chronic Respiratory Disease
Footnotes
Author contributions
The protocol was developed by CG, ED and SS. CG conducted all interviews, NG, AB and ED moderated the interviews. CG, AB, NG, EC, AW and ED contributed to data coding. CG developed the manuscript and this was approved by all authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was funded through the Health Education England/NIHR, East Midlands Integrated Clinical Academic Internship Award (University of Lincoln). This study is supported by the National Institute for Health Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.