
Abstract
Despite overwhelming evidence of its benefits, a widespread implementation of pulmonary rehabilitation (PR) is lacking and the landscape of multidisciplinary programs remains very scattered. The objective of this study is to assess how PR is organized in specialized care centres in Belgium and to identify which barriers may exist according to respiratory physicians. A telephone and online survey was developed by a Belgian expert panel and distributed among all active Belgian chest physicians (n = 492). Data were obtained from 200 respondents (40%). Seventy-five percentage of the chest physicians had direct access to an ambulatory rehabilitation program in their hospital. Most of these programs are organized bi or triweekly for an average period of 3–6 months. Programs focus strongly on chronic obstructive pulmonary disease patients from secondary care, have a multidisciplinary approach and provide exercise capacity and quality of life measures as main outcomes. Yet large differences were observed in process and outcome indicators between the programs of centres with standard funding and those of specialized centres with a larger allocated budget. We conclude that multidisciplinary PR programs are available in the majority of Belgian hospitals. Differences in funding determine the quality of the team, the diversity of the interventions and the monitoring of outcomes. More resources for rehabilitation will directly improve the utilization and quality of this essential treatment option in respiratory diseases.
Introduction
According to the American Thoracic Society (ATS) and the European Respiratory Society (ERS), pulmonary rehabilitation (PR) is a comprehensive intervention based on a thorough patient assessment, followed by patient-tailored therapies that include, but are not limited to, exercise training, education and behaviour change, designed to improve the physical and psychological condition of people with chronic respiratory disease and to promote the long-term adherence to health-enhancing behaviours. 1
PR plays an essential role in the management of symptomatic patients with chronic obstructive pulmonary disease (COPD). The main benefits of comprehensive PR programs for patients with COPD include a decrease in symptoms (dyspnoea and fatigue), improvements in exercise tolerance and health-related quality of life, 2 –4 a reduction in health-care utilization and potentially an effect on exacerbation rate and survival. 5 –7 Over the last decade, compelling evidence is also rising on the indication of PR for other respiratory domains, including cystic fibrosis, interstitial lung diseases, pulmonary hypertension, lung cancer and lung transplantation. 8 –12 Furthermore, several authors have demonstrated a favourable cost-benefit ratio for PR in different health-care systems. 13,14
Despite the huge amount of scientific evidence in favour of PR in different respiratory diseases, the number of patients referred to existing programs is low. Major barriers that have been identified include a lack of awareness and knowledge of patients and health-care practitioners, a limited accessibility to established programs for a disabled population and the insufficient funding and quality control of the existing programs. 15,16 In a large survey completed by representatives of 430 centres from 40 countries, not only key similarities but also large differences among PR programs across continents and within countries have been highlighted, which concerned the setting, the case mix of individuals with a chronic respiratory disease, the composition of the PR team, the completions rates, the methods of referral and the types of reimbursement. 17 The authors stressed the importance of process and performance indicators as benchmarks to ensure quality and multidisciplinarity, in accordance with international standards.
The health-care system in Belgium is public, funded by the federal government with a fee-for-service–based reimbursement system. In general, respiratory rehabilitation in Belgium is organized at different levels. Patients in primary care are most often referred to private physiotherapists for an individualized exercise training program of 18 sessions (which amounts the maximum number of physiotherapy sessions reimbursed), eventually extended to longer interventions when specific lung function criteria (forced expiratory volume in one second [FEV1] < 60% of predicted value) are met for additional reimbursement. In secondary care, most multidisciplinary PR programs are developed under the supervision of physical medicine specialists. Federal funding for these PR programs is obtained from the number of individual training sessions in patients who met the specific criteria of FEV1 (FEV1 < 60% of predicted value), with a maximum of 60 sessions. In general, these allocated resources are insufficient to cover the expanding multidisciplinary needs of respiratory disease-specific programs. Therefore, PR programs are often incorporated in the larger structural programs of cardiac, orthopaedic and neurological disorders. Finally, maximized PR for more severe respiratory patients is available in four expert centres geographically spread over the country. These centres have obtained a larger budget to execute 60 multidisciplinary sessions in symptomatic patients with severe respiratory disease (diffusing capacity [DLCO] or FEV1 < 50% of predicted value) and at least two of the following markers of functional impairment: quadriceps force < 70% predicted, respiratory muscle force < 70% predicted, 6-minute walk distance (6MWD) < 70% predicted, maximal load on incremental exercise < 90 W and Chronic Respiratory Disease Questionnaire symptoms score < 20 points or total score < 100. Only pulmonologists with an additional 2 years of certified training in PR are allowed to oversee these programs. Every year, these centres have to report inclusion, process and outcome indicators to the federal health-care agency.
Although the organization of rehabilitation at increasing levels of intensity may theoretically cover the heterogeneous needs of respiratory patients, the actual landscape is very scattered. PR programs are developed rather by local needs or network initiatives than by a centralized structural plan to cover the needs of the Belgian population. At this stage, little data are available on the number of the programs in Belgium, or on process and outcome indicators that are used. The objective of our group is to register how PR in secondary care centres is structured, how programs are organized with regard to the allocated resources, and which barriers still exist according to the respiratory physicians. Based on an extensive telephone and online survey, we report here on the main outcomes.
Material and methods
Medistrat (Lasne, Belgium) received support from the Belgian Society for Pneumology (BVP-SBP) and from the Chiesi Foundation (http://www.chiesifoundation.org/) to undertake a large survey with all active chest physicians (492) in Belgium. Between May 2015 and August 2015, all physicians were first contacted by email for their willingness to participate and if no answer was obtained after one reminder, contacted by Medistrat by phone for potential interest. They were asked to fill out an online questionnaire or take a telephone interview lasting 15 minutes on average. To augment participation, no preparatory work was demanded before completing the survey. Chest physicians agreeing to participate provided first their domain of interest, the address and type of their practice (hospital, private or combination) and whether or not they had access to a rehabilitation program in the hospital. The questionnaire was designed by Medistrat based on the input of an experienced team of physicians and physiotherapists involved in PR. The questions covered the structural organization, patients and program characteristics and program evaluation (Table 1). The complete questionnaires provided to the physicians are available in Table S1 of the Online Supplementary material. The recorded information was treated anonymously to respect data privacy, and the results were analysed using descriptive statistics (numbers and percentages) and χ 2 tests for significance.
English short version of the survey questions that were asked to the Belgian chest physicians.

PR: pulmonary rehabilitation
Results
Physicians
Of the 492 physicians contacted, 221 directly refused by email or telephone, 271 were interested for participation, of which 71 refused or cancelled at the second stage. Completed questionnaires were obtained from 200 chest physicians (24% via Internet and 76% via the phone), which were all used for the analysis. Sixty percentage of the answers were collected from physicians practicing in Brussels or Wallonia and 40% from physicians in Flanders. Sixty-six percentage of respondents were only practicing in the hospital, 1% had a private practice and 33% combined hospital and out of hospital private practices. Overall, respondents were representative of the broad respiratory specialist workforce in Belgium, with a general profile and a broad interest in respiratory diseases.
A total of 25 chest physicians (12%) were affiliated to a hospital with an expert PR program supported by the federal convention (convention hospitals (CHs)). Nearly two-third of the physicians (N = 124; 62%) had access to a PR but non-expert program in their hospital (PRH), while one quarter (N = 51; 26%) had no PR program in their hospital (non-PRH). A map of the different hospitals, with PR program and at least one participating physician, is provided in Figure S1 of the Online Supplementary material. In the CHs, 96% declared that a chest physician was in charge of the program, which is obligatory by the convention agreement. In hospitals with no convention (PRH), the persons in charge of PR were either specialists in physical medicine (41%) or chest physicians (53%). Interestingly, 80 physicians of 149 with a PR program (CH + PRH; 54%) declared to have a chest physician with a certification in PR (recognized subspecialty for respiratory physicians in Belgium) in their team. These skilled physicians were often in charge of the program (data not shown).
Patients
Patients in the PR program were referred by chest physicians of that same hospital (97%). Seventy-eight percentage of the respiratory physicians who participated in the survey referred patients themselves. Forty-six percentage reported to have referrals from chest physicians outside the hospital (67% for CH and 42% for PRH). Surprisingly, the number of patients referred by the general practitioners was only 22% on average (with no statistical difference between CH and PRH) and almost no referrals by other disciplines were deemed to be present (4%).
The different respiratory diseases of patients included in PR programs are depicted in Figure 1. Most physicians (86%) reported to have stable COPD patients in their program, 75% also reported to include unstable COPD patients. Other respiratory diseases were less frequently reported as being part of the local training program (50% for restrictive disorders to 18% for cystic fibrosis). Overall, physicians estimated the number of patients entering a local PR program at 57 per year on average (n = 119 per year in CH; n = 45 per year in PRH; data not shown). Forty-three physicians (21.5%) declared no patient refusals to participate in a PR program; 157 physicians (78.5%) declared to encounter refusals for a variety of reasons (Figure 2). According to the physicians, main reasons invoked by patients for declining a proposed PR program were the following: (a) the distance from home and the absence of transport, (b) too time-consuming and (c) lack of interest. For centres with no PR program in the hospital, the relative weight of all the reasons for not participating tended to be higher. Once refused to enter a hospital-based PR program for whatever reason, the alternative options for rehabilitation proposed by the chest physician (three of a list of nine) varied between the groups (Online supplementary Table S2). In general, for CHs, the preferred alternative was a specified prescription to an experienced physiotherapist (73%) over a general prescription (41%). By contrast, physicians working in PRH or centres without PR program (non-PRH) preferred the general prescription for physiotherapy (64%; p = 0.05 for comparison with CHs) over a prescription to an experienced physiotherapist (41%; p < 0.005 for comparison with CHs). Independent of the group or hospital setting, the referral to primary care, patient empowerment and standard medication were plausible options for 30–40% of the physicians.
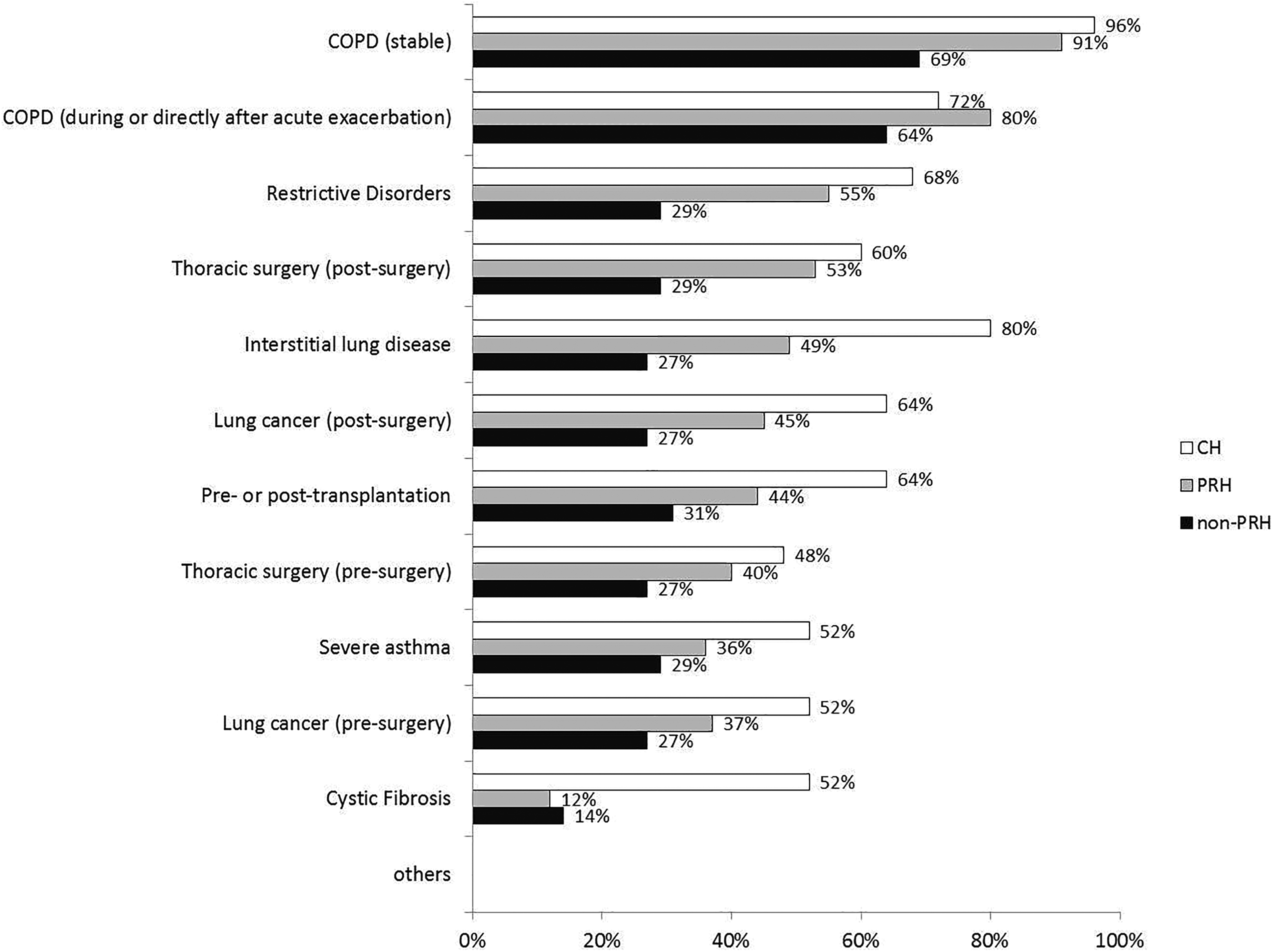
Types of patients included in PR programs expressed as percentages of chest physicians in centres having no convention but a PR program (N = 124; white), in centres having a convention (N = 24; grey) and in centres without a convention and a PR program (N = 52; black). PR: pulmonary rehabilitation.

Reasons invoked by the patients for not entering the proposed PR program (N = 157; 10 point-scale: 1 = never for this reason and 10 = very often for this reason). The full line corresponds to centres with a PR program and the dotted line to centres without PR program. PR: pulmonary rehabilitation.
Programs
In the CHs, the professionals involved in the PR teams were physiotherapists (96%), chest physicians (92%), dieticians (84%), social workers (76%), psychologists (76%) and occupational therapists (72%). Although these disciplines should theoretically be part of the multidisciplinary team according to the convention, some of the survey respondents were not aware of their role. In the absence of a convention, these numbers were, respectively, 94, 77, 52, 52, 51 and 48%, indicating a reduced multidisciplinarity with regard to the presence of a dietician, psychologist and occupational therapist (Figure 3(a); Online supplementary Table S3).

(a) Disciplines included in the rehabilitation team according to the percentage of physicians (Occupational…: occupational therapist; Exercise…: exercise physiologist). (b) Interventions included in the PR programs according to the percentage of physicians. (Resistance…: resistance training using apparatus, Pursed…: pursed lips breathing, Resistance training using…: resistance training using handheld weights/elastic bands, Energy conservation…: energy conservation technique/activities of daily living (ADL) training and Neuromuscular electrical…: neuromuscular electrical stimulation). CH: convention hospital; PRH: non-expert hospital with PR program; PR: pulmonary rehabilitation.
According to all chest physicians, the most prevalent exercise training interventions in the PR program were stationary cycling, treadmill walking and resistance training using a training apparatus. The other interventions clearly depended on the presence of a convention. Compared to the CHs, programs of PRH contained less education sessions (84% vs. 66%; p = 0.02), less smoking cessation (84% vs. 62%; p < 0.01), less nutritional (76% vs. 53%; p = 0.02) interventions and psychosocial support (72% vs. 45%; p < 0.005; Figure 3(b); Online supplementary Table S4).
As expected, most training programs had individual sessions that lasted for 30 minutes to 2 hours, at a frequency of two to three sessions a week, for a period ranging between 12 weeks and 6 months. As stipulated in the contract between federal healthcare and the CH, the programs in CH had longer and more frequent sessions for a longer period of time (6 months; data not shown).
In the CHs, the main outcomes, which were provided to the referring physician after finishing the program, were lung function (96%), 6MWD (92%), dyspnoea (84%), quality of life (80%), maximum cardiopulmonary exercise testing (80%) and lower limb muscle strength tests (80%). For programs of the PRH, 6MWD (74%) and lung function (65%) were also the most frequently reported outcomes, whereas quality of life (54%), dyspnoea (53%), maximal exercise testing (50%) and lower limb muscle strength (43%) were significantly under-reported (Figure 4(a); Online supplementary Table S5). All outcomes were significantly and more frequently provided in CH than PRH hospitals (p < 0.02).

(a) Outcomes reported by the PR program according to the percentage of physicians. (Inspiratory muscle…: inspiratory muscle strength, Lower limb muscle…: lower limb muscle strength and Physical activity…: physical activity monitoring). (b) Follow-up organized by the rehabilitation program according to the percentage of physicians. CH: convention hospital; PRH: non-expert hospital with PR program; PR: pulmonary rehabilitation.
Once a PR program was terminated, follow-up with the referring chest physician (88%) was the option of choice. Compared to the PR programs in PRH, the reassessment of rehabilitation outcomes after 6 months to 1 year (76% vs. 37%; p < 0.001), the recommendation for physical activity (64% vs. 45%; p > 0.05) or the referral to a local physiotherapist (56% vs. 39%; p<0.05) or fitness centre (48% vs. 19%; p < 0.001) was more often applied as follow-up of CH PR programs (Figure 4(b);Online supplementary Table S6).
Satisfaction
The level of satisfaction reported by all respondents towards the existing PR programs ranged from absolutely (36%), over yes (34%), it depends (21%), or no (7%), to absolutely not (2%). The absolute satisfaction of chest physicians operating in CH increased to 64% while it dropped to 39% for the chest physicians in PRH centres and 15% for chest physicians with no direct access to PR (p = 0.001; Figure 5). The main reasons for non-satisfaction (n = 17) were weak structure (24%), weak on multidisciplinarity (18%), no feedback/report (18%), limited reimbursement (18%) or lack of physician’s involvement (12%; data not shown). Overall, the main targets for future improvements were considered to be better reimbursement (73%), a broader access (66%), a broader multidisciplinary approach (53%) and/or a larger referral (51%;Online supplementary Table S7).

Levels of satisfaction towards the rehabilitation program according to the percentage of physicians. CH: convention hospital; PRH: non-expert hospital with PR program; non-PRH: no PR program in hospital; PR: pulmonary rehabilitation.
Discussion
The current survey explores how multidisciplinary ambulatory PR programs are organized in secondary and third line care hospitals in Belgium. Based on a questionnaire completed by a representative sample of Belgian respiratory physicians (40%), detailed descriptions were obtained on the organizational aspects, process and outcome indicators of one of the major therapies in respiratory diseases. We found that 75% of the responding chest physicians had direct access to an ambulatory rehabilitation program in their hospital. Most of these programs are organized bi or triweekly for an average period of 3–6 months. The programs are multidisciplinary by nature, focus strongly on COPD patients of secondary care and report 6MWD and lung function data as main outcomes. However, there are major differences between the few programs that have secured larger budgets (CHs) and the majority of programs that have developed under classical means of funding through reimbursement (non-CHs – PRH). Programs that are financially supported by a convention with the Belgian National Institute for Health and Disability Insurance are, by definition, supervised by a respiratory physician with 2 years of training in rehabilitation sciences. The true multidisciplinarity of the team, which consists of a physiotherapist, social worker, dietician, nurse psychologist and occupational therapist, is stipulated in the convention agreement and translates in a larger range of interventions, a better monitoring of outcomes and a more individualized follow-up. The comparison on efficacy between the full-option programs (CH) and standard training interventions (PRH) was not an objective of the current survey. Nevertheless, one can hardly question the added value of smoking cessation, education, nutritional and psychosocial interventions which were often lacking in PRH standard programs. 18,19 Future studies need to include process and outcome parameters, including quality of life measures and symptom scores, to allow a more robust comparison of these performance indicators and their respective heath-economic impact. 16 Furthermore, a revision of Belgian reimbursement criteria that are largely based on pulmonary function tests, to more comprehensive functional and patient-reported criteria, is mandatory for the inclusion of subjects with the largest needs.
Twenty-five percentage of chest physicians did not have direct access to a PR program in their centre. Most of these physicians refer patients to other centres or private physiotherapists upon clinical indication. Our survey indicates that patient barriers for entering a PR program are more pronounced with chest physicians who do not have direct access to PR. Furthermore, the efforts for an appropriate referral, with specified prescription to primary care physiotherapists as alternative, seem also larger in a referring CH. Programs in CH are also superior in the organization of post-rehabilitation care, maintenance training and follow-up. Together, our survey shows that better reimbursement and funding does not only improve the quality of the PR program itself but also extends to the care for eligible patients, who cannot participate or have finished the program in the past. As advocated by the expert panels of the ERS/ATS, a major challenge in the further implementation of rehabilitation are awareness, accessibility and funding. 16,20 Our survey describes the same barriers from the physicians’ perspective and clearly appoints to a central role of appropriate resources.
A major strength of our study is the large sample of participating chest physicians covering the different PR settings of specialized care in Belgium. With a clear distinction between the financing of CH and PRH, our survey demonstrates how improved funding directly impacts on the quality of PR programs and the satisfaction of its providers. These observations may not only apply to the Belgian situation but are also likely relevant to any other health-care system. Vice versa, limited reimbursement for secondary prevention may also reduce the quality below the level of international standards and recommendations. It has to be stressed that most PR programs in PRH provide excellent work for the limited budget. However, if we want to upscale the quality of the average program, a more fair financial compensation for the investments in team and structure will be required. 16
Several methodological limitations of this survey should be underlined, the most important ones being inherent to the survey method itself. Although the questions were aligned with a recent international survey, 17 composed by a professional office and carefully reviewed by a Belgian expert panel, some questions and answers may have been misleading. One difficulty intrinsic to the Belgian situation was the need to translate all questions in French and Dutch, with potentially different connotations. In addition, the survey is providing ‘the physician’s estimation’ but did not search for the patients’ perspective. It is likely that recall bias has affected some of the individual answers, but there is no reason to believe why this would be more in certain hospital settings. In other words, the observed group differences between CHs and non-CHs are consistent and valid findings, although we did not check the correctness of the answers by site visiting. Finally, we deliberately interrogated chest physicians. COPD patients are often followed up by general practitioners or general specialists in internal medicine. It is likely that patients treated in this context may have even lower access to PR programs.
In conclusion, our study demonstrates that multidisciplinary PR programs are available in the majority of Belgian hospitals. Differences in resources determine the quality of the team, the diversity of the interventions and the monitoring of outcomes. An objective evaluation on how appropriate financing results in major quality differences will break the barriers of limited awareness of health-care payers and boost the field forward.
Supplementary material
Supplementary_Material - How resources determine pulmonary rehabilitation programs: A survey among Belgian chest physicians
Supplementary_Material for How resources determine pulmonary rehabilitation programs: A survey among Belgian chest physicians by Wim Janssens, Jean-Louis Corhay, Peter Bogaerts, Eric Derom, Nicolas Frusch, Delphine Nguyen Dang, Jesabelle Kibanda, David Ruttens, Lisa Thyrion, Thierry Troosters, Eric Marchand in Chronic Respiratory Disease
Footnotes
Acknowledgements
The authors would specially thank Chiesi Belgium and the Belgian Thoracic Society for the logistic support and the organization of expert meetings. They would also thank Medistrat and all participating physicians in Belgium.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Janssens reports grants from Boerhinger Ingelheim, Chiesi, GSK, Novartis, Astra Zeneca, outside the submitted work. Dr Bogaerts reports personal fees from GSK, Astra Zeneca, Boerhinger Ingelheim, Chiesi, Novartis, and Bristol-Meyers Squibb, outside the submitted work. Mrs Thyrion and Mrs Kibanda are the employees of Chiesi SA/NV Belgium. The other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Chiesi Foundation.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.