
Abstract
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogenous lung disease characterised by persistent respiratory symptoms. 1 Besides the respiratory symptoms, a decreased exercise capacity is often seen in this population.2,3 Pulmonary rehabilitation (PR) is an essential part in the comprehensive management of patients with COPD. 3 Individually tailored exercise training is widely recognised as the core component of PR since it improves exercise capacity, reduces dyspnea and fatigue symptoms and enhances quality of life. 3 An accurate assessment of exercise capacity is crucial to implement a tailored exercise program and to assess the effectiveness of an intervention.3–5 Additionally, the exercise capacity of patients with COPD provides an estimation of disease severity and progression. 6
The cardiopulmonary exercise test (CPET) is widely acknowledged as the golden standard for evaluating exercise capacity. 7 However, this test has limitations as it demands expertise and expensive equipment to administer. This hampers its implementation into clinical practice. The 6-minute walk test (6MWT) is a well-established field test to assess functional exercise capacity of patients with COPD that overcomes the complexities associated with CPET. 8 It also shows reasonable relations with the patients physical activity (PA). 4 However, due to constraints in time and space, this test is not frequently conducted outside the hospital set-up. 9 Variants using a shorter track or conducted outside are reported,10–12 but widespread adoption remains limited. 13
Therefore, there is a need for a quick and feasible assessment tool that can be used by clinicians across diverse settings. The one-minute sit-to-stand test (1′STST) has emerged as a promising test as it can be conducted across a wide range of healthcare settings. 14 The test has garnered increasing attention in research involving patients with COPD. 14 Recent studies verified its test-retest reliability,14–17 validity,14–16,18–21 and responsiveness.14,22,23 Yet, these investigations were predominantly carried out in well-controlled research environments, so these results require confirmation in clinical practice. Further, there is limited knowledge regarding the physiological response to the 1′STST in terms of the cardiorespiratory stress, and the association of the test results with objectively assessed PA is only investigated in one study. 24
The primary objectives of this retrospective study were to assess (1) the test-retest reliability, (2) the construct validity and (3) the responsiveness of the 1′STST when implemented in clinical practice. The secondary objectives were (1) to compare the cardiorespiratory responses (i.e. heart rate, oxygen saturation, and symptom scores) between the 1′STST, CPET, and 6MWT and (2) to confirm the previously established minimal important difference (MID) of three repetitions. The relationship between the 1′STST and PA was investigated as exploratory outcome.
Methods
Participants
Participants were included in this retrospective study when they fulfilled the following inclusion criteria: (1) a clinical diagnosis of COPD confirmed by spirometry (post-bronchodilator forced expiratory volume in the first second (FEV1) to forced vital capacity (FVC) ratio <0.70); (2) enrolled in the three-month PR program at University Hospital Leuven between 16/06/2022 and 17/03/2023; and (3) performed at least one set of two 1′STSTs prior to the start of PR. Patients with a primary respiratory disease other than COPD were excluded. Data was extracted from the electronic clinical records of the hospital. This study was approved by the Ethics Committee Research UZ/KU Leuven (S-68172). Patients were informed that their data were used for the current analysis; prospective informed consent was not obtained.
Pulmonary rehabilitation
The outpatient PR was conducted in accordance with the European Respiratory Society and American Thoracic Society (ERS/ATS) guidelines. 25 Patients attended the hospital three times a week for three months. The program included whole-body exercises and strength training. Each two-hour session included the following exercises: stationary bike, treadmill, sit-to-stand exercises, stair climbing, leg press, vertical traction, arm ergometry and chest press. Progression was guided by BORG scores, aiming for a dyspnea and fatigue rating of 4-6/10.
Assessments
All assessments took place one week prior to the start of PR and after three months of PR. Patients visited the hospital on two separate testing days, usually with a one-week interval.
One-minute sit-to-stand test
Two 1′ STSTs were taken with one-week time interval. A standard operating procedure was established and training of the assessors (i.e. the pulmonary physiotherapists) was organised. The test was performed on a standard height chair (46 cm) without arm rests. Participants were instructed to stand up and sit down as many times as possible within one minute while crossing their arms over their shoulders. 20 Standardised instructions were given before the test. No encouragement was given during the test itself. The number of repetitions was noted and expressed in absolute values and as percentage of the predicted value. 26 The nadir oxygen saturation (SpO2) and highest heart rate (HR) during the test were recorded. Modified BORG scores (ranging from zero to ten) for dyspnea and leg fatigue were recorded before and at the end of the exercise.
Other physical measurements
Two
Statistical analysis
To investigate test-retest reliability, both 1′STSTs were included; for other analyses the best of both 1′STSTs (i.e. highest repetitions) was used. First, to evaluate test-retest reliability, a paired t test was used to compare the two baseline 1′STSTs. An intraclass correlation coefficient (ICC) was applied to assess their agreement. Second, to evaluate the construct validity, the relation between the 1′STST and other physical measurements (i.e. 6MWT (m), VO2max (mlO2/min/kg), Wmax (watt), and QF (Nm/kg)) at baseline was assessed using Pearson correlation analysis. A very strong correlation was defined as r ≥ 0.80; a strong correlation as r = 0.60-0.79; a moderate correlation as r = 0.40-0.59; a weak correlation as r = 0.20-0.39; a very weak correlation as r < 0.20). 37 We also explored the correlations between the 1′STST and 6MWT with PA parameters (i.e. step count, WT and MI). Third, to test the responsiveness of the 1′STST, a paired t test was conducted to examine the change in the 1′STST following PR, as well as in the other physical measurements and in PA parameters. To investigate the size of the intervention effect, standardised mean difference (SMD) was calculated for all physical measurements. SMD cut-off points of 0.20, 0.50, and 0.80 were considered as a small, medium, and large effects, respectively. 38 Spearman Correlation was employed to assess the relationship between the change in the 1′STST and changes in the other physical measurements. As exploratory outcome, the relation between change in the 1′STST and changes in PA parameters was assessed. For comparison, the correlations between the change in the 6MWT and PA parameters were examined. Fourth, a comparison was made between the cardiorespiratory responses at peak exercise among the 1′STST, 6MWT, and CPET, using a paired t test. Based on the MID of 30 meter in the 6MWT, 39 sensitivity and specificity were calculated for different cut-off points in the 1′STST and a Receiver Operating Characteristic (ROC) curve analysis was performed. Finally, to explore the rationale to perform a second 1′STST in the same assessment time, the analyses for validity and responsiveness were repeated using only the first test. All statistical analyses were conducted using SAS 9.2, with a predetermined level of significance set at 0.05 for all tests.
Results
Baseline characteristics (n = 45).

Data are presented as mean ± SD or n (%). FEV1: forced expiratory volume in one second; DLCO: diffusing capacity of the lungs for carbon monoxide; GOLD: Global Initiative for Chronic Obstructive Lung Disease; mMRC: modified Medical Research Council; BMI: body mass index; 1′STST: one-minute sit-to-stand test; 6MWT; 6-minute walk test; QF: quadriceps force; VO2max: maximal oxygen consumption; Wmax: maximal work rate; WT: walking time; MI: movement intensity.

Flow of patients with COPD following three months of pulmonary rehabilitation. PR: pulmonary rehabilitation; 1′STST: one-minute sit-to-stand test.
Test-retest reliability
There was no significant difference between the initial (20.2 ± 6.4 repetitions) and the second 1′STST (21.0 ± 6.5 repetitions) at baseline (mean difference of 0.9 ± 4.0, p = .13), nor following PR (mean difference of 0.3 ± 3.8, p = .64). The ICC indicated good test-retest reliability at baseline (ICC = 0.79) and at follow-up (ICC = 0.89).
Construct validity
Figure 2 shows weak to moderate positive correlations between the 1′STST and the 6MWT (r = 0.57, p < .0001), QF (r = 0.33; p = .01), VO2max (r = 0.50, p = .0006) and Wmax (r = 0.52, p = .0003) at baseline. A sensitivity analysis using only the first 1′STST yielded similar results (see Figure S1). Correlation between 1′STST repetitions and other physical measurements at baseline. A: 6-minute walk test; B: quadriceps force; C: maximal oxygen consumption during the CPET; D: peak work rate during the CPET; E: step count; F: walking time. 1′STST: one-minute sit-to-stand test.
Responsiveness
Thirty-eight patients (84%) attended the follow-up visit after the three-month PR. The best 1′STST improved significantly (∆ = 3.6 ± 6.4 repetitions, p = .0013) following rehabilitation. The effect size was medium (SMD = 0.56). There was an increase in the 6MWT (∆ = 45 ± 59m, p < .0001; SMD = 0.76), QF (∆ = 12 ± 27Nm, p = .0093; SMD = 0.44), VO2max (∆ = 0.7±2mlO2/min/kg, p = .037; SMD = 0.35) and Wmax (∆ = 7 ± 14 watt, p = .0043; SMD = 0.5) following PR. The change in the best 1′STST was positively associated with ∆6MWT (r = 0.57, p = .002) (see Figure 3), ∆QF (r = 0.48, p = .003) and ∆VO2max (r = 0.41, p = .014), but not with ∆Wmax (r = 0.27, p = .11). When considering only the first 1′STST before and after rehabilitation, the 1′STST improved by 4.00 ± 6.62 repetitions (p = .0013) and correlations were slightly weaker and reached significance only for ∆6MWT (r = 0.51, p = .0012), and ∆QF (r = 0.36, p = .034), but not for ∆VO2max (r = 0.28, p = .11) and ∆Wmax (r = 0.29, p = .09). Association between changes in the 1′STST and 6MWT following a three-month PR program (r = 0.57, p = .002). Baseline data (○) and follow-up data (•) were connected for a given patient. 1′STST, one-minute sit-to-stand test; 6MWT, 6-minute walk test.
Exploratory analysis of the association with PA
A moderate positive correlation was found between the 1′STST and daily step count (r = 0.38, p = .013) and WT (r = 0.38, p = .013) at baseline. No significant correlation was found for MI during walking (r = 0.24, p = .13). In contrast, the 6MWT demonstrated stronger correlations with PA parameters, including step count (r = 0.48, p = .0015), WT (r = 0.45, p = .003), and MI during walking (r = 0.45, p = .0028).
No improvements were found for PA (step count ∆ = 60 ± 1624 steps/day, p = .84; WT ∆ = 1.74 ± 19.35 min/day, p = .63; MI during walking ∆ = 0.03 ± 0.16 m/s2, p = .30). The change in the 1′STST was not correlated to changes in parameters of PA. The change in the 6MWT revealed a moderate correlation only with change in MI during walking (r = 0.50, p = .005), but not with other parameters of PA.
Cardiorespiratory response
Cardiorespiratory responses to the 1′STST, 6MWT and CPET.
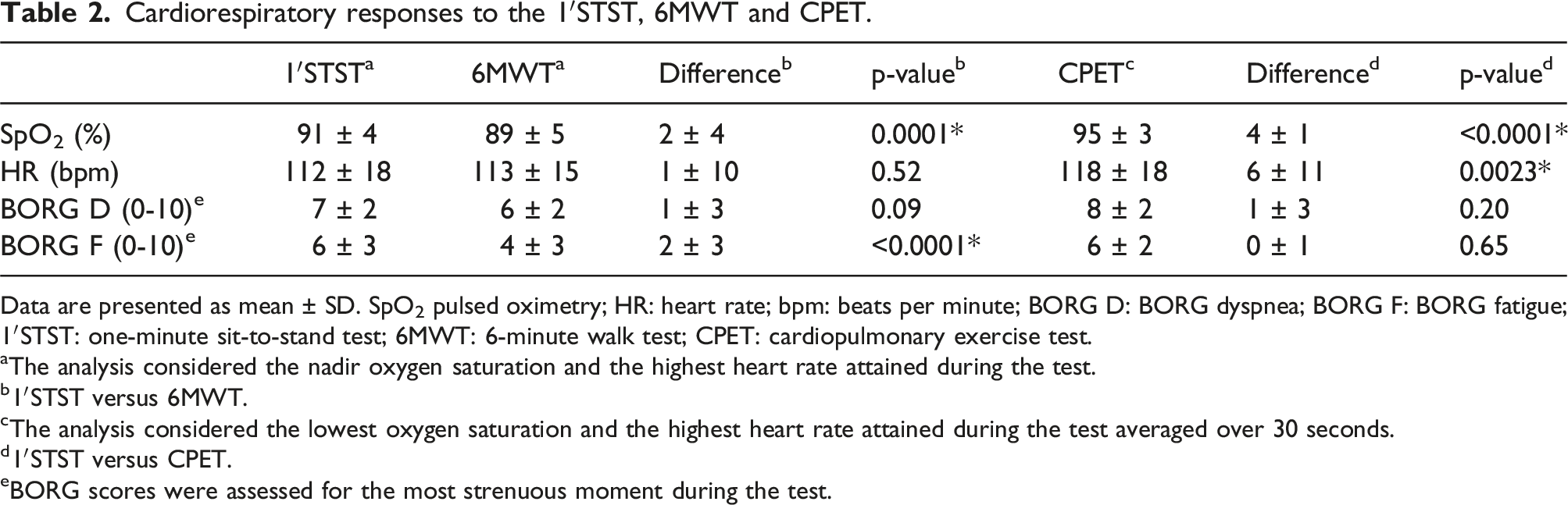
Data are presented as mean ± SD. SpO2 pulsed oximetry; HR: heart rate; bpm: beats per minute; BORG D: BORG dyspnea; BORG F: BORG fatigue; 1′STST: one-minute sit-to-stand test; 6MWT: 6-minute walk test; CPET: cardiopulmonary exercise test.
aThe analysis considered the nadir oxygen saturation and the highest heart rate attained during the test.
b1′STST versus 6MWT.
cThe analysis considered the lowest oxygen saturation and the highest heart rate attained during the test averaged over 30 seconds.
d1′STST versus CPET.
eBORG scores were assessed for the most strenuous moment during the test.
Confirming the minimal important difference
The cut-off of three repetitions in the 1′STST yielded a sensitivity of 71%, a specificity of 71% and an accuracy of 71% to detect an increase of 30m in the 6MWT. The ROC curve resulted in an AUC of 0.78 (see Figure 4). Receiver Operating Characteristics (ROC) curve. The cut-off of three repetitions resulted in the most optimal balance between sensitivity and specificity.
Discussion
The 1′STST confirmed reproducibility, validity, and responsiveness when adopted in clinical practice. Generally, the analyses for the best 1′STST were similar to the analysis using only the initial test. While participation in PR resulted in an increase of 3.6 repetitions, three repetitions was found to be the optimal cut-off for identifying responders.
We observed good test-retest reliability in our study, with an ICC of 0.79, which was slightly less compared to previous studies in COPD (ICCs of 0.9 and 0.93)14,15 and in other patient populations (ICCs of 0.93 and 0.98).40,41 In earlier studies involving patients with COPD,14,15 both tests were performed on the same day, while our study implemented a one-week interval due to the extensive test battery. Previous literature, however, does not suggests that a longer time interval between two tests is per se associated with lower ICCs.17,41–43 In this clinical context, with assessments performed at one-week intervals, fluctuations in the patient’s condition can occasionally happen. This may explain the discrepancies between two test observed in few patients. This is further supported by the ICC of the 6MWT (ICC = 0.77). Additionally, the changes in the 1′STST between visits one week apart exhibited a weak correlation with the changes in the 6MWT on these visits (r = 0.38, p = .0084). Nevertheless, there is no compelling rationale to conduct a second test; a single test effectively captures the effects of rehabilitation. While in 42% and 52% of the patients, the first test emerged as the best test at baseline and follow-up, respectively, differences were generally small and not clinically significant. When patients were classified using a P25 cut-off as an indicator of a “low” test result, 26 only four patients would have their label changed from “low” to “normal” with the introduction of a second test. Thus, we agree with previous reports that – also in clinical practice – a single 1′STST can be used as a valuable screening tool for exercise intolerance.14,16,44 For research purposes, however, a second test may be necessary to obtain a more accurate estimation of the patient’s exercise capacity.
The present study found a moderate correlation between the 6MWT and the 1′STST. However, notable differences were observed in the exercise responses elicited by both tests: lower SpO2 was observed during the longer 6MWT, and participants reported higher fatigue scores during the 1′STST. Both the 1′STST and the 6MWT assess functional exercise capacity through different relevant daily life functions; walking in the 6MWT places a greater demand on cardiorespiratory capacity, while rising from a chair during the 1′STST targets lower limb muscles strength, proprioception, and balance more specifically. Despite these variations, the HR response and dyspnea scores were comparable between the two tests. Our findings align with previous literature demonstrating that both tests elicit a similar cardiorespiratory response, 14 but that oxygen desaturation was more pronounced during the 6MWT, with saturation ranges of 86%–89% during the 6MWT compared to 89%-92% during the 1′STST.14,15,20,45 Others, however, reported less hemodynamic stress in the 1′STST compared to the 6MWT in terms of heart rate, BORG dyspnea and systolic blood pressure. 18 Given that the 1′ STST cannot accurately identify whether significant desaturation would occur during longer exercise bouts, the results on desaturation should be interpreted with caution. The 6MWT may be more appropriate to identify patients who exhibit desaturation. In our cohort, the sensitivity and specificity of the 1′STST for detecting patients with significant desaturation (ΔSpO2≥4% and nadir SpO2<90%) were 33% and 94%, respectively.
The Covid-19 pandemic underscored the importance of valid and responsive physical tests that can be conducted in various settings with minimal equipment, time and space. The 1′STST can serve as a helpful, less time-consuming surrogate when a (quiet) hallway is not available. This test only requires a chair, stopwatch and pulse oximeter, and can be completed in less than five minutes (including the explanation). This makes it particularly suitable for low-resourced settings in hospitals, primary care, or home-based environments. 16 Moreover, it can be more easily utilised in hospital wards whenever patients are capable of standing up independently.
Our study revealed a moderate correlation between the 1′STST with VO2max and Wmax, and their relation over time. Prior research has explored the comparability of VO2max between the 1′STST and CPET, suggesting that both tests elicit similar cardiopulmonary stress. 46 We found a lower saturation during the 1′STST, but a higher heart rate during the CPET; both tests exhibited similar symptom scores, indicating that the 1′STST is perceived to be at least as demanding as the incremental cycling test.
In the present study, a weak, but significant association between quadriceps force and performance on the 1′STST was found. In addition, the change in 1′STST was moderately correlated with the change in quadriceps force after PR. Literature is not unanimous on this relation; one study reported a significant correlation (r = 0.36), 23 while another did not (r = 0.064). 15 The performance on the 1′STST is influenced by factors such as balance, mobility, psychological factors, and metabolic capability, indicating that it is not solely a proxy measure of lower limb strength. 47 Given the relative high metabolic load and high level of perceived fatigue, however, a 30-second sit-to-stand test or five times sit-to-stand test may be a better test of skeletal muscle strength.19,23,47,48
There are currently no established guidelines for using the 1′STST to prescribe a tailored exercise program, although the test can help select patients with poor exercise tolerance for exercise training interventions. 49 Reference values have been provided by Strassman et al.. 26 The intensity of the training program, however, should then be prescribed based on more formal exercise testing. 25
The observed improvement in the 1′STST score following PR aligns with previous studies, which reported improvements of 3.6 ± 4.1 14 and 3.8 ± 4.2 repetitions. 22 An improvement of two to three repetitions is recommended for defining a meaningful improvement in the 1′STST.14,16,22 This was confirmed in our sample, where an improvement of three repetitions yielded the optimal sensitivity and specificity in identifying responders to PR.
This study has the strength that it reflects the use of the test in clinical practice. Previously the test had only been examined within the confines of specific research objectives. In our rehabilitation centre, the test has been implemented in clinical routine. This provided us with the opportunity to evaluate the test in a real-world clinical context, but further research is needed to explore te implementation in a truly primary care setting. Second, this study represents one of the first investigations into the relationship between PA and the 1′STST. Only one previous study examined the relationship between step count and the 1′STST, showing a moderate relationship between both constructs (r = 0.51, p = .0001). 24 Although they found an association, they concluded that the 1′STST cannot be used to predict a very inactive lifestyle. 24 Our data revealed a weak correlation between the 1′STST and step count as well as walking time; the changes in both constructs were not related, reinforcing the thought that the 1′STST is a test of exercise capacity, which increases with exercise training, whereas PA is a behavior that does not change unless behavior interventions are applied. 50 Using the combination of the 1′STST and objectively measured PA could allow clinicians to classify patients as appropriate achievers, underachievers or overachievers, as had been done using the 6MWT. 51 The 6MWT did show a somewhat stronger relation to PA,24,52 also in the present cohort.
In conclusion, our results confirm that the 1′STST can serve as a reliable and valid measure of functional exercise capacity in individuals with COPD. In clinical practice, the present study demonstrates reliability, validity, and responsiveness to pulmonary rehabilitation. The 1′STST requires less time and space, making it easily implementable in a wide range of healthcare settings.
Supplemental Material
Supplemental Material - The one-minute sit-to-stand test: A practical tool for assessing functional exercise capacity in patients with COPD in routine clinical practice
Supplemental Material for The one-minute sit-to-stand test: A practical tool for assessing functional exercise capacity in patients with COPD in routine clinical practice by Paulien Mellaerts, Heleen Demeyer, Astrid Blondeel, Tim Vanhoutte, Sofie Breuls, Marieke Wuyts, Iris Coosemans, Lode Claes, Nele Vandenbergh, Kaat Beckers, Lucas Vanden Bossche, Dimitri Stylemans, Wim Janssens, Stephanie Everaerts and Thierry Troosters in Chronic Respiratory Disease.
Footnotes
Acknowledgments
The authors acknowledge the assistance of Charlotte Amerijckx, Arne Beckers and Yiting Cui.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.