
Abstract
Patients with chronic obstructive pulmonary disease (COPD) who participate in pulmonary rehabilitation (PR) often have concomitant cardiovascular disease (CVD), which is a frequently undiagnosed and undertreated comorbidity. CVD contributes to the burden of the disease and is associated with an increased risk for hospitalizations and mortality. Optimizing the diagnosis and management of cardiovascular risk and disease should be considered as part of the holistic approach of PR. In addition, we need to consider similarities and differences in cardiac and PR programs, in order to improve personalized care in patients with both diseases. The current review addresses the burden of CVD in COPD patients who participate in PR, how CVD and its risk factors affect PR and should be managed during PR, and extends on what we can learn of the organization of cardiac rehabilitation programs.
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex and heterogeneous disorder, in which multiple extrapulmonary manifestations and comorbidities importantly contribute to the individual burden of the disease. 1 Of these, cardiovascular comorbidities are the most prevalent and impactful 2 but also among the most frequently undiagnosed morbidities beyond the lungs in patients with COPD. 3 Addressing, sometimes multiple, undiagnosed or undertreated comorbidities during PR, might offer a unique opportunity for personalized and holistic medicine in patients with COPD, with an important potential to reestablish health. 4 Given the frequency and impact, it is important to consider cardiovascular disease (CVD) in patients with COPD entering PR, in order to create patient-tailored and safe rehabilitation programs and adapt education, and enhance behaviors regarding healthy lifestyle adherence for both respiratory and cardiac diseases. For this review, we aim to study the literature regarding (1) the occurrence and consequences of CVD in patients with COPD entering PR, (2) how CVD affects PR and whether or not PR might influence cardiovascular risk, and (3) distillate lessons from cardiac rehabilitation (CR) programs.
The prevalence and importance of CVD in PR
High prevalence of CVD in PR
CVD and its classical risk factors (ageing, smoking, sedentary life style, obesity and metabolic diseases) are common in patients with COPD. A systematic review showed a nearly 2.5 times increased risk of CVD overall, and a two to five times higher risk of major CVD types (ischemic heart disease, cardiac arrhythmia, congestive heart failure (CHF), diseases of the pulmonary circulation, and arterial diseases) in patients with COPD, compared to matched controls or random samples from the general public. 5 Also cardiovascular risk factors, like hypertension, hyperglycemia, dyslipidemia, increased intima-media thickness, and arterial stiffness have shown to be highly prevalent in COPD. 6,7 Comorbid CVD increases the complexity of the patient with COPD, as it is associated with more symptoms, 2 impaired survival, 8 and increased risk of hospitalizations, 9 irrespective of the degree of airflow limitation. Complex COPD patients are often referred for PR. It may come as no surprise that a diagnosis of CVD and/or identifiable risk factors is particularly prevalent in subjects entering PR. Crisafulli et al. showed that the majority of COPD patients entering a PR program reported comorbid metabolic or cardiovascular issues. 10 The high prevalence of CVD or risk was confirmed using objective measures in the CIRO comorbidity study (CIROCO). 11 Importantly, the objective measures did not match the chart-based diagnosis, emphasizing the need for a thorough evaluation of the medical history and additional objective testing for comorbidities. Only 21.1% of patients with electrocardiogram (ECG) changes, compatible with prior myocardial infarction, were previously known with this diagnosis. Similarly, in those with objectively identified dyslipidemia and diabetes mellitus, only 14.0% and 26.7% of patients, respectively, were previously known with this disease. Conversely, clinical evaluation remains a valuable addition to objective testing in case of treatment effects or limitations of the method of assessment. 3
Influence of CVD on PR outcomes
Although CVD is highly prevalent in COPD patients entering PR, information on the influence of CVD on PR outcomes is scarce. Crisafulli et al. was the first to analyze retrospectively the effects of different groups of self-reported comorbidities on the outcomes of PR. 10 The results were heterogeneous. In the multiple logistic regression analysis, metabolic diseases reduced the probability to reach the minimal clinical important difference (MCID) for the six-minute walking distance (6MWD; odds ratio (OR) 0.57 (96% confidence interval (CI): 0.49–0.67)), whereas heart diseases (OR 0.67 (96% CI: 0.55–0.83)) reduced the probability to reach the MCID for St George’s Respiratory Questionnaire (SGRQ). In contrast, the presence of heart disease was a predictor for clinical relevant improvement of walking distance (OR 2.36 (96% CI: 1.85–3.01)). To further elucidate these interactions, the authors performed a similar, but prospective study. Interestingly, in this study no individual or grouped comorbidity significantly influenced the probability of achieving the MCID for any of the outcomes, with the exception of osteoporosis which seemed to impact on walking distance. 12 More recently, Mesquita et al. evaluated the objectively identified comorbidities and clusters of comorbidities in the CIROCO study against conventional PR outcomes. 13 Interestingly, no individual cardiovascular or other comorbidity influenced the likelihood of achieving clinically important benefit on exercise capacity (6MWD and constant work cycling test) and quality of life (SGRQ). More interesting was the comparison of different comorbidity clusters in terms of rehabilitation outcomes, as these multimorbidity groups reflect the clinical reality. Both clusters with increased Framingham cardiovascular risk score, one named “cardiovascular”, the other “metabolic” (based on differences in metabolic comorbidities) did not have a significant different response compared to the cluster with less comorbidities. However, the study might have been underpowered and patients belonging to the metabolic cluster tended to have a higher probability to improve their quality of life (OR 2.09 (95% CI: 0.97–4.50) p = 0.06), while they were less likely to improve their walking distance (OR 0.57 (95% CI: 0.29–1.15) p = 0.12). The latter might not be surprising because walking is a weight-bearing exercise and patients belonging to the metabolic cluster were more likely to be obese. 13 Overall, we can conclude that comorbid CVD is not a reason to withheld patients from rehab programs.
Can PR lower the cardiovascular risk in patients with COPD?
Current influence of PR on cardiovascular risk
Several features of PR, such as exercise and nutritional intervention have the potential to address the cardiovascular risk. PR also reduces symptoms of depression and anxiety, 14 which are both associated with CVD. 15,16 However, its effects on short- and long-term cardiovascular risk in patients with COPD have not been uniformly established. In COPD patients with a concomitant metabolic syndrome, pulmonary rehabilitation (PR) can reduce waist circumference and could decrease fasting glucose. 17
Arterial stiffness, a robust predictor of cardiovascular risk, has repeatedly shown to be increased in patients with COPD. 7,18,19 In young healthy people, short-term endurance exercise training can decrease arterial stiffness. 20 However, the effects of exercise or rehabilitation programs on arterial stiffness in different patient populations have been diverse. 21 In patients with COPD, two studies with a limited number of patients have shown a significant improvement in arterial stiffness after endurance training. 22,23 Both studies excluded patients with diabetes mellitus, one also excluded patients with other metabolic conditions, known ischemic heart disease and CHF. Contrary, in a larger study, including 162 COPD patients with a mean age of 64 years with multiple comorbidities, no change in average aortic pulse wave velocity was noted after PR, despite sufficient training intensity. 7 An adequately powered randomized controlled trial is needed to further establish the role of PR in reducing arterial stiffness. 24
Moving forward: Assessment of cardiovascular risk in patients entering PR
Cardiovascular risk assessment and management is an important component of the initial evaluation at the start of a PR program. This as a part of the integrated approach that PR stands for, as also for reasons of optimal management and safety. 5 The PR assessment offers a unique opportunity to systematically screen for cardiovascular risk factors (questionnaire, body mass index measurement, dyslipidemia, metabolic syndrome, cardiovascular risk using a validated scoring system, etc.), or established CVD (medical history review, concise structured interview and physical examination, ECG, plasma brain natriuretic peptide measurement). Similarly, a maximal cardiopulmonary exercise, commonly used to evaluate training load in patients, might reveal dynamic ECG changes and help to assess the safety of exercise. 25 Both in COPD and CHF, the incremental shuttle walking test combined with telemetry has also been used for patient assessment. 26 –28 Cardiac evaluation including echocardiography is recommended for COPD patients who have signs of CHF and/or concerning symptoms, such as exertion-related dizziness or chest pain. 25 Interventions should include a rigorous management of the classical modifiable cardiovascular risk factors such as smoking status, dyslipidemia, arterial hypertension, diabetes mellitus, obesity, and lifestyle.
Dealing with CVD during PR
Safety of cardio-PR programs
General considerations
Exercise training has been shown to be safe in CR. The occurrence of major cardiovascular events (myocardial infarction or cardiac arrest) during exercise ranges from 1/50,000 to 1/120,000 patient-hours of exercise. 29 For all patients participating in PR, contraindications to exercise training should be checked prior to and at the beginning of the assessment as described above. These are similar to the contraindications for CR (Table 1). Recommendations for exercise discontinuation should also be followed. In patients with an implantable cardioverter-defibrillator (ICD), exercise heart rates should not reach higher than 10–15 beats below the ICD tachycardia threshold.
Contraindications for cardiac rehabilitation. 30

CR: cardiac rehabilitation.
Exercise-induced desaturation
The Global Initiative for Chronic Obstructive Lung Disease advocates long-term administration of oxygen in patients with COPD with a PaO2 at or below 7.3 kPa (55 mmHg) or SaO2 at or below 88%. In patients with pulmonary hypertension, peripheral edema suggesting CHF, or polycythemia, long-term administration of oxygen is also recommended at a PaO2 between 7.3 kPa (55 mmHg) and 8.0 kPa (60 mmHg). 31 Management of exercise-induced desaturation for COPD patients with concomitant CVD is less investigated than for patients with COPD in general. 32 However, CHF is characterized by impaired oxygen delivery to working muscles. Exercise performance for patients with CHF has been shown to be better at low altitude associated with an increase in oxygen saturation and cardiac output. 33 Severe oxygen desaturation during exercise also seems undesirable in patients with ischemic heart disease, but its effects have not been established. Therefore, it could be considered to prescribe oxygen during training in normoxemic patients with concomitant heart disease who show desaturation below the arbitrary level of 85% and to adjust the oxygen suppletion with exercise in patients that already use long-term oxygen therapy for rest hypoxaemia.
How to manage cardiac comorbidities during PR?
Patients with known CVD should be optimally medically treated and have stable disease. 34 For patients with CHF, weight and fluid management are important features during rehabilitation. Patients on diuretics are at risk for renal dysfunction and electrolyte imbalances and blood sample analysis should be considered. The rehabilitation team should be knowledgeable and have basic clinical skills and consideration of safety aspects regarding CVD. Therapists should be aware that signs and symptoms of CHF, myocardial ischemia, and COPD, which may be hard to distinguish. The presence of a member of the rehabilitation team skilled in advanced life support and readily available defibrillation equipment should be considered in high-risk patients. 35
Similar to education on respiratory disease, patients with concomitant CHF should be provided disease-specific education during the program or should be referred to another health care professional for this purpose. 34 Education topics can include, for example, the heart and its function, cardiovascular risk factors and pathologies, cardiology investigations, warning signs (such as angina), self-assessment techniques (blood pressure, glycemia, weight monitoring), fluid and salt restriction, medications, and life-saving measures. 35 In patients with coronary heart disease, an antiatheromatous diet should be provided, together with education and practical workshops. 35 As in COPD, depression, mood disorders, and smoking cessation should be addressed. 35
What can we learn from CR?
Cornerstones in CR
As for PR, CR has evolved to a holistic, patient-tailored approach, which addresses the underlying CVD, as well as physical, mental, and social conditions, so that the patients may function optimally and improve health behavior. Cornerstones of both CR and PR include health behavior change and education, smoking cessation, psychological health, optimizing medical therapy, long-term management, audit, and evaluation. 25,36 Patient-tailored treatment options can be discussed in the setting of both CR (i.e. implantable cardiac defibrillators and/or cardiac resynchronization therapy) as PR (i.e. non invasive ventilation in hypercapnic respiratory failure, lung volume reduction in severely hyperinflated patients, or referral for lung transplantation assessment).
The focus of CR was traditionally aimed at the secondary prevention of CVD events, predominantly for patients after a myocardial infarction or cardiac surgery, excluding patients with CHF. 37 However, based on patient characteristics, similar to those of patients with COPD, exercise training has emerged as a key component for CR in patients with CHF. 34,35 The systemic consequences of COPD and CHF show considerable similarity, including skeletal muscle dysfunction, mood disturbances, osteoporosis, hormonal alterations, and anemia. 34 Factors such as hypoxemia, disuse, aging, nutritional depletion, medication use, systemic inflammation, and smoking can contribute to skeletal muscle dysfunction, early onset of peripheral muscle fatigue, and impaired endurance performance. Low exercise tolerance, in turn, has a large influence on health status in both disorders. 38 Whereas secondary prevention is the primary treatment goal in asymptomatic patients participating in CR, symptomatic patients might experience exertional breathless, fatigue, and functional impairment. In these patients, improving function and health-related quality of life become important treatment goals, closely resembling to treatment goals in patients with COPD.
Is it CR in pulmonary patients, what’s in a name?
As mentioned above, exercise intolerance in patients with COPD and CHF is multifactorial and shows considerable similarity, involving ventilatory, gas exchange, cardiovascular, and peripheral muscle abnormalities. However, dynamic lung hyperinflation during exercise is specifically related to COPD, further impairing the balance between ventilatory capacity and demand during exercise, exacerbating dyspnea. Abnormalities in gas exchange in patients with CHF are mainly based on regional hypoperfusion but not ventilation inhomogeinity. 39
The physical aspects of rehabilitation for both COPD and CHF patients are nowadays better described as cardiopulmonary rehabilitation. Exercise programs, including aerobic, interval, and strength training are comparable and benefits of CR and PR are similar (Table 2). 25,40 –42 Neuromuscular electrical stimulation has shown to improve several physiologic, exercise, symptomatologic, and quality-of-life parameters both in patients with heart failure and COPD. 43,44 Inspiratory muscle training has also been used in CR. 43 Besides, the role of inspiratory muscle training in patients with COPD is still being explored. It has shown to reduce dyspnea during activities of daily living; improvements in walking distance and small gains in health-related quality of life have been reported. 25 However, if added to whole body exercise, which per se leads to substantial improvements in exercise capacity, dyspnea, and health-related quality of life, detecting further improvement has proven more difficult. 25 Thus, currently inspiratory muscle training is not consistently recommended in addition to exercise and its use may be limited to subjects who cannot adequately perform whole body exercise. However, a large, adequately powered, multicenter randomized trial is currently being performed in COPD patients with inspiratory muscle weakness. 45 Educational topics are evidently different than for CR. Dyspnea management is a cornerstone in PR, but is also important in CHF.
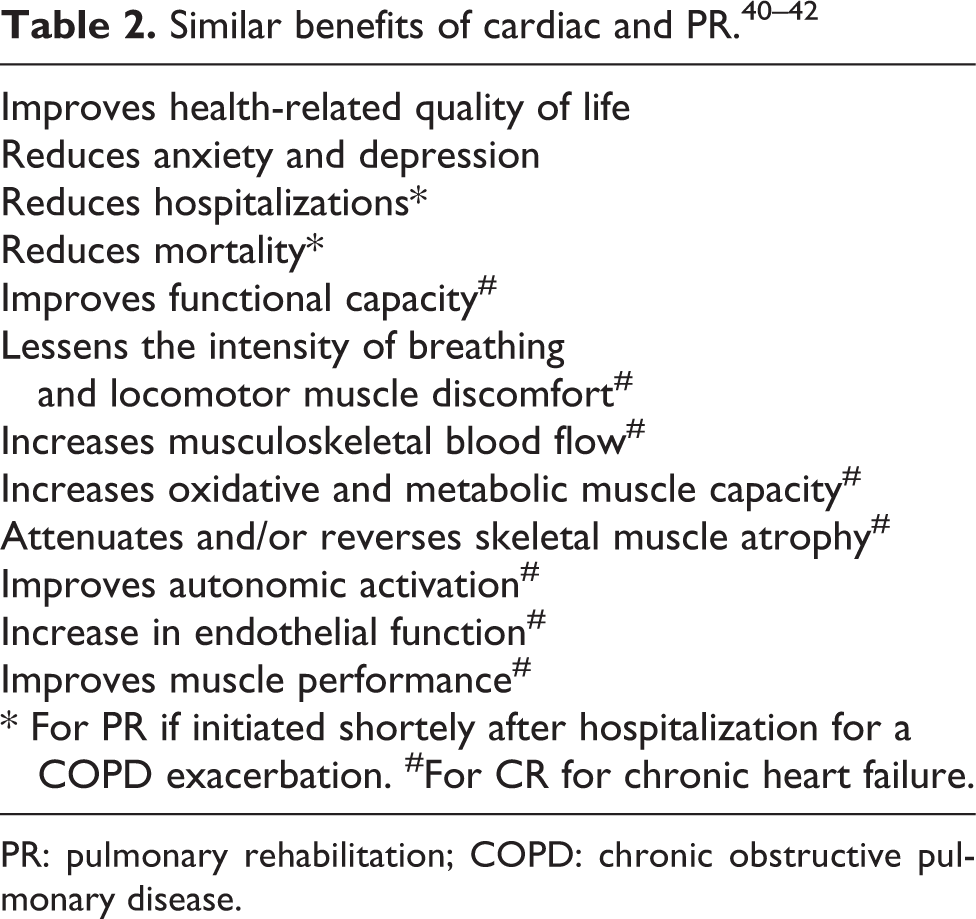
PR: pulmonary rehabilitation; COPD: chronic obstructive pulmonary disease.
Some interventions are specific for PR. Proportional assist ventilation can allow a higher intensity of training in patients with severe COPD, leading to greater improvements in maximum exercise capacity. 46 Although not widely used, some benefits of helium–hyperoxic gas mixtures in addition to exercise have been reported. 25
Lessons from the organization of CR
The British Association for Cardiovascular Prevention and Rehabilitation rigorously advocates offering CR programs to all eligible patients via an agreed and coordinated patient referral and/or recruitment process. The initial assessment should be from a member of the CR team as part of in-patient care for those admitted to hospital, in order to maximize service uptake. 36,47 The earliest stages of CR, the identification, referral, and recruitment to CR begin as soon as possible after admission (e.g. for an acute myocardial infarction) and before discharge from hospital. 48 The patient is invited to a CR session which should start within 10 days of their discharge from hospital.
An acute exacerbation of COPD, for patients communication could be described as a lung attack, in resemblance to a heart attack. A first episode of a lung attack, and certainly first hospitalization gives a window of opportunity for early PR. Early PR following hospitalization for an acute COPD exacerbation has shown to be feasible and beneficial. In 2004, Man et al. showed that early PR, compared with usual care, led to significant improvements in walk distance and quality of life. 49 In 2010, Seymour et al. randomized 60 patients, hospitalized for an acute COPD exacerbation, to receive either usual care or to participate in an outpatient PR program within a week after hospital discharge. They showed a reduction from 33% to 7% in hospital admissions over a 3-month period if patients were started on rehabilitation (OR 0.15, 95% CI: 0.03–0.72, p = 0.02). 50 Still, referral rates for early PR following hospitalization for acute COPD exacerbations are poor. 51
The British Association for Cardiovascular Prevention and Rehabilitation also advocates that a menu-based approach, delivered in easily accessible venues, provides for the greatest chance of uptake and adherence to the CR program. For example, patients with mild COPD might need more secondary prevention than dyspnea management. The choice in terms of venue (including home) and time (e.g. early mornings and evenings) should meet a patient’s individual needs. 34,47 Home-based exercise training, delivered after an educational program, has proven effective in reducing dyspnea 52 and increasing exercise performance 53 in patients with COPD. However, thus far there seems to be more diversity in CR than in PR with the use of technology and location. 54 Telehealthcare, through phone calls, websites, or mobile phones, often combined with education and/or exercise training, has also been investigated and may lead to improvements in physical activity levels, but study methodologies and outcomes are heterogenous. 55 These modalities are currently being further explored in patients with COPD. 56
Both in CR and PR, patients should develop self-management skills and become empowered to take ownership of their own responsibility to pursue a healthy lifestyle. Caregivers and family should also be equipped to contribute to long-term adherence by helping and encouraging the individual to achieve their goals. Patients should be signposted and encouraged, where appropriate, to join local support groups, community exercise and activity groups, community dietetic and weight management services, smoking cessation services. 36 In the absence of a maintenance strategy, the benefits of PR appear to diminish over 6–12 months, so long-term management is an essential feature of PR. The effects of maintenance exercise training programs, ongoing communication to improve adherence, and repeating PR remain univocal, 57 but different formats should be further explored. There is a need for ongoing peer support, through group activities with other COPD patients who have similar needs and experiences. 25 There is also a growing interest in the interaction between patients with COPD and their informal caregivers, which play an important role in improving the quality of life of both patients and their informal caregivers and save healthcare costs. 58 Table 3 summarizes some potential points of improvement for PR, based on the organization of CR and the prevalence and importance of CVD in patients with COPD.
Potential points of improvement for PR in COPD.

COPD: chronic obstructive pulmonary disease; CVD: cardiovascular disease; PR: pulmonary rehabilitation.
Conclusions
PR and CR share similar features and organizational needs. Early systematical recruitment of patients, including in-hospital recruitment during the first hospitalization for a COPD exacerbation, a menu-based approach to deliver easily accessible rehabilitation, and maintenance strategies to preserve benefits from rehabilitation should be further explored. CVD and its modifiable risk factors are frequent, often undiagnosed and insufficiently treated comorbidities, which importantly contribute to morbidity and mortality in patients with COPD. Therefore, systematical cardiovascular risk management and screening for CVD should therefore be a component of PR. An adapted integrated cardiopulmonary rehabilitation for COPD patients with concomitant CVD should be provided with consideration of medical management, training intensity, safety issues, educational topics, and dietary intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.