
Abstract
Background
Early commencement of rehabilitation might counteract the loss of muscle strength due to a chronic obstructive pulmonary disease acute exacerbation (COPDAE). Blood flow restriction resistance exercise (BFR-RE) using a low intensity of training load has demonstrated muscle strength gain in varieties of clinical populations. This trial aimed at studying the efficacy and acceptability of BFR-RE in patients with post-COPDAE which was not reported before.
Method
A prospective, assessor blinded, randomized controlled study with 2-week in-patient rehabilitation program with BFR-RE was compared to a matched program with resistance exercise without BFR in patients with post-COPDAE. The primary outcome was the change of muscle strength of knee extensor of dominant leg. The secondary outcomes included changes of hand grip strength (HGS), 6-minute walk test (6MWT) distance, short physical performance battery (SPPB) scores, COPD assessment test (CAT) scores; acceptability and feasibility of BFR-RE; and 1-month unplanned re-admission rate.
Results
Forty-Five post-COPDAE patients (mean age = 76 ± 10, mean FEV1%=49% ± 24%) were analyzed. After training, BFR-RE group and control group demonstrated a statistically significant median muscle strength gain of 20 (Interquartile range (IQR) 3 to 38) Newton(N) and 12 (IQR -9 to 30) N respectively. BFR-RE group showed a significant change in SPPB scores, but not in 6MWT distance and HGS after training. Between groups did not have statistically significant different in all primary and secondary outcomes, though with similar acceptability. Drop-out rate due to training-related discomfort in BFR-RE group was 3.7%.
Conclusion
BFR-RE is feasible and acceptable in patients with post-COPDAE. A 2-week inpatient pulmonary rehabilitation with BFR-RE improved muscle strength of knee extensors, but not a greater extent than the same rehabilitation program with resistance exercise without BFR. Further studies could be considered with a longer training duration and progression of resistance load. [ClinicalTrials.gov Identifier: NCT04448236].
Keywords
Introduction
The global prevalence of chronic obstructive pulmonary disease (COPD) among people aged 30–79 years in 2019 was 10.3% (95% CI 8.2–12.8) which translated to 391.9 million people (95% CI 312.6–487.9). 1 The mortality of a COPD exacerbation was 15.6% (95% CI 10.9%–20.3%). 2 The local COPD prevalence of Hong Kong was 12.4% defined by lower limit of normal range of FEV1/FVC ratio. 3 The annual COPD hospital admissions under Hospital Authority was around 20,000 per year. 4
Muscular dysfunction is one of the extra-pulmonary morbidity of COPD. 5 Peripheral muscle force was found to be significantly reduced during COPD acute exacerbation. 6 Quadriceps weakness was found in approximately one third of patients with COPD. 7 Reduced muscle strength was associated with increased mortality in moderate to severe COPD. 8
Muscle strength is about the ability of the muscle to exert a maximal force on one occasion which is affected by disease states and reversed by rehabilitation via resistance training. Traditionally, 60 to 70% of 1-repetition maximum (1-RM) of training load is suggested in high-load resistance training to achieve muscle growth. 9 Though this load might not be feasible, particularly to patients admitted for post-COPD acute exacerbation (COPDAE) rehabilitation with decreased general condition.
Blood flow restriction resistance exercise (BFR-RE) training, also known as Kaatsu training, was developed by Dr Yoshiaki Sato more than 40 years ago. 10 The crux of the BFR-RE training is that it can use a lower training load (approximate 15 to 30% of 1-RM) to achieve the gain of muscle strength and mass. 11 This training method applies external pressure (80% of limb occlusion pressure) via external constricting device to proximal part of the limb to occlude venous drainage of muscle but allowing certain arterial supplies, leading to a pooling of blood in the capillary beds of the limb musculature distal to the device.
BFR-RE is postulated to induce metabolic stress by creating an ischemic/hypoxic environment leading to secondary mechanisms to muscle growth, e.g. cell swelling, nitric oxide production, fast twitch muscle fiber (Type II) recruitment, satellite cell activity via paracrine actions, etc. The mechanical tension, as another primary mechanism, might also have synergistic effect with the metabolic stress during BFR-RE, though contributing lesser extent if using low load for resistance training. 12
Concerning the growth of muscle mass, BFR-RE training led to a comparable increase when compared to high-load resistance exercise (HL-RE). 13 However, concerning the increase of muscle strength, BFR-RE was less effective than that in HL-RE but more effective than that in low-load resistance exercise (LL-RE) alone. 13 Therefore, BFR-RE can be considered when HL-RE training is not advisable (e.g. frail elderly, post-operative rehabilitation) since lower intensity load is required.
BFR-RE training was well studied among healthy adults, 13 elderly 14 and patients for musculoskeletal rehabilitation, 15 but not in patients with COPD, except a case report using BFR-RE as an initial training to prepare a load-compromised patient with COPD for subsequent high-load strength and endurance training in an outpatient pulmonary rehabilitation program. 16 A recent descriptive qualitative study showed that patients with COPD and health professionals recognized BFR-RE with low load as an alternative exercise method with potential health benefits since the adherence of training might be compromised by the traditional high load and showed concerns on the adverse events during BFR-RE. 17 A review demonstrated the side-effects were minimal and the cardiovascular complications were not elevated by BFR with appropriate application by trained practitioners after careful case selection and contraindication screening. 18
The effect of BFR-RE on muscle strength in hospitalized patient with post-COPDAE, which has not been studied, was the primary outcome of this study. Improvement of functional tests, health related quality of life and 1-month readmission rate after current discharge were explored as secondary outcomes. Since BFR-RE was not formally used in Hong Kong, the acceptability and feasibility of this training modality were assessed as well.
Objectives
The primary outcome of the study was to compare the change of localized muscle strength19,20 in term of maximal voluntary isometric contraction (MVIC) of knee extension of the dominant leg with or without blood flow restriction (BFR) on the same low-load resistance exercise training in the conventional in-patient pulmonary rehabilitation program.
The secondary outcomes of the study were to investigate any functional improvement in term of Short Physical Performance Battery (SPPB), 21 6-min walk test (6MWT), 22 any change of systemic muscle strength in term of hand grip strength,23,24 any change of health-related quality of life in term of self-administered Chinese version of COPD assessment test (CAT)25,26 and any difference of unplanned readmission rate for acute exacerbation within 1 month after current discharge with additional BFR to resistance exercise in in-patient pulmonary rehabilitation program.
The acceptability of BFR-RE was explored in the study in term of “Pain score” before, immediate and 5-min post exercise measured by visual analog scale (0 to 10). Participants’ acceptance was self-rated by a “5-point Likert categorical scale” after the whole program. Drop-out rate and reasons of drop-out were assessed to determine the feasibility of BFR-RE.
The current study was to evaluate the hypothesis that low-load resistance training with BFR demonstrates more muscle strength gain, better functional improvement and similar acceptability/feasibility than conventional low-load resistance training without BFR in patients with post-COPDAE.
Study design
Subjects
Exclusion criteria.

*Active malignancy is defined by not received potentially curative treatment, or having ongoing treatment, or having recurrent or progressive disease after treatment. 43
COPD=Chronic Obstructive Pulmonary Disease.
MRSA = Methicillin–resistant Staphylococcus aureus.
Randomization
Blocked and stratified randomization method were applied. Based on the pilot phase of the study, subjects were stratified by baseline maximum voluntary isometric contraction (MVIC) (≥ 240N (Newton) or < 240N), which was the median derived from a pilot test, before randomization. Randomization list was generated by computer.
Blinding
Outcome assessments at recruitment and on discharge were carried out by blinded physiotherapists without knowledge of patient’s treatment groups. Study subjects, doctors, nurses and involved physiotherapists for training were for obvious reasons not blinded.
Intervention
A 2-week in-patient interdisciplinary standardized pulmonary rehabilitation program was providing to both groups included breathing exercises, bronchial hygiene, health education, low-load resistance exercise (15%–30% of 1 repetition maximum (1-RM) as tolerated), aerobic training in the form of walking exercise under supervision of physiotherapist with frequency of 5 times per week, intensity of rate of perceived dyspnea (RPD) of 4-6 (10 points scale), duration of 20 minutes or as tolerated, activity of daily living training by occupational therapists, and dietitian advice to ensure adequate nutrient intake.
Patients from both BFR-RE group and control group with supervision by physiotherapists individually underwent the low-load resistance exercise training which was standardized with isotonic knee extension, 5-6 sessions per week for 2 weeks. Patients who had completed at least 10 sessions in 2 weeks’ period were included for outcome analysis. Single limb was trained in each session. The patient was lying on bed horizontally with knee being supported at popliteal fossa at 150° flexion initially and performed isotonic knee extension to 180°. Alternate limb was under training on alternate day (i.e. each limb had resistance training 2-3 times per week). The first set was 30 repetitions followed with 3 sets of 15 repetitions with 30 seconds rest period between each set. The execution speed was 1-2 seconds in each repetition until completion or contraction failure. 30 Physiotherapists ensured the adherence of the training by direction supervision and offered verbal encouragement. Low-load resistance of 15%–30% of 1 repetition maximum (1-RM) was used for resistance exercise using sandbags. 11
1-RM was calculated by formula derived from maximum voluntary isometric contraction (MVIC). This formula was based on the study of 176 in-patient elderlies in Japan (352 legs) 31 : 1RM (kg) = 0.188 + 0.187 × MVIC (kgf). The unit of kg-force (kgf) is a non-SI unit for force previously used in the referenced Japanese study. 31 According to the National Institute of Standards and Technology, 1 kgf is equal to 9.8 Newton(N). 32 1kgf was taken approximately to 10N in the current study for simplicity.
The BFR-RE group was supervised by BFR-training-certified physiotherapists and underwent the above-mentioned resistance training in the physiotherapy gym with a medium size of “Delfi’s Easi-Fit Tourniquet cuff” of the PTS Personalized Tourniquet System (Delfi Medical Innovations Inc.) with 80% limb occlusion pressure (LOP) 33 which is placed at the most proximal thigh with maximum 10 minute of restriction time as a safety measure. The applied pressure is automatically measured by the cuff according to the personalized LOP with pre-set protocol in the system. The cuff was inflated just before the first set of training, maintained during the inter-set rest period and deflated immediately after the final set.
The control group performed the same above-mentioned resistance training without the pressure cuff under the supervision of physiotherapist.
Data collection and outcome measures
Baseline demographics and clinical information of subjects were collected. Primary and secondary outcomes were assessed at baseline and after completion of training (i.e. at least 10 sessions of training).
Maximum voluntary isometric contraction (MVIC) was measured by the computer dynamometer (Primus RS BTE, The Technology of Human Performance, USA). Three submaximal warm-up contraction trials are given with 1-minute rest afterwards. Three trials of MVIC with 1-minute rest between each trial were instructed. After a build-up phase of 2s, an MVIC was needed to be in a steady, maximal contraction, with a plateau phase of 3s. 20 Hand grip strength (HGS) was measured by hand-held dynamometer (JAMAR) by taking average in 2 trials by the dominant hand. 23 Though no specific training for HGS in the program, it was recorded because in some studies showed after BFR-RE, apart from the target muscle increased muscle strength, general muscle strength also increased as a systemic effect of BFR, 34 thus it was used as a surrogate marker to reflect the systemic response. 6-minute walk test (6MWT) was performed according to guideline. 22 The Short Physical Performance Battery (SPPB) 21 is a standardized objective tool to assess the lower limb function consisting 3 components: standing balance, 4-m gait speed (4MGS), and five-repetition sit-to-stand motion (5STS). Each component has its subscale of 0-4. Total summary score is 12. If the SPPB score is less than 10, it indicates mobility limitation. COPD assessment test (CAT)-Chinese version 25 is a self-administered questionnaire about health-related quality of life containing 8 questions and 6 points each (0 to 5) and validated to be administrated in Asians. 26 Higher score means worse health status.
Delayed onset of muscle soreness (DOMS) 35 presents as a range from slight muscle stiffness that quickly disappears during daily routine activities, to debilitating pain that restricts movement. The tenderness mainly concentrates in the distal part of the muscle and diffuses progressively by 24 to 48 h post exercise. The presence or absence of DOMS was documented by physiotherapists before each training session. Acceptability of resistance exercise was reflected in a visual pain analog scale (0 to 10) performed before, immediate and 5-min post exercise by the physiotherapist in each training session with 0 mark indicating no pain and 10 marks indicating maximal pain. A 5-point Likert categorical scale after the whole program was used to assess the preference of the subject towards the whole program. Drop-out rate and reasons of drop-out were used to examine the feasibility of practice. 1-month unplanned readmission rate and reasons of readmission (COPDAE related or not-COPDAE related) were analyzed.
Blood sample for creatinine kinase and urine sample for myoglobulin were checked before and after the in-patient rehabilitation program in both groups to screen for any evidence of muscles injury, particularly rhabdomyolysis.
Statistical analysis
Owning to no published literature of in-patient post-COPDAE pulmonary rehabilitation program with BFR-RE, an accurate estimation of the sample size of this study was impossible. Therefore, a priori power analysis was based on a study with 6-week training of BFR-RE in elderly subjects with mean age of 76.5-year-old was taken as a guidance. 36 In order to have a power of 80% to detect a difference muscle strength gain at the 0.05 level of significance, 18 patients were needed in each group, with a total sample size of 36. Previous pilot conducted in Haven of Hope Hospital showed a sample loss of 10%. Since BFR-RE was a new modality of treatment with unknown acceptance and drop-out, a higher dropout rate of 30% was adopted taking into accounts of BFR-related or logistically-related reasons (e.g., hospitalization less than 2 weeks, hospital infection contact precaution requirement), hence 52 patients in total were targeted for the study.
Data were shown in means with standard deviation or medians with inter-quartile range. Shapiro-Wilk test was used to test the distribution of normality of data. Related-samples Wilcoxon Signed Rank test was used to examine the within-group differences. Independent Sample T test or Mann-Whitney U test was used to analyze the between-group differences of the continuous data. Fisher’s Exact Test or Likelihood Ratio Chi-Squared test was used to demonstrate the between-group differences of the categorical data. A probability value of < 0.05 was considered to be statistically significant. As the study was meant for evaluation of treatment efficacy, therefore per protocol analysis was used in the study. Statistical analysis was performed SPSS version 26.0.
Ethics
The study was conducted in accordance with the principles of the Helsinki Declaration and approved by the Kowloon Central Cluster/Kowloon East Cluster Research Ethics Committee (Reference no.: KCC/KEC-2020-0090).
Results
Total 1021 patients with various respiratory diseases admitted to respiratory wards were screened. 166 patients with post-COPDAE met the inclusion criteria while 113 patients were excluded. (Table 1) Thus, 53 patients were recruited to the study. Six patients dropped out in the study due to non BFR-RE related reasons, e.g. unpredicted early discharge due to personal reasons leading to less than 2 weeks of hospitalization, requirement of contact precautions according to the hospital infection control team. The training-related drop-out rate in the blood flow restriction resistance exercise (BFR-RE) group was 7.4% (2 out of 27 patients) while none in the control group. So finally, results of 45 patients were analyzed. (Figure 1) Recruitment flowchart.
Baseline and clinical characteristics between groups
Baseline characteristics between BFR-RE and control group.

amean ± Standard deviation.
bMedian (Interquartile range).
cCount (% of n).
dTested by Independent sample T test.
eTested by Fisher's Exact Test.
fTested by Likelihood Ratio Chi-Square Test.
gTested by Mann-Whitney U Test.
Statistically significant if p < .05.
Abbreviations: COPD=Chronic Obstructive Pulmonary Disease, FEV1post BD= Force expiratory volume in 1 s (After using bronchodilator), FEV1post BD predicted %= Predicted % FEV1post BD with reference in Hong Kong 44 , mMRC= Modified Medical Research Council Dyspnea Scale, MVIC = maximum voluntary isometric contraction, NIV= Non-invasive ventilation.
Primary outcome
Outcomes of the study.

Data: Median (Interquartile range).
aTested by Likelihood Ratio Chi-Square Test.
bTested by Mann-Whitney U Test.
cTested by Related-samples Wilcoxon Signed Rank Test.
Statistically significant if p < .05.
Abbreviations: Δ, Change in parameter (Post-Pre), 6MWT= 6-m Walk test distance (Meter), CAT= COPD assessment test score, HGS= Handgrip strength (Newton), MVIC= Maximal voluntary isometric contraction (Newton), SPPB= Short Physical Performance Battery Score.
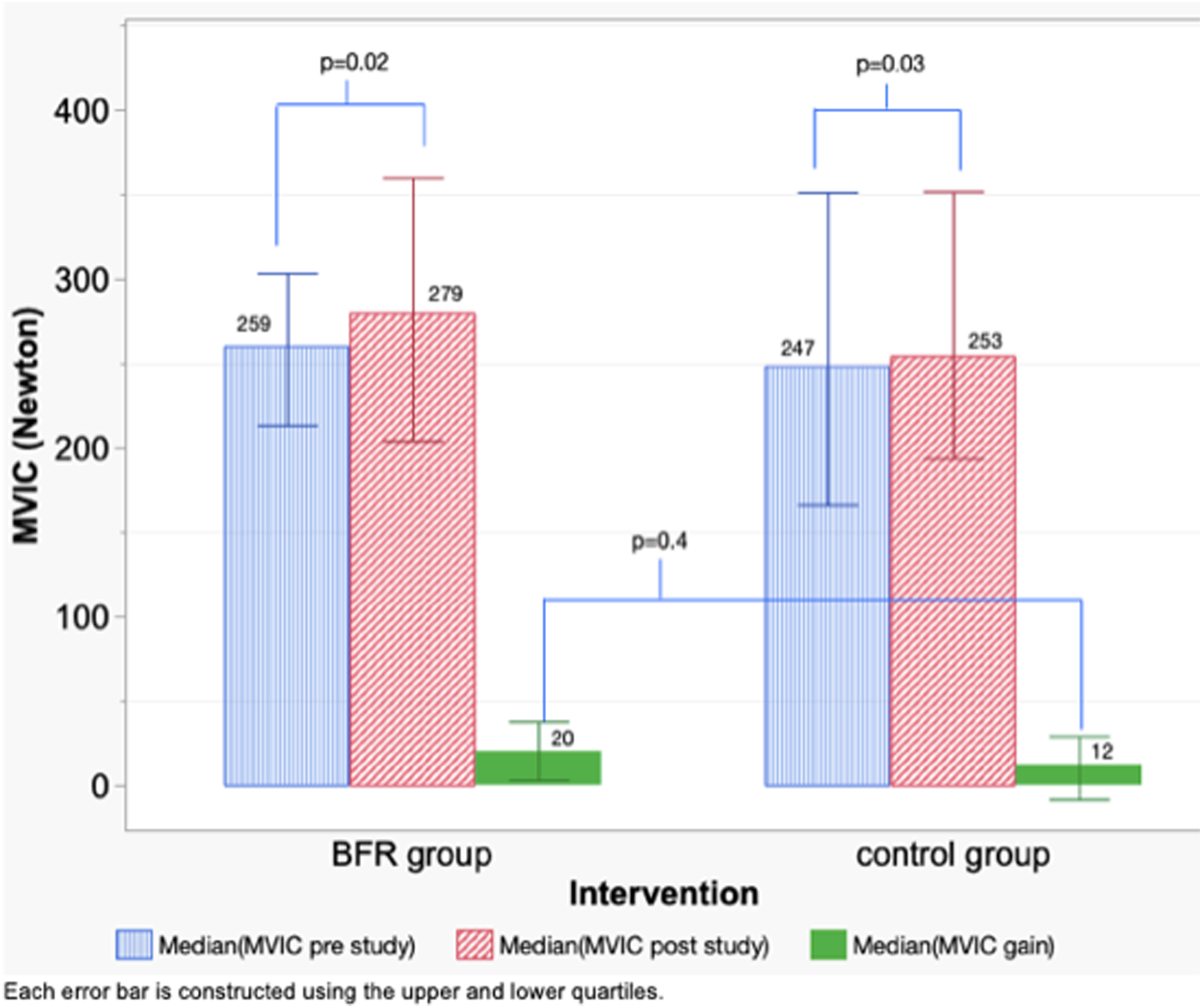
Change in maximum voluntary isometric contraction (MVIC) (Newton).
Secondary outcomes
Functional Performance
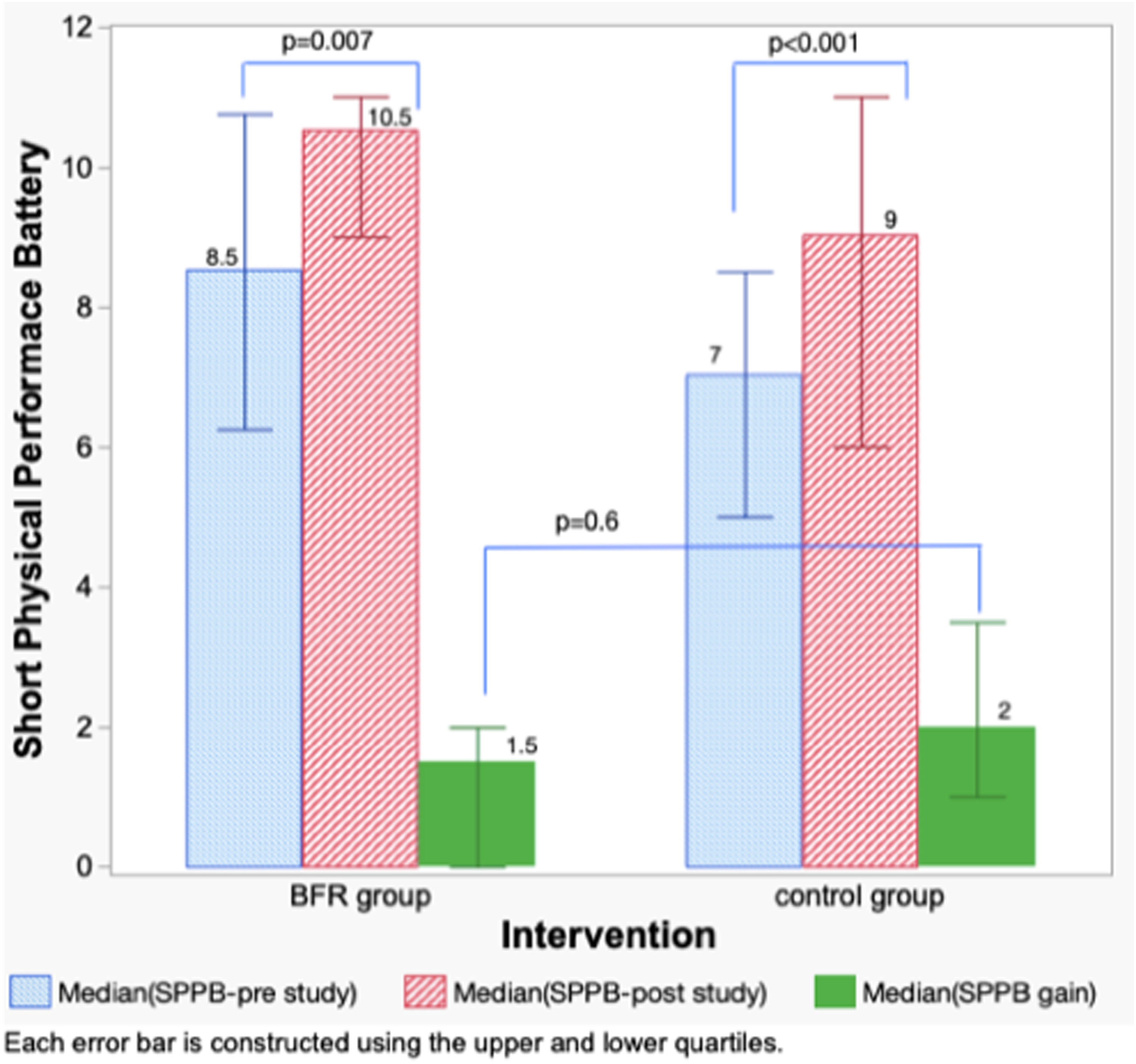
The median change of hand grip strength in BFR-RE group was 10N (IQR 0 to 20), comparing to that in control group was 20N (IQR 0 to 55) (Figure 3). The median change of 6-min walk test distance in BFR-RE group was 6 m (IQR -24.5 to 55.8), comparing to that in control group was 37 m (IQR 17.5 to 68.5) (Figure 4). The median change of Short Physical Performance Battery score in BFR-RE group was 1.5 (IQR 0 to 2), comparing to that in control group was 2 (IQR 1 to 3.5) (Figure 5). The median change of COPD Assessment Test (CAT) score in BFR-RE group was 7 (IQR 0.25 to 15), comparing to that in the control group was 6 (IQR 2 to 12.5) (Figure 6). All the between-group differences of changes in functional performances after training were statistically insignificant (p=.09; p=.05; p=.6; p=.5, respectively) (Table 3). Change in hand grip strength (Newton). Change in 6-min walk test distance (m). Change in Short Physical Performance Battery score. Change in COPD assessment test score.


Feasibility
Both groups had statistically insignificant difference (p=.6) in presence of Delayed Onset Muscle Soreness (DOMS), 5% (N=1 out of 20) in BFR-RE group, comparing 12% (N=3 out of 25) in control group. There was statistically significant increase of pain score 3.4 out of 10 marks (p=.001) immediate after training session with BFR-RE comparing with control group, but the average pain score dropped to zero in 5 minutes after training. No significant adverse events were reported during the training period.
Acceptability
There was 75% of subjects (15 out of 20 patients) in the BFR group showed "Like/Very like” when asked about the acceptance of whole program which was similar to the control group (60%, 15 out of 25 patients) (p=.5) (Figure 7). Acceptance of training (p = .5).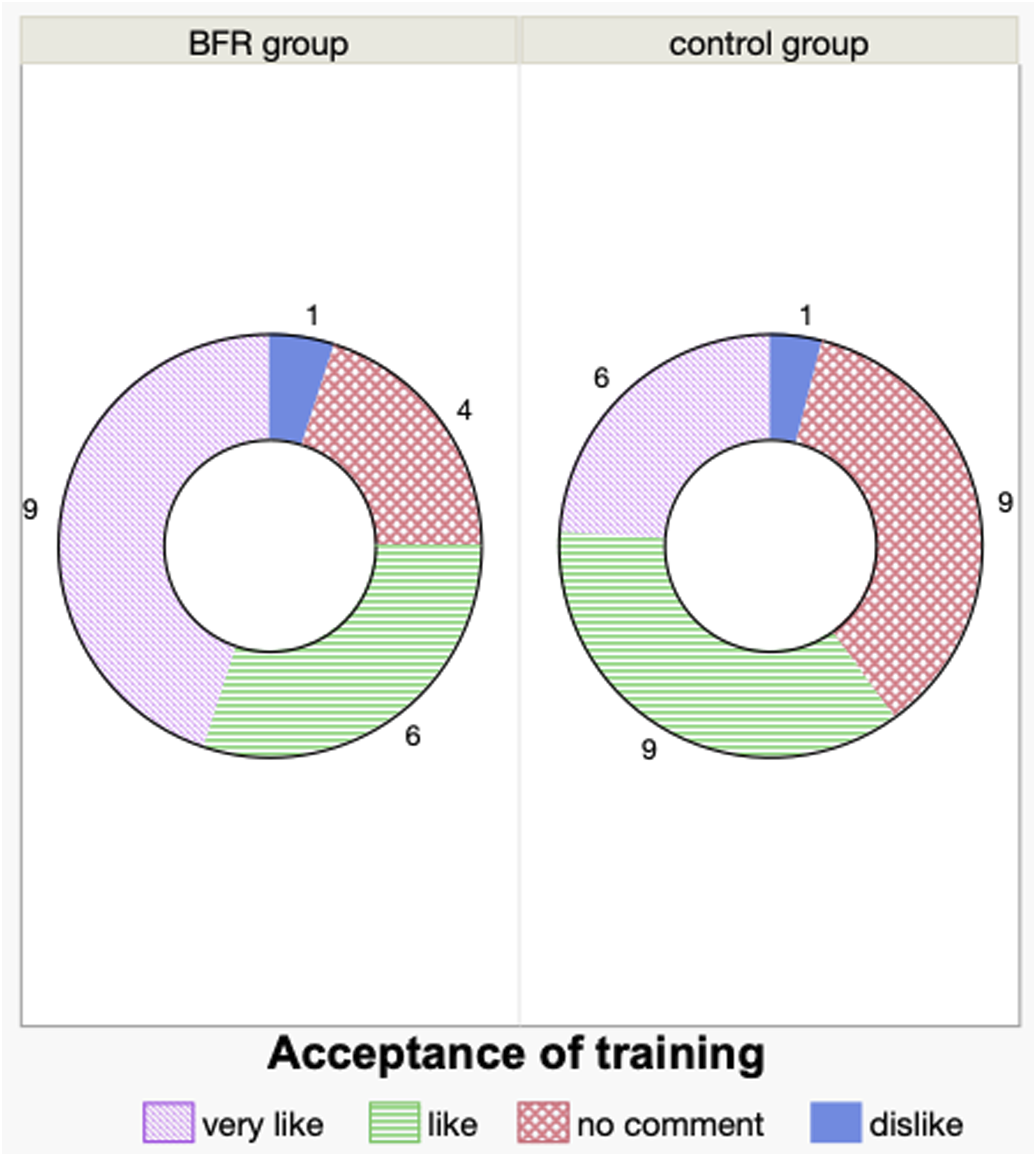
Drop-out of the study
Seven patients were drop-out in BFR-RE group, including 3 needed to have hospital infection contact precaution and 2 were hospitalized less than 2 weeks due to early discharge for personal reasons. The remaining 2 were defaulted training because of pain related to the occlusion pressure and bradycardia related to the underlying complete heart block with conservative treatment. One drop-out in the control group was due to hospitalization less than 2 weeks due to early discharge for personal reasons.
Other observational findings during study:
The occurrence of acute medical events during rehabilitation was statistically significantly different between both groups (p=.01). There were 8 out of 20 patients had acute exacerbation or hospital acquired infections in BFR-RE group, comparing to control group (4 out of 20). Three more medical events recorded in BFR-RE group, including fall with knee injury, insomnia and walking limited by low back pain.
There was no statistically difference (p=.7) between both groups in unplanned COPD-related readmissions within 1 month of discharge, 2 out of 20 patients in BFR-RE group, comparing to 1 in 25 in control group.
There was no statistically significant difference in biochemical changes within and between two groups. Concerning the creatinine kinase (CK) level in serum sample, in BFR-RE group, the median change was zero (pre-study: 64, IQR 34 to 108 units/L; post-study: 68, IQR 38 to 102 units/L), comparing to that in control group was 4, IQR -12 to 15 units/L (pre study: 46, IQR 34 to 68 units/L; post study: 52, IQR 40 to 63 units/L). There was no myoglobin in urine sample detected in pre or post study of both groups.
Discussion
This is the first randomized controlled study on BFR-RE in in-patient pulmonary rehabilitation program for patients with post COPDAE in the literature and demonstrated BFR is acceptable to be included in the resistance exercise training. Although statistically insignificant, it showed an 8N additional muscle strength gain in the BFR-RE group compared with the control group (same low-load resistance exercise without BFR). There was 8% muscle strength gain within the BFR-RE group after training comparing to 5.6% in control group (p= .3).
In a BFR-RE randomized control trial 37 conducted in healthy elderlies demonstrated around 19% muscle strength gain from baseline in BFR-RE group after a 3-days per week training for 4 weeks (12 sessions for each limbs), but failed to demonstrate a significantly different improvement between groups. The meta-analysis 11 of 11 studies, in which 9 studies were conducted in healthy subjects younger than 25 years of age, showed a significant improvement of muscle strength with a mean effect size of 0.58 (95% CI of 0.40 and 0.76) when comparing with sole low intensity training with effect size of -0.00 (95% CI of -0.18 and 0.17). Owning to the different type of subjects of study, the effect might not be transferable to elderly patients in post-COPDAE in current study.
The average calculated 1-RM of knee extension in our study was 5 kg. However, in a reported pulmonary rehabilitation program without using BFR for resistance training in outpatient COPD group showed a mean of 1-RM was 37 ± 13.6 kg. 38 An underestimation of 1-RM might contribute to inadequate training load leading to a less effective muscle strength improvement in the current study. This could be due to the intrinsic study defect when choosing the conversion formula31,39 to determine 1-RM from MVIC.
The short in-patient training phase might fail to detect clinically significant physiological change of BFR-RE. However, due to the COVID-19 pandemic, a further extension of out-patient training phase was not feasible which could be possible to detect the difference of muscle strength gain. Muscle strength gain by high intensity resistance training is proposed via different mechanisms, neurologically and morphologically. 40 Within the first 2 weeks of training, the rise of strength relies more on the neurological adaptation by learning and changes in intermuscular coordination of agonists, antagonists and synergists, increase in motor-unit recruitment or firing frequency, etc. In the following weeks, further gain of muscle strength attributes to the hypertrophy of individual fibers by myofibrillar growth and proliferation, increase in myonuclei to cytoplasm ratio by upregulation of transcription or translation, activation of satellite cells to proliferate and fuse with existing myofibers. This could not be detected in our study and no structural imaging applied to detect the muscle hypertrophy.
Failure to show a post training significant improvement of 6-min walk test distance in BFR-RE group could be explained by more subjects with acute medical events during rehabilitation (55% in the BFR-RE group), comparing only 16% in the control group. These acute medical events included COPD acute exacerbation, hospital acquired infections, accidental fall and insomnia.
Both BFR-RE group and control group achieved minimal clinical important difference (MCID) in SPPB, 21 with a median score of 1.5 (IQR 0 to 2) and 2 (IQR 1 to 3.5) respectively without significant between group difference. Balance and gait speed did not only rely on quadriceps strength, but also coordination, joint conditions, proprioception, vision etc. More training sessions and longer time for muscular morphological adaptation might be needed to show the additional benefit of the BFR-RE.
The median pain score rated immediately after BFR-RE training was 3.4 (IQR 1.3 to 5.4) out of 10 points and dropped to zero in 5 min after training indicating the patients could adapt and tolerate the pain induced by BFR. There was only 1 subject out of 27 in BFR-RE group could not tolerate the training due to occlusion discomfort. The drop-out rate due to BFR-related discomfort was 3.7%. The presence of DOMS was similar between the BFR-RE group (5%, n=1) and control (12%, n=3) (p=.6). The low level of DOMS when using 15%–30% of 1-RM makes BFR-RE more feasible to introduce into COPD cohorts.
The other drop-out patient in BFR-RE group was due to the undetectable occlusion pressure by the blood flow restriction device. That patient had asymptomatic bradycardia due to known high grade heart block though he opted not for pacemaker. The BFR device does not mention any lowest limit of heart rate to preclude of the training, otherwise, this case should be excluded from the study before recruitment.
There was no other significant adverse effect reported in the study and no statistically significant difference within and between groups in the biochemical aspects suggesting of risks of muscle injury or rhabdomyolysis. This was consistent with the literature that BFR-RE was a safe procedure. 41
Limitations of the study
Most of the subjects in the study was male leading difficult to translate the effect on muscle strength gain after BFR-RE to female patients for post COPDAE rehabilitation. Calculation of 1-RM by the equation might underestimate the training load. The post training evaluation might be too early after the last session of training (next day of last training or even in the afternoon after the last morning training session). The short training duration (2 weeks) unlikely reached the plateau of the improvement of muscle strength which could be demonstrated in average of 12-week progressive resistance training protocols. 42 The outcome measurement during post-COPDAE was difficult since different acute medical events could occur affecting the training and assessments.
Suggestions for future study
The duration of training could be continued and extended to 10 to 12 weeks in outpatient pulmonary rehabilitation center after discharge. This might get a higher effect of training improvement as Loenneke showed. 11
Current study excluded all patients required assistance in walking solely since no appropriate functional tests for them. However, these frail hospitalized patients might be possible to tolerate and benefit more from low-load BFR-RE since they are mostly load compromised for training.
Conclusion
Feasibility and high acceptance of BFR-RE in patients with post-COPDAE were demonstrated in current study. Low-load resistance training with or without BFR in a 2-week inpatient pulmonary rehabilitation both improved muscle strength of knee extensors, but BFR-RE group did not show statistically significantly additional muscle strength gain, comparing to control group (resistance exercise without BFR). Further studies could be considered in an outpatient setting with a longer training duration and progression of resistance load according to the increase of muscle strength throughout the training period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.