
Abstract
Background
Functional status is a marker for evaluating fall risk and predicting mortality and hospitalisations in elderly and patients with COPD. Acute exacerbations of COPD result in sudden declines in exercise capacity, quadriceps force (QF) and physical activity (PA), but their impact on functional status remains unclear. This study aimed to (i) compare the functional status of patients with COPD to healthy controls and (ii) assess prospectively the impact of an exacerbation on functional status.
Methods
Healthy controls and patients were assessed. Patients were followed up every 6 months and were tested again immediately if they reported an exacerbation. The short physical performance battery (SPPB), timed up and go test (TUG), 1-minute sit-to-stand test (1MSTS), 6-minute walking distance (6MWD), QF and PA (accelerometery) were measured.
Results
Thirty-six patients (69 ± 7 years, 69% male) and 25 matched healthy controls (68 ± 7 years, 80% male) were included. Functional status was decreased in patients compared to healthy controls. Twelve patients were retested 10 ± 7 days after a moderate (n = 11) or severe (n = 1) exacerbation. The 1MSTS (∆-3 ± 3repetitions, p < 0.0001), 6MWD (∆-34 ± 46m, p < 0.0001) and QF (∆-9 ± 13Nm, p = 0.05) decreased after exacerbation onset. No changes in SPPB and PA were observed.
Conclusion
An exacerbation negatively impacts the already reduced functional status in patients with COPD. The SPPB is not able to capture this decline.
Keywords
Introduction
Patients with Chronic Obstructive Pulmonary Disease (COPD) experience both pulmonary and extra-pulmonary symptoms, such as fatigue, skeletal muscle dysfunction, and reduced exercise capacity,1,2 hindering daily activities like walking, stair climbing, and sitting and standing from a chair. 3 Assessing functional status, defined as the ability to complete activities necessary for fulfilling basic physical, psychological, and social needs, 4 can provide valuable insights into these challenges.
Functional status can be evaluated through various tests, which often overlap but emphasise different impairments. For instance, the short physical performance battery (SPPB) and timed up and go test (TUG) evaluate functional mobility and balance.5,6 The 5-times sit-to-stand test (5STS) addresses predominantly postural control and lower limb strength, 7 while the 1-minute sit-to-stand test (1MSTS) assesses functional exercise capacity. 8 Recently, instrumented assessment using wearable sensors became available, allowing more granular assessment of the different phases of these functional tests (e.g., walking, turning, standing up and sitting down) and providing insights into the underlying mechanisms of impairments. The detailed information also allows to explore whether the performance of patients changes throughout the test.
Compared to healthy individuals, patients with COPD exhibit reduced functional mobility and balance, with reduced gait speed (weighted mean: +0.21 m/s during 4-meter gait speed (4MGS)) 9 and longer times to complete the 5STS (+3.30-6 s)10,11 and the TUG (weighted mean: +2.61 s). 12 Furthermore, patients showed decreased functional exercise capacity (-4-8 repetitions during 1MSTS).13–15 Whereas these impairments in COPD are known, detailed information about which component of a specific test is more affected is limited.
Functional tests have demonstrated a strong ability to predict falls, mortality and acute exacerbations of COPD (AECOPD).16–19 AECOPDs are associated with adverse clinical outcomes, including declines in lung function, quality of life, muscle function, and exercise capacity.20–23 However, its acute impact on functional status and physical activity (PA) remains unclear. 21 One study reported functional impairment during an AECOPD as measured by the 4MGS and 6-minute walking test (6MWT), but did not observe a reduction in PA. 24 This study compared hospitalised patients during an AECOPD with stable patients with COPD, and did not longitudinally assess the impact of an AECOPD. Research investigating the impact of a moderate AECOPD is currently limited. 25 Additionally, the impact of an AECOPD on the different components of functional tests remains unexplored. Given its negative impact on muscle function, it is hypothesised that the sit-to-stand transition of a sit-to-stand test will be more affected than the stand-to-sit transition, as the latter primarily requires postural control. 10
This study aimed to (i) cross-sectionally compare functional status (including a spectrum of functional tests: SPPB, TUG, 1MSTS, 6MWT), quadriceps force and PA between patients with COPD and healthy controls; (ii) prospectively investigate the acute impact of an AECOPD on these outcomes; and (iii) explore the components of functional tests (SPPB, TUG and 1MSTS) using wearable sensors. We hypothesised that functional status is reduced in patients with COPD compared to healthy controls and further declines during an AECOPD.
Methods
Study design
This prospective cohort study was nested in a randomised controlled trial investigating the effectiveness of a long-term PA coaching intervention in patients with COPD (NCT04139200). Details of the intervention are published elsewhere 26 and available in the supplement. Patients were recruited at Ghent University Hospital (Ghent, Belgium) between September 2021 and April 2023.
Functional status was assessed at baseline and every 6 months until the first occurrence of an AECOPD (the maximum follow-up period was 2 years). Patients used a smartphone application which prompted a weekly question (“Did you change your medication in the past week?”) to detect changes in medication as an indicator of an AECOPD. 27 When a change in medication was reported, the investigators were alerted and patients were contacted to discuss the change in medication. If an AECOPD was detected (i.e., the patient reports an increase in symptoms together with an intake of antibiotics and/or corticosteroids; with or without a hospital admission), the patient was invited for a reassessment as soon as possible.
Study population
Patients above 40 years with a smoking history of ≥10 pack years, a clinical diagnosis of COPD (confirmed by spirometry (FEV1/FVC <0.70)) and no AECOPD within 4 weeks prior to inclusion were eligible to participate. Patients involved in a multidisciplinary rehabilitation program, on the waiting list for lung transplantation, unable to use a smartphone or unable to improve PA due to musculoskeletal comorbidities were excluded.
For comparison, healthy controls were recruited between November 2022 and August 2023 for a single clinical visit. Control subjects were 50-80 years old, had an FEV1/FVC ≥0.70, never smoked or quit smoking more than 20 years prior to inclusion, did not participate in a structured exercise program and displayed no orthopaedic or other comorbidities preventing from being physically active.
Both studies were approved by the ethical committee of Ghent University Hospital (BC-10267 (COPD) and ONZ-2022-0387 (healthy controls)) and participants signed informed consent prior to data collection.
Participant characteristics
Sociodemographic data (age, sex, height, weight), smoking history, pharmacological treatment and spirometry according to ATS/ERS guidelines were collected in both groups.
Functional status
The SPPB, TUG and 1MSTS were conducted in a standardised order while wearing the Dynaport MoveTest (McRoberts, The Hague, The Netherlands), containing a tri-axial accelerometer, gyroscope and magnetometer. 28 This device provides granular data on these tests and its phases.
The SPPB consists of three sub-tests: Standing balance test, 4MGS and, 5STS. Each subtest was scored 0 to 4, with a maximum score of 12 indicating better performance. 5 For the 5STS, the average duration of the sit-to-stand-to-sit cycle, sit-to-stand and stand-to-sit transition, stand and sit phase of the 5 cycles were retrieved. The duration of each phase was also expressed as a percentage of the total time needed to complete a sit-to-stand-to-sit cycle.
For the TUG, participants stand up from a chair, walk 3 meter at their habitual speed, turn, walk back to the chair and sit down again, 6 collecting the total duration as outcome. Total duration of the sit-to-stand and stand-to-sit transition as well as average duration of the walk and turn phase were retrieved. Additionally, the duration of both transitions was expressed as a percentage of the total sit-to-stand-to-sit cycle.
In the 1MSTS, participants performed as many sit-to-stand cycles as possible within 1 minute with arms across the chest, 8 recording the number of completed cycles. In addition, average duration of the sit-to-stand-to-sit cycle, sit-to-stand and stand-to-sit transition, stand and sit phase of all cycles were retrieved. The duration of each phase was also expressed as a percentage of the total time needed to complete a sit-to-stand-to-sit cycle.
Functional exercise capacity was measured as the best of two 6MWT in a 55 meter quiet corridor, according to ATS/ERS guidelines, and expressed in meters.
Quadriceps force
Isometric quadriceps force of the right leg was measured in a seated position with 90° knee flexion via a fixed strain gauge dynamometer (Sauter Controls NV, Zellik, Belgium). The best out of three attempts was recorded.
Physical activity
PA was objectively measured for seven consecutive days using the Dynaport MoveMonitor (McRoberts, The Hague, The Netherlands). Participants were instructed to wear this validated tri-axial accelerometer during waking hours, 29 with a valid measurement requiring at least 8 h of wear time on a minimum of two weekdays. 30 Average daily step count and movement intensity during walking were retrieved for analyses.
Symptom experience
In patients, symptoms were assessed using the modified Medical Research Council (mMRC) scale for dyspnoea, the COPD Assessment Test (CAT) for health status (score ≥18 indicating high symptom burden 31 ), the Chronic Respiratory Disease Questionnaire (CRDQ-SAS) dyspnoea domain, and the fatigue subscale of the Checklist Individual Strength (CIS) (score ≥36 indicating severe fatigue 32 ).
Statistics
Statistical analyses were performed using SAS V9.4 (SAS Institute, Cary, North Carolina, USA). Data are presented as mean ± SD, median (Q1-Q3), or proportions after testing for normality using the Shapiro-Wilk test. Statistical significance was set at p < 0.05.
Unpaired t-tests or Mann-Whitney U tests were conducted to compare the functional status between patients and healthy controls. To investigate the impact of an AECOPD on functional status, paired t-tests or Wilcoxon Signed-Rank tests were performed to compare the last stable measurement preceding the AECOPD with the data after the AECOPD. As a reference, the yearly change in functional status (data at 1 year follow-up minus data at baseline) was assessed in patients who did not experience an AECOPD during follow-up (n = 22). PA analyses were adjusted for duration of daylight. 33
Finally, we explored whether patients changed their performance throughout the test. To do this, we analysed the duration of each sit-to-stand-to-sit cycle throughout the 1MSTS using data of the Dynaport MoveTest. The time of the sit-to-stand-to-sit cycle was the dependent variable and the number of the repetition was the independent variable (fixed effect) in a mixed model for repeated measures analyses with patient ID as a random effect. This analysis was repeated for patients and healthy controls separately.
Results
Participant characteristics
Characteristics of participants included in the analyses, expressed as mean ± SD, median (Q1-Q3) or proportion.
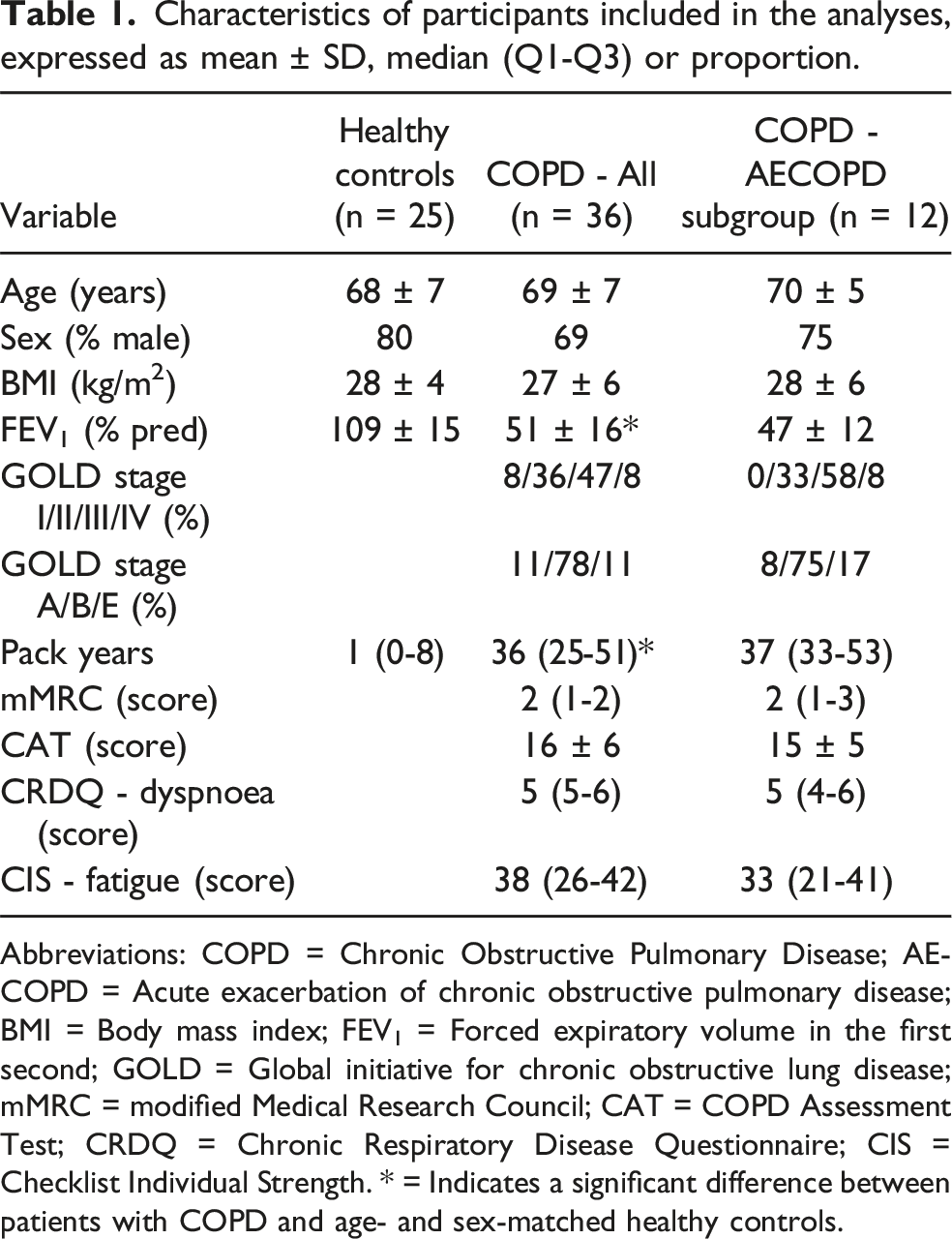
Abbreviations: COPD = Chronic Obstructive Pulmonary Disease; AECOPD = Acute exacerbation of chronic obstructive pulmonary disease; BMI = Body mass index; FEV1 = Forced expiratory volume in the first second; GOLD = Global initiative for chronic obstructive lung disease; mMRC = modified Medical Research Council; CAT = COPD Assessment Test; CRDQ = Chronic Respiratory Disease Questionnaire; CIS = Checklist Individual Strength. * = Indicates a significant difference between patients with COPD and age- and sex-matched healthy controls.
Patients with COPD versus healthy controls
Patients showed impairments across all parameters of functional status (Figure 1). Compared to controls, patients had lower quadriceps force (mean ± SD 119 ± 42 Nm vs. 170 ± 37 Nm, p < 0.0001), daily step count (5164 ± 2952 steps/day vs. 7832 ± 2879 steps/day, p = 0.001) and movement intensity during walking (1.67 ± 0.27 m/s2 vs. 2.04 ± 0.35 m/s2, p < 0.0001). Functional status in healthy controls (grey) versus patients with COPD (black). Functional tests: (A) Short physical performance battery (SPPB), (B) Timed up and go test (TUG), (C) 1-minute sit-to-stand (1MSTS) and (D) Six-minute walking distance (6MWD). Data are expressed as individual datapoints or mean ± SD. Differences between both groups are investigated by unpaired t-test (parametric data) or Mann- Whitney U test (non-parametric data). Abbreviations: HC = Healthy controls; COPD = Chronic Obstructive Pulmonary Disease.
The total SPPB score was lower in patients (median (Q1-Q3) 11 (10-12) vs. 12 (12-12), p < 0.001), primarily attributed to deficits in 5STS (3 (3-4) vs. 4 (4-4), p = 0.001) and balance (4 (4-4) vs. 4 (4-4), p = 0.05). While the SPPB point score for 4MGS showed no differences (4 (4-4) vs. 4 (4-4), p = 0.24), patients had worse absolute values for 4MGS (1.56 ± 0.18 m/s vs. 1.42 ± 0.29 m/s, p < 0.001) and 5STS (11.59 ± 2.59 s vs. 9.20 ± 1.78 s, p < 0.001).
Objectively measured data of timed up and go test, 1-minute sit-to-stand test and 5-times sit-to-stand test in healthy controls versus patients with COPD, expressed as mean ± SD.

Differences between both groups are investigated via unpaired t-test. Abbreviations: COPD = Chronic obstructive pulmonary disease; s = Seconds.
No statistically significant differences were found between both groups when the duration of individuals phases were expressed relative to the total time of the sit-to-stand-to-sit cycle (Table S1). Furthermore, the time to complete the sit-to-stand-to-sit cycles remained stable throughout the 1MSTS in both groups (time effect: p = 0.53 (COPD) and p = 0.66 (controls)).
Impact of an AECOPD
12 patients were tested 10 ± 7 days after change in medication (n = 11) or hospital discharge (n = 1) and there were 111 ± 48 days between their last stable measurement preceding the AECOPD and testing after an AECOPD. Compared to their preceding stable measurement, 1MSTS and 6MWD decreased significantly (Figure 2). Both tests declined numerically more than the 1-year decline observed in the stable cohort (∆-1 ± 3 repetitions (1MSTS) and ∆-15 ± 66m (6MWD)). Quadriceps force tended to decline (∆-9 ± 13 Nm, p = 0.05), the 1-year decline in the stable cohort was ∆-13 ± 33 Nm. No changes were observed in SPPB (nor sub-tests: ∆0.00 ± 0.14 m/s, p = 0.99 (4MGS) and ∆0.41 ± 1.67 s, p = 0.43 (5xSTS)) and TUG (Figure 2). After excluding one outlier, TUG increased with Δ0.72 ± 0.84 s, (p = 0.03). The AECOPD did not significantly impact movement intensity (mean ± SEM ∆0.03 ± 0.07 m/s2, p = 0.66) and daily step count (mean ± SEM ∆-946 ± 708 steps/day, p = 0.21). However, the reduction of the latter was numerically greater than the 1-year change observed in the stable cohort (mean ± SEM ∆51 ± 500 steps/day). Functional status in patients with COPD at the last measurement preceding the AECOPD and as soon as possible after experiencing an acute exacerbation of COPD. Functional tests: (A) Short physical performance battery (SPPB), (B) Timed up and go test (TUG), (C) 1-min sit-to-stand (1MSTS) and (D) Six-minute walking distance (6MWD). Data is expressed as individual datapoints. One patient experienced an AECOPD requiring hospitalisation (dotted line). Differences between both groups are investigated by paired t-test (parametric data) or Wilcoxon Signed-Rank test (non-parametric data). After excluding one outlier, TUG increased significantly (p = 0.03). Abbreviations: AECOPD = Acute exacerbation of chronic obstructive pulmonary disease.
The Dynaport MoveTest showed that the average duration of the stand-to-sit transition and walk phase during TUG increased following an AECOPD (n = 7; Table S2). Similarly, patients needed more time to perform sit-to-stand-to-sit cycles after an AECOPD, primarily driven by an increase in the stand-to-sit transition (p = 0.044 (1MSTS) and p = 0.018 (5STS)). In the 1MSTS, the time of the sit-to-stand transition also tended to be longer after an AECOPD (17% slower, p = 0.065; Table S2). No significant changes were observed in sitting time (31% slower) during 1MSTS. The 1MSTS appeared to be more sensitive to the impact of an AECOPD compared to the 5STS (Table S2).
Health status and symptoms of dyspnoea and fatigue worsened after experiencing an AECOPD (Figure 3). Eighty three percent of the patients became highly symptomatic (CAT score ≥18 points) and 55% experienced extreme fatigue (CIS score ≥36 points) compared to 33% and 36%, respectively, before the AECOPD (p = 0.01 and p = 0.16). Changes in questionnaires in patients with COPD at the last measurement preceding the AECOPD and as soon as possible after experiencing an acute exacerbation of COPD. (A) modified Medical Research Council (mMRC) questioning dyspnoea, (B) COPD Assessment Test (CAT) questioning health status, (C) Chronic Respiratory Disease Questionnaire (CRDQ-Dyspnoea) questioning symptoms of dyspnoea and (D) Checklist Individual Strength (CIS) - fatigue subscale. Data is expressed as individual datapoints. One patient experienced an AECOPD requiring hospitalisation (dotted line). Cut-off scores of CAT and CIS questionnaires are displayed on the graphs. Differences between both groups are investigated by paired t-test (parametric data) or Wilcoxon Signed-Rank test (non-parametric data). Abbreviations: AECOPD = Acute exacerbation of chronic obstructive pulmonary disease.
Discussion
This study confirms impaired functional status in stable patients with COPD compared to healthy subjects. It is the first to show that all phases of functional tests are affected, as patients required more time to complete all phases of the TUG and sit-to-stand tests. Experiencing an AECOPD leads to acute worsening of most functional tests and symptoms of dyspnoea and fatigue. The SPPB and PA were not affected by the AECOPD, or these measures were less sensitive to detect changes in this small sample.
Our findings align with previous studies showing worse functional status in patients with COPD compared to healthy subjects, as measured by the SPPB, TUG, 1MSTS and 6MWT.2,12,13,34 New is that objectively collected data showed that patients required more time to complete each phase of the TUG, which is usually attributed to reduced muscle strength (standing up), balance (turning and sitting down) and gait speed (walking phase). Our data supports this, as patients exhibit reduced muscle strength and gait speed compared to healthy controls, and required 40% more time to complete turns.
The sit-to-stand-to-sit manoeuvre is a highly relevant and muscle power demanding functional task. We found that most phases of 5STS and 1MSTS are prolonged in patients compared to healthy controls. Patients also remained nearly twice as long seated than controls between transitions, whereas the stand phase was not significantly different. Janssens et al. 10 reported a longer stand and stand-to-sit phase during 5STS in patients with COPD compared to healthy subjects. The discrepancy with our results might be attributed to the inclusion of patients with lower quadriceps strength (75%pred vs. 82%pred) in this study, as sufficient quadriceps strength is essential for the sit-to-stand transition. 35 Of note, this transition is the most sensitive phase for predicting fall risk. 36 Interestingly, and against our hypothesis, both patients and controls kept a constant time to complete the sit-to-stand-to-sit cycles throughout the 1MSTS. However, this should be confirmed in larger samples.
To the best of our knowledge, this is one of the first studies using a prospective design to examine the impact of an AECOPD on a suite of tests assessing functional status in patients with COPD. Previous longitudinal studies showed that functional exercise capacity, quadriceps force and PA declined during and after an AECOPD22,23,25,37 which aligns with most of our data. In our cohort, PA did not change significantly, which can mainly be attributed to the small sample size. The decline after an AECOPD (−946 ± 708 steps/day) exceeded the 1-year change in stable patients (51 ± 500 steps/day). Second, the timing of the assessment might also explain this discrepancy. Alahmari et al. 23 reported that PA recovered to continued low levels within a median of 3.5 days after a moderate AECOPD, whereas our patients were assessed after an average of 10 days following a change in medication or hospital discharge. This could already have induced a (partial) recovery of PA. Last, the majority of patients experienced a moderate AECOPD. The present study justifies properly powered studies to investigate prospectively the impact of moderate and severe AECOPDs on PA.
Some measures, such as the SPPB (including subtests), seem less sensitive to pick up the changes in functional status after AECOPDs. In contrast, the 1MSTS and 6MWT, which require muscle endurance and resistance to fatigue as well as ventilatory capacity and may therefore be more suitable. 13 Objectively measured data showed that the average duration of the stand-to-sit and sit-to-stand transition during the 1MSTS are prolonged after an AECOPD, which may be explained by the reduction in quadriceps function and increased quadriceps fatigue after an AECOPD. Furthermore, our findings emphasize the importance of assessing fall risk, as the sit-to-stand transition - identified as the most sensitive phase for predicting fall risk - is adversely affected by an AECOPD. 36
Health status and symptoms of fatigue and dyspnoea worsened after an AECOPD, which aligns with the findings of Zimmerman et al., 38 who showed a significant increase in the CAT score at the onset of an AECOPD to 7 days after onset. Our findings are also consistent with previous research, showing increased symptoms of fatigue, measured by FACIT-F, during an AECOPD without hospitalisation. 25
Strengths and limitations
This study is one of the first providing an insight in the functional status of patients with COPD using a suite of tests. We provided in depth information about different phases of functional tests compared to a healthy control group. Furthermore, this study also provides insight into the impact of experiencing an AECOPD (with or without hospitalisation) on functional status using a longitudinal design.
Nevertheless, our study has some limitations that should be considered. First, technical issues with the wearable sensor led to missing data for some patients and healthy controls, resulting in a low sample size. Second, the small number of patients experiencing an AECOPD challenges the ability to draw robust conclusions. Third, only one patient experienced an AECOPD requiring hospital admission making extrapolation to all AECOPDs difficult. Analyses are mainly based on the impact of AECOPDs not requiring hospital admission and may provide an underestimation of the impact of AECOPDs requiring hospital admission. We used a quick, non-obtrusive method of collecting AECOPDs. Whereas we cannot rule out that AECOPDs were missed using this methodology as compared to for example daily reporting of symptoms, compliance with answering the weekly question on medication change was high and the methodology showed to be a crucial complement to regular forms of detection of AECOPDs. 27 Moreover, if AECOPDs would have been missed, this would not have affected the results on the impact of an AECOPD. Last, selection bias among healthy controls cannot be excluded, as motivated individuals are more prone to participate. However, they performed as expected for 6MWD and quadriceps force and did accumulate relatively modest step counts compared to previous healthy cohorts recruited in Belgium. 39 Their 1MSTS performance was slightly below predictions by Strassmann et. 40 Hence we believe possible bias is unlikely.
Conclusion
Patients with COPD have a reduced functional status across all tests used, compared to healthy controls. Sit-to-stand as well as stand-to-sit transitions appear slower in patients with COPD. Importantly, the occurrence of an acute exacerbation of COPD leads to further worsening of the already reduced functional status in some, but not all functional tests. The 1-minute sit-to-stand test and 6-minute walking test appeared as the most sensitive tests to pick up the impact of an exacerbation on functional status.
Supplemental Material
Supplemental Material - Functional status in COPD: Comparison with healthy controls and impact of an exacerbation
Supplemental Material for Functional status in COPD: Comparison with healthy controls and impact of an exacerbation by Fien Hermans, Eva Arents1, Astrid Blondeel, Nina Cardinaels, Wim Janssens, Thierry Troosters, Eric Derom, and Heleen Demeyer in Chronic Respiratory Disease.
Footnotes
Acknowledgements
The authors would like to thank the colleagues from the pulmonary function testing at Ghent University Hospital for their assistance with the clinical assessments. Additionally, we would like to thank all the participants of the study.
Ethical considerations
Both studies were approved by the ethical committee of Ghent University Hospital (BC-10267 (COPD) and ONZ-2022-0387 (healthy controls)).
Consent to participate
All participants signed informed consent prior to data collection.
Consent for publication
All participants provided informed consent for publication.
Author’s contributions
HD and FH conceived and designed the study. Patient recruitment and data collection was performed by FH and EA. Data analyses and interpretation were performed by FH and HD. FH wrote the first draft of the paper. All authors critically reviewed the manuscript and provided feedback. All authors read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Flemish Research Foundation (grant G0C0720N). AB is a pre-doctoral research fellow of the Flemish Research Foundation (FWO-Flanders, 1194320N). WJ is a senior clinical research fellow of the Flemish Research Foundation (FWO-Flanders). HD is a post-doctoral research fellow of the Flemish Research Foundation (FWO-Flanders, 12H7517N).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be made available upon request.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.