
Abstract
To study the impact of self-administration of nonprescription medicines (NPMs) on patients with chronic obstructive pulmonary disease (COPD), in Chongqing Municipality, China. A total of 85 patients who had used NPM were assigned to the NPM group. Another 83 patients who had only used prescription medicines (PMs) were assigned to the PM group. Their income, educational levels, health status, public health insurance coverage, the expense of drugs during exacerbation, and the numbers of acute exacerbations during the past year were surveyed, and the approved drugs for COPD were evaluated. The contents of corticosterone in various types of NPMs were determined by high-performance liquid chromatography. The proportion of use of NPM in hospitalized patients with COPD was 12.96%. The percentage of illiteracy and low income was significantly higher in COPD patients in the NPM group than those in the PM group. The cost of drugs per day and the quality of life in the NPM group were lower than those in the PM group. Further analysis revealed that 15 of 21 NPMs contained corticosteroids. More importantly, medical advice from doctors and nurses appeared to be effective. Some Chinese patients with COPD living in the Chongqing area of China used NPMs that contained corticosteroids. Health education and advisement can effectively limit the use of NPMs.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by airflow limitation and can progress into dyspnea. Pathophysiologically, COPD involves many components, including airspace epithelial injury, inflammation, mucus hypersecretion, and oxidative stress in the airway and lungs. 1 Importantly, COPD is a leading cause of chronic morbidity and mortality, and its prevalence is increasing worldwide. 2
The overall prevalence of COPD in China was 8.2% (men, 12.4%; women, 5.1%) in individuals aged 40 years or above, 3 and the prevalence of COPD in individuals aged 40 years or above of the Chongqing municipal area was as high as 13.7%, representing the highest level in China. 3 Smoking and solid fuel–related air pollution have been associated with the development of COPD; and in China, the control of this disease still remains a challenge. 4 ,5 Currently, the standard therapy for COPD in China is consistent with the Global Initiative for Chronic Obstructive Lung Disease (GOLD). 6 ,7 However, the standard therapies, such as application of bronchodilators and theophylline, do not always appear to effectively alleviate patients’ symptoms during acute exacerbations at home. In addition, many patients have little or no insurance coverage and may be unable to afford the costs of these therapies. Accordingly, they usually seek cheaper and nonprescription medicines (NPMs) that have not been approved by the Chinese State Food and Drug Administration, from online pharmacies and other resources. These NPMs may include fake or substandard drugs, folk prescription, and off-label drugs. Similarly, it has been noticed that more than half of the drugs sold online are fake or of substandard quality, in Europe 8 ; and the prescription-only analgesics are readily available from various Web sites, often without a valid prescription in the United Kingdom. 9 Actually, China’s economic reform and the piecemeal nature of health care insurance have created a huge pharmaceutical market in which the lack of authoritative drug formulary, ineffective drug production/sell supervision, and distortion of the price schedule affect the control of COPD in China. 10 However, what percentage of COPD patients use NPMs and how the use of NPMs affects the disease progression has not yet been explored.
This study is aimed at investigating the use of NPM in COPD patients in the Chongqing Municipality, China, and how the use of NPM could affect the disease progression in Chinese COPD patients.
Methods
Study population and design
A total of 656 patients with acute exacerbation of COPD (AECOPD) admitted to 3 hospitals in Chongqing, China, from October 2009 to December 2009, were consecutively recruited in the study. Patients with COPD at stage I or higher were diagnosed, according to the criteria of the GOLD 6 , and the standard of the ratio of post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <70%. 1 Patients with a history of allergic rhinitis, asthma, and other chronic and acute diseases, or a recent history of myocardial infarction, heart failure, and arrhythmia were excluded.
Patients were surveyed by a questionnaire for their demographic characteristics, including family income, education, insurance coverage, the exacerbated use of and spending on drugs, the number of exacerbations during the recent year, and the subjective evaluation of the approved drugs for COPD. In addition, they were also surveyed for their health status using the disease-specific St George’s Respiratory Questionnaire (SGRQ), including three components (symptoms, activity, and impact) and the total SGRQ score. 11 Their blood pressure and blood glucose levels were measured. The 85 patients who had used NPMs were assigned to the NPM group. The other 82 patients who had only used prescription medicines (PMs) were assigned into the PM group. Written informed consent was obtained from the patients, and the experimental protocol was approved by the Ethic Committees of the hospitals.
Measurements of corticosterone levels
A total of 21 NPMs were collected from patients and the contents of corticosterone in the NPMs were determined by high-performance liquid chromatography (HPLC) (LC-10A, Shimadzu, Kyoto, Japan), using prednisone acetate or dexamethasone acetate (National Institute for the Control of Pharmaceutical and Biological Products, NICPBP, Beijing, China) as control samples. 12 Briefly, each NPM (1 g) such as prednisone acetate or dexamethasone acetate was dissolved in methanol to prepare the sample or standard solution (0.5 mg/ml). Each sample (20 μl) was subjected to reverse phase chromatography at 240 nm using the acetonitrile–water mixture (33:67) as the mobile phase and octadecylsilyl as the stationary phase. The concentrations of prednisone in each sample were calculated by linear regression analysis, according to the standards. The range of sensitive detection was between 5 and 50 ng/ml, with the correlation coefficient of 0.998.
Medical advice and follow-up
All the patients in the NPM group were advised regarding the correct therapeutic strategies of COPD, including diet, proper medical drugs, oxygen therapy, and rehabilitation therapy. In addition, they were informed about the potentially harmful effects of NPM on their health. After these medical interventions, the attitudes toward NPM were collected on the day before discharge. All the enrolled patients were surveyed by phone regarding the use of NPM every month for half a year after discharge.
Statistics
Data are expressed as mean ± SD of each measure for each group. The difference in each measure between these two groups was analyzed by χ 2 test and Student’s t test using a software package (SPSS, version 11.0, Chicago, USA). A p value of <0.05 was considered statistically significant.
Results
To determine the use of NPM in Chinese COPD patients and its effect on the disease progression, a total of 168 AECOPD patients were recruited, and their demographic and clinical characteristics are given in Table 1. There was no significant difference in the distribution of age, gender, and disease stages between these two groups of patients. However, the percentage illiteracy and low income in the patients in the NPM group was significantly higher than those in the PM group. Furthermore, the public health care insurance coverage in the NPM group was conspicuously lower than that in the PM group. Interestingly, the percentage of patients with hyperglycemia or hypertension in the NPM group was significantly higher than those in the PM group. Apparently, more patients with hyperglycemia and hypertension in the NPM group were living at lower family incomes and with less health care insurance coverage.
Characteristics of the patients
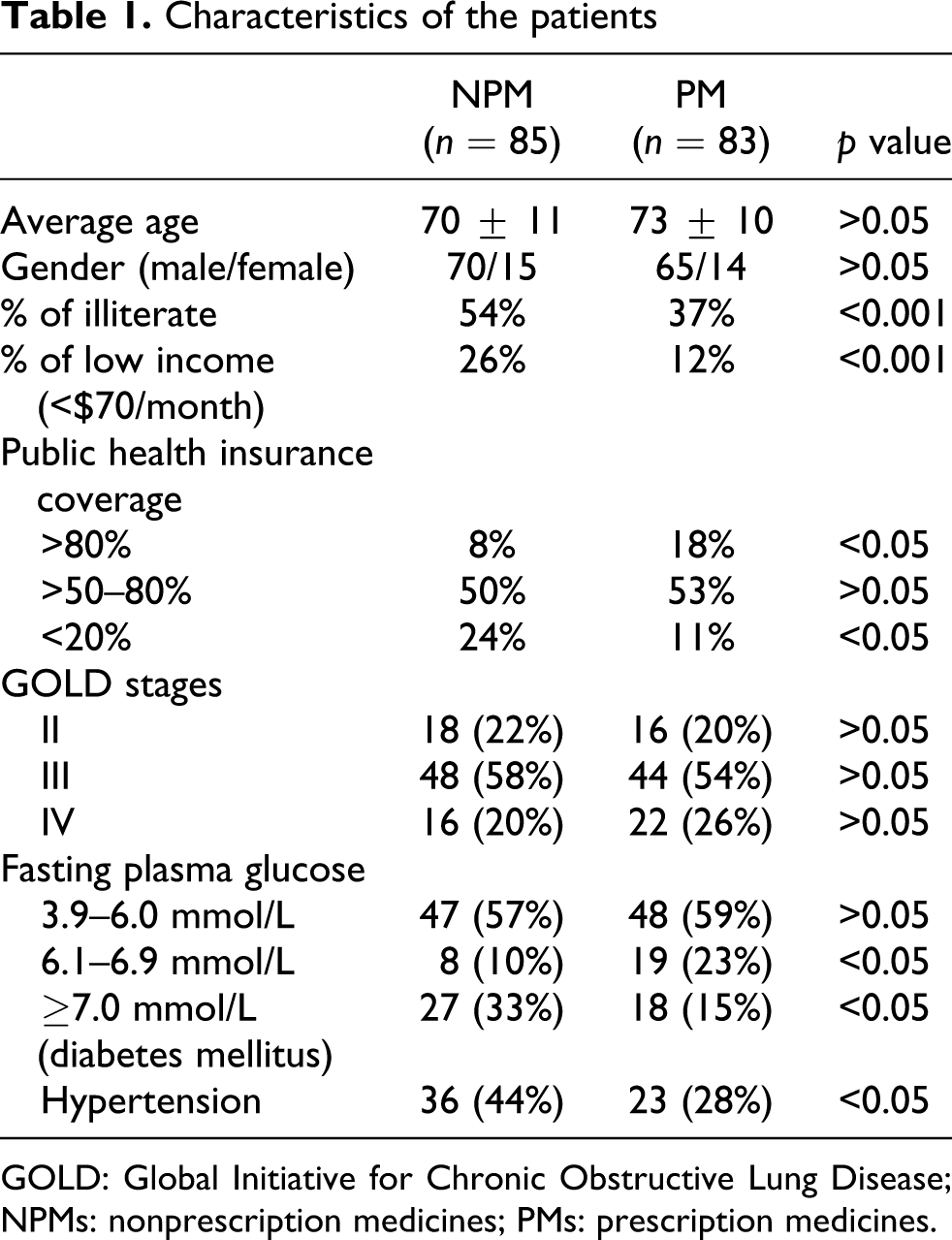
GOLD: Global Initiative for Chronic Obstructive Lung Disease; NPMs: nonprescription medicines; PMs: prescription medicines.
Questionnaire analysis of the quality of life by SGRQ scores indicated that there was significant difference in the total SGRQ scores (56.87 ± 12.99 vs. 52.13 ± 12.41, p = 0.021), symptoms (67.55 ± 15.81 vs. 57.92 ± 16.46, p = 0.00016), activities (62.16 ± 13.82 vs. 54.11 ± 14.61, p = 0.0003), and impacts (57.67 ± 15.33 vs. 52.11 ± 15.24, p = 0.0199) between these two groups of patients (Table 2). The number of acute exacerbation during the past year in the NPM group was greater than that in the PM group. However, the subjective evaluation for the approved drugs in the NPM group was significantly lower than that in the PM group.
Therapeutic effects of the drugs

NPMs: nonprescription medicines; PMs: prescription medicines; SGRQ: St George’s Respiratory Questionnaire.
The amount spent on drugs on a daily basis by patients in the NPM group was lower than that of the PM group (0.54 ± 0.31 $ vs. 2.1 ± 0.48 $, p < 0.001). Furthermore, 45% of patients in the NPM group spent $0.15/day on medical drugs, while only 35% of patients in the NPM group spent more than $0.8/day on medical drugs; all patients in the PM group spent more than $0.8 /day on medical drugs.
Analysis of 21 kinds of NPMs collected from 85 patients revealed that 15 kinds of NPM contained corticosterone (71%), with 10 containing prednisone, and another 5 containing dexamethasone. The mean concentration of prednisone was 5.05 ± 2.13 mg/g NPM. Following medical education, 51% of patients believed that they would not use the NPM, but 26% of patients said that they might use the NPM again, before discharge. Notably, 23% of patients still insisted that they would use the NPM in future. Further survey revealed that only 24% of patients did use the NPM again during the 6-month follow-up.
Discussion
In this study, we found that there were considerable number of COPD patients who used NPMs without a valid prescription in Chongqing, China. These NPMs often contained corticosteroids, which was associated with increased prevalence of type 2 diabetes and hypertension in COPD patients. Medical advice effectively prevented further usage of NPM in some COPD patients.
Further analysis revealed that low level of education, family income, and insurance coverage were the major factors associated with the use of NPM in COPD patients. The percentage of patients with low family income, education, or insurance coverage in the NPM patients was significantly higher than that in the PM group. Indeed, as many as 75% of COPD patients in the NPM group admitted that they did not think that the standard approved drugs were effective for COPD therapy. Patients with low family income and insurance coverage usually seek cheaper medicines that are affordable. Our results were partly consistent with a very recent study 13 that showed that lower educational attainment and household income in COPD patients were related to greater disease severity, poorer lung function, and greater physical functional limitations. Thus, it is important to strengthen the awareness of COPD and the standard therapy for COPD in the less educated and low-income patients, particularly for those with low insurance coverage.
The ease of access and broad availability of Internet pharmacies in China 8 may be another factor contributing to the use of NPM in those patients. According to Chinese law, prescription-only medicines must be sold or supplied ‘only in accordance with a prescription given by an appropriate practitioner.’ 14 However, the existence of counterfeit drugs in China has always been a critical problem, which cannot be overlooked. 15 ,16 Notably, over three quarters of the Web sites involved in online pharmacy business ignore the regulations, allowing consumers to self-prescribe. 9 Although some online pharmacies require a prescription, most of those pharmacies only require a prescription by fax or e-mail. 9 Therefore, new policies should be established and implemented for regulating and control of NPM access.
Furthermore, the use of NPM is dangerous to COPD patient. A previous study reported that more than half of the drugs sold online were fake or contained substandard chemicals. 8 Indeed, many NPMs contain ‘composition and ingredients’ without the correct scientific specifications and are consequently ineffective and often dangerous to patients. 17 We found that the composition and ingredients of most NPMs were not clearly specified in the labels. This lack of clarity of ingredients used in the NPMs may deliberately conceal the potential harmful effects on health. In addition, many NPMs contain unhealthy components that may cause adverse effects. Indeed, we found that 15 kinds of NPMs contained prednisone/dexamethasone. Although corticosteroids are used in the conventional treatment of severe COPD worldwide, 18 , 19 long-term use of corticosteroids has been proven to be dangerous for patients with mild and moderate COPD. 20 ,21 The percentage of patients with diabetes and hypertension in the NPM group was significantly higher than those in the PM group. Given that the long-term use of prednisone or dexamethasone is associated with the development of diabetes and hypertension, 22 ,23 it is possible that the use of NPM contributed to the development of these diseases (diabetes and hypertension) in the COPD patients. Moreover, a very recent meta-analysis report indicated that long-term corticosteroid inhalation was associated with a significantly increased risk of pneumonia. 24 In this study, we found conspicuously worse health status (SGRQ scores) and more frequent acute exacerbations in COPD patients in the NPM group during the past year. These results further support the notion that long-term use of corticosteroids, especially systemic corticosteroids, is evidently harmful to COPD patients.
More interestingly, we found that medical advice by health care providers is effective in reducing the use of NPM in COPD patients. Evidentially, 51% of patients in the NPM group considered not using NPM in future, and 76% of patients in the NPM group did not use NPM again, 6 months after the education. These findings are very encouraging and suggest that many patients have returned to the use of standard therapies for the treatment of COPD.
In conclusion, the present findings indicated that, in the Chongqing area of China, many patients with COPD used NPM that contained corticosteroids, which was associated with the development of diabetes and hypertension as well as resulted in worse health status in COPD patients. Low family income, education, and insurance coverage as well as easy of access and broad availability of NPMs were the major factors leading to the use of NPM in COPD patients. Medical advice by health care providers effectively reduced the use of NPMs in most patients with COPD. Therefore, it is important to encourage physicians to educate the patients regarding the importance of standard therapies for COPD and the harmfulness of NPMs. Moreover, strict regulations of the drug market by the Chinese government should also be considered in the future.
Footnotes
The role of each author in the study: Guoqiang Cao (Research Design), Lian Li and Haidong Li (collection data, Health education and advisement), Jing Li (radioimmunoassay, follow up), Fang-Wang (follow up, Health education and advisement), Hucheng Wang (statistical analysis), and Lin Zhang (HPLC analysis).
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.