
Abstract
Knowledge on the sequelae of Coronavirus Disease 2019 (COVID-19) remains limited due to the relatively recent onset of this pathology. However, the literature on other types of coronavirus infections prior to COVID-19 reports that patients may experience persistent symptoms after discharge. To determine the prevalence of respiratory symptoms in survivors of hospital admission after COVID-19 infection. A living systematic review of five databases was performed in order to identify studies which reported the persistence of respiratory symptoms in COVID-19 patients after discharge. Two independent researchers reviewed and analysed the available literature, and then extracted and assessed the quality of those articles. Of the 1,154 reports returned by the initial search nine articles were found, in which 1,816 patients were included in the data synthesis. In the pooled analysis, we found a prevalence of 0.52 (CI 0.38–0.66, p < 0.01, I 2 = 97%), 0.37 (CI 0.28–0.48, p < 0.01, I 2 = 93%), 0.16 (CI 0.10–0.23, p < 0.01, I 2 = 90%) and 0.14 (CI 0.06–0.24, p < 0.01, I 2 = 96%) for fatigue, dyspnoea, chest pain, and cough, respectively. Fatigue, dyspnoea, chest pain, and cough were the most prevalent respiratory symptoms found in 52%, 37%, 16% and 14% of patients between 3 weeks and 3 months, after discharge in survivors of hospital admission by COVID-19, respectively.
Introduction
The clinical presentation of the new Coronavirus Disease 2019 (COVID-19) can range from a mild infection to a severe illness. 1 It is estimated that close to 10% of hospitalised COVID-19 patients require admission to the Intensive Care Unit (ICU). 2 The most common symptoms present in the acute phase are fever, cough, dyspnoea, and fatigue. 3,4 Others symptoms are less frequent, such as sore throat, headache, and diarrhoea. 3,4
Length of hospital stay can range from days to weeks, depending on the patient’s own risk factors, the severity of the disease, etc. 5 The mean time of hospitalisation has been reported to range from 10 days to 1 month, 6 –8 indicating that COVID-19 patients may be subjected to a prolonged hospital stay. This introduces various complications (respiratory, cardiovascular, cognitive, physical, and psychological). 9,10 Among them we find a very characteristic phenomenon called ICU-acquired weakness (ICUAW). This is defined as diffuse, systematic, and generalised muscle weakness that develops after the onset of critical illness and incorporates critical illness polyneuropathy (CIP), critical illness myopathy (CIM), and critical illness neuromyopathy. 11 It is generally associated with sepsis, multiorgan failure, and persistent systemic inflammation. 11 Its prevalence varies between 25% and 57% and has been associated with a longer mechanical ventilation duration, days in ICU, and hospital stay. 12 In COVID-19 patients, there are still no long studies reporting the prevalence of ICUAW.
In the last months, the scientific literature uses a new term, ‘Long COVID’ to describe illness in people who have either recovered from COVID-19 but are still report lasting effects of the infection or have had the usual symptoms for far longer than would be expected. 13 The sequelae after discharge and their impact on quality of life of the patient are not yet fully known. Some authors have reported lung damage in severe COVID-19 cases, such as fibrotic remodelling of the lung parenchyma 14,15 with pulmonary function impairment, 16 along with the persistence of symptoms for weeks to months after discharge. 17 The symptoms, like fatigue or dyspnoea, are patients reported outcomes and play an essential role in increasing patient engagement, improving health systems, and ensuring that clinical care and research is person-centred. 18
Following the acute phase of COVID-19, there is increasing awareness of patients with ‘long COVID’ in whom residual symptoms persist beyond the acute viral illness. 13 Among the persistent symptoms we can find a high prevalence of respiratory symptoms such as fatigue, dyspnoea, cough, and chest pain. 17 –21 The persistence of these symptoms can negatively impact quality of life, affecting one in three patients, both in patients with or without comorbidities. 18 In addition, in subjects of working age it can delay return to work. 19,22
The mechanisms of why patients may report persistent respiratory symptoms have not yet clearly been established, but probably are related to the pathophysiological mechanism that occurs during the disease. One possible explanation is the association of COVID-19 with a severe systemic inflammatory reaction and vasculopathy responsible for endothelial lesions. 23 Additionally, pulmonary interstitium changes may be due to inflammatory cell infiltration, oedema, and interstitial thickening, whereas pulmonary parenchyma changes could reflect oedema, alveolar haemorrhage, cell exudation and hyaline membrane formation. 24 To fill this gap, the PHOSP-COVID study aims to determine the prevalence and impact of COVID-19 on lung parenchymal, airway and vascular damage, as well as determining the effects of COVID-19 across various organ systems. 25
Due to the high number of patients who are hospitalised for COVID-19, and because it is essential to detect the persistent respiratory symptoms to plan follow-up and possible interventions to manage the Long COVID syndrome, we decided to carry out a systematic review and meta-analysis aimed to determine the prevalence of respiratory symptoms in survivors of hospital admission after COVID-19 infection.
Methods
We conducted a systematic review of the literature using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (25). The review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42020215533)
Criteria for considering the studies in this review
The inclusion criteria for the systematic review were a) randomised controlled trials (RCT) and observational studies (retrospective, prospective, cross-sectional, longitudinal, case-control and cohort), b) whose objective was to determine the prevalence of respiratory symptoms in patients presenting with COVID-19, c) laboratory-confirmed COVID-19 infection by quantitative real-time polymerase chain reaction (qRT-PCR) or polymerase chain reaction dual fluorescence (PCR), d) hospitalised adult patients (≥ 18 years), e) follow-up from 30 days after Covid-19 infection, f) follow-up from 21 days after hospital discharge. The exclusion criteria were: a) systematic reviews, protocol studies, case reports, studies showing the effects of medical or other intervention. No other restrictions in eligibility criteria were applied.
Search strategy and data sources
A comprehensive primary literature search was performed using the Embase, Cochrane Central Register of Controlled Trials (CENTRAL), CINAHL, Web of Science, PubMed / MEDLINE databases. The search covered the period from December 2019 to October 22, 2020. The terms used were: a) For condition: COVID-19 OR coronavirus disease OR SARS-CoV-2 OR 2019 novel coronavirus disease OR 2019-nCoV infection AND after discharge OR at discharge OR post COVID OR after acute phase OR follow up. b) For the main outcome: fatigue OR dyspnea OR dyspnoea OR shortness of breath OR breath shortness OR breath shortnesses OR breathlessness OR tachypnoea OR chest pain OR cough OR rhinitis OR rhinitides OR mucus OR nasal catarrh OR sputum production OR sore throat. c) For population: adult OR older people OR elderly OR aged. The primary search was supplemented by a manual search of the references of the included articles. Eventually, accepted or in press publications (which may be available on pre-print servers and journal websites may be missed using the authors’ search strategy) for this reason, an expert on the field was asked about any important studies. We imposed no language restrictions. All articles found were exported into Rayyan web software. 26
Reviewing procedure and study selection
Two review authors (KCM and YMJ) independently screened titles and abstracts. We selected all articles that were deemed potentially eligible by at least one of the reviewers. Two of the review authors (KCM and YMJ) independently considered the full records of all potentially relevant studies for inclusion by applying the selection criteria. Any disagreement was solved by a third reviewer (RTC). All studies that did not fulfil the predefined criteria were excluded, and their bibliographic details were listed with the specific reason for exclusion.
Data extraction
Two review authors (KCM and YMJ) independently extracted data from all included studies. The database was then verified, and discrepancies were resolved by a third review author (RTC). The summary of the selected variables included: author, country, type of study, sample size, age, anthropometric characteristics (Body Mass Index (BMI) or weight), length of hospital stay, time of assessment, severity of patients, cases with and without respiratory symptoms (fatigue, dyspnoea, cough, chest pain, sore throat, sputum production, and rhinorrhoea). If some relevant data were not in the article, the author was contacted to request the information.
Assessment of methodological quality
The risk of bias and the quality of observational and interventional studies was assessed using the corresponding assessment tools recommended by the National Heart, Lung, and Blood Institute (NHLBI). 27 The assessment was performed by two review authors (KCM–YMJ), any disagreement was resolved by a third review author (RTC). The criteria were evaluated as ‘Yes’, ‘No’, or ‘Other’ (not applicable, not reported, or not determinable), and an overall rating was provided for each study based on the items rated with an affirmative answer: ≥ 75% = good, 50–75%= fair, ≤ 50% = poor.
Statistical analysis
We used MetaXL software version 5.3 (EpiGear International, Sunrise Beach, Queensland, Australia) for the meta-analysis and generation of a forest plot that showed combined estimates with a 95% confidence interval. We pooled the prevalence around individual outcomes using the double arcsine transformation method. 28 We obtained combined measurements of effect for each primary outcome through meta-analysis under a random-effect model due to the expected heterogeneity between studies. 29 Statistical heterogeneity was measured through the I 2 statistic and classified as low (I 2 < 25%), moderate (I 2 25–50%), or high (I 2 > 50%). 30
Results
Study selection
The search found 1,154 potential studies (1,150 from selected databases and 4 from manual searches). Among these, 164 correspond to duplicates. We screened 990 titles and abstracts and excluded 963 records which did not meet our inclusion criteria. 27 articles were assessed as full text, of which 17 articles were excluded due to wrong outcome (n = 6), wrong population (n = 5), wrong study design (n = 4), duplicate data (n = 1) and for being preprint (n = 1). Finally, 10 articles were included for analysis. 17 –22,31 –34 The flow chart of the study selection process is shown in Figure 1.

Study selection process.
Characteristics of the included studies
Eight studies were conducted in Europe, 17,19 –22,31,32,34 1 in Asia, 33 and 1 in North America. 18 The designs of the studies included 5 prospective, 17,18,31,33,34 1 retrospective, 20 1 bidirectional, 32 and 3 cross-sectional. 19,21,22
Participants
In total, 1,816 subjects were included. The sample sizes varied between 78 18 and 538 33 participants. The studies included 809 females and 1,007 males, mean age varied between 49 ± 15 31 and 63.2 ± 15.7. 19 The mean hospital stay varied between 6.5 (IQR 4–10.75) days 21 and 13.5 ± 9.7 days, 17 two studies did not report it. 18,31 Nine studies reported the persistence of respiratory symptoms between 3 weeks to 3 months after discharge of COVID-19 infection, 17,18,20 –22,31 –34 and one study reported the persistence of respiratory symptoms after 3 months of hospital admission 19 (Table 1). The method used to register the symptoms was phone interview in four studies, 19,22,31,33 hospital visit in five studies, 17,18,21,32,34 and one study did not report a method. 20
Characteristics of the included studies.

Data are shown as Mean±SD, Median (
Abbreviations:
Methodological quality assessment
We used the NHLBI’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies in the 10 studies, with one being rated as ‘good’, 32 six being rated as ‘fair’ 17,19,21,22,31,33 and three being rated as ‘poor’ 18,20,34 (Supplementary file S1).
Main results
Fatigue
Eight studies reported fatigue, including 1,668 subjects. 17,19 –22,31,33,34 The instruments used were visual analogue scale, 21,22,34 fatigue according to the World Health Organization (WHO) performance status classification, 31 and presence/absence of symptoms. 17,19,20,33 One author did not report the method of data collection. 18 In the pooled analysis, the prevalence was 0.52 (CI 0.38–0.66) with high heterogeneity (I 2 = 97%) with a p < 0.01 (Figure 2, Table 2).
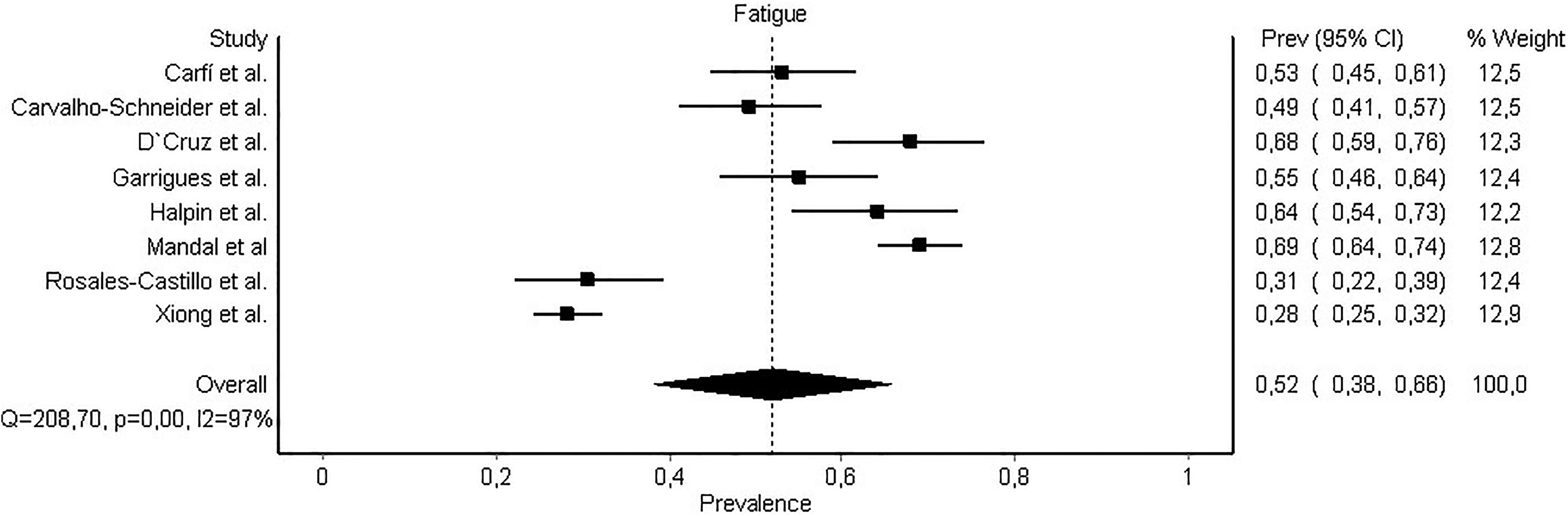
Prevalence of fatigue.
Number of patients with symptoms in included studies.

Dyspnoea
Nine studies reported dyspnoea, including 1,334 subjects. 17 –22,31,32,34 The instruments used were visual analogue scale, 21,22,34 the modified Medical Research Council scale (mMRC), 19,31,32,34 and the presence/absence of symptoms. 17,20,33 In the pooled analysis the prevalence was 0.37 (CI 0.28–0.48) with a high heterogeneity (I 2 = 93%) with a p < 0.01 (Figure 3, Table 2).

Prevalence of dyspnoea.
Chest pain
Five studies reported chest pain, including 1066 subjects. 17,19,31,33,34 This symptom was reported by the presence/absence 17,19,31,33 and one study used the visual analogue scale. 34 In the pooled analysis, the prevalence was 0.16 (CI 0.10–0.23) with high heterogeneity (I 2 = 90%) with a p < 0.01 (Figure 4, Table 2).

Prevalence of chest pain.
Cough
Seven studies reported cough, including 1,496 subjects. 17 –21,33,34 This symptom was reported by the presence/absence, 17 –20,33 and two studies used the visual analogue scale. 21,34 In the pooled analysis the prevalence was 0.14 (CI 0.06–0.24) with a high heterogeneity (I 2 = 96%) with a p < 0.01 (Figure 5, Table 2).

Prevalence of cough.
Other symptoms
Two studies reported sore throat and sputum production, present in 27 (4%) and 28 (4.1%) subjects respectively 17,33 ; and one article reported rhinorrhoea present in 19 subjects (13.3%). 17
Discussion
Principal findings
Fatigue, dyspnoea, chest pain, and cough were the most prevalent respiratory symptoms found in 52%, 37%, 16%, and 14% in survivors of hospital admission by COVID-19 infection, respectively.
Comparison with other studies
Although the respiratory symptoms were analysed individually in this systematic review, it is necessary to emphasise that persistent symptoms can coexist in the same patient. In a prospective study in 143 patients at approximately 2 months of follow-up, Carfí et al. indicated that 32% had 1 or 2 symptoms, and 55% had three or more. 17 These findings were confirmed by Huang et al., who showed that 76% of patients reported at least one symptom in an ambi-directional cohort study with more than 1700 patients at 6 months after symptom onset. 35 Until now, it have been proposed that the persistence of symptoms in COVID-19 patients may be due to a prolonged state of convalescence due to the strong inflammatory response. 31
Unlike dyspnoea, cough, and chest pain, fatigue is not exclusively a respiratory symptom. However, we decided to include it in this review as it is a multidimensional problem that overlaps with dyspnoea, and even with psychological distress and cognitive dysfunction. 22 Furthermore, fatigue can occur as a consequence of respiratory system alterations and is commonly assessed in patients with chronic respiratory diseases. 36
The intensity of the symptoms is difficult to objectify, indeed, it is essential to emphasise that there are validated tools in other diseases that determine each symptom’s intensity and characteristics. 37 For example, in fatigue, there is the fatigue assessment scale (FAS), 37 instrument used to assess patients with sarcoidosis that has been used in COVID-19 patients, 38 but is not currently validated in this population. The same happens in dyspnoea with mMRC, which is reported only by 2 studies. 19,32 Although they are not yet validated for COVID-19, one should look for scales that better define the disease’s intensity and affectation in people.
Prevalence of respiratory symptoms in working age subjects, as recent studies have reported, 17,18,32,33 may mean the impossibility of returning to work. Carvalho-Schneider et al. 31 in a 2-months follow-up of 150 patients, founded significant prolonged symptoms associated with those aged 40 to 60 years, and Garrigues et al. 19 in a 3-months follow-up of 120 patients, reported that only 46% of patients admitted to the ICU returned to work versus 77% of patients in the general ward, at a follow-up of 110 days. Also, Halpin et al. reported that only 10% of patients who recovered from COVID-19, who was in an ICU, returned to their original job 4 to 8 weeks post-infection. 22 In a 6-month follow up, Huang et al., did not report if patients are workers, but it es very probable because the mean age was 57.0 (IQR 47.0–65.0). 35
It would have been interesting to differentiate the prevalence of respiratory symptoms according to severity. However, until the time of the review few studies made this classification of patients. 19,22,33 Garrigues et al. and Xiong et al., both in 3-month follow-up, point out that there were no statistically significant differences between the ICU group and patients in the general ward. 19 However, Halpin et al. mention that dyspnoea and fatigue have a higher prevalence in patients who required ICU care than those who were managed in less complex wards. 22 Interestingly, Xiong et al., found that the duration of virus shedding after COVID-19 onset and hospital length of stay were longer in survivors with fatigue, 33 but the others studies included did not report it. Interestingly, Arnold et al. demonstrated the persistence of symptoms at 8–12 weeks, even those admitted with mild disease. 39 Although persistent symptoms are more likely to be found in more severe patients; all patients should be evaluated regardless of severity.
The symptoms have a multifactorial origin. Their perception is due to organic component; however, their presence is also related to psychological and mental health factors. Thus, it is essential to consider the mental health of patients. D’Cruz et al. founded a post-traumatic stress disorder, anxiety and depression in 25, 22 and 18% of patients 2 months after severe COVID-19 pneumonia, respectively. 34 These findings were confirmed by Huang et al., who described the same mental health disorders in addition to sleep difficulties in a 6-month follow-up.
An important aspect to consider is the presence of previous chronic respiratory diseases that can influence the perception of respiratory symptoms. In general, most of the articles included had a prevalence of asthma or chronic respiratory disease (COPD) in less than 10% of the patients, except for Halpin et al. (30%), Rosales-Castillo et al. (20%) and D’Cruz et al. (11%). 20,22,34 In particular, Halpin et al., reported dyspnoea in 50% of his patients, higher than the average of 37% among all included studies. 22
According to ethnic origin, most studies did not report it. However, Halpin et al., described that among all patients for whom ethnicity was known, 8/19 (42.1%) of Black Asian and Minority Ethnic (BAME) participants reported moderate or severe breathlessness, compared with 18/72 (25.0%) of white patients. In future studies with larger samples, this factor can be analysed to confirm these findings. 22
Implications for clinical practice
The wide range of persistent respiratory symptoms seen in the included studies re-enforces the importance of a holistic approach recommended by the guidelines. 40 The sequelae left by COVID-19 and the persistent symptoms after discharge agree with what was seen in previous years with Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS), where it was reported that hospitalised patients presented physical and psychological sequelae up to 6 months and 1 year, respectively. 41,42 The follow-up of these patients is essential, not only in the physical field but also in the biopsychosocial field. It represents a tremendous logistical and economic challenge, as a follow-up implies; therefore, a rigorous selection of patients who benefit from these follow-up programmes are generally patients who developed more severe disease. This is in order to intervene in the post-acute phase of the patients, contributing to social and labour reintegration and quality of life. 9,43
Finally, in the follow-up of COVID-19 patients, we need to register the persistence of respiratory symptoms such as pulmonary function, radiological imaging, electrocardiography, or other specific tests, with a subsequent evaluation at 3 and 6 months after discharge. 44,45
Limitations
A limitation of the study is the heterogeneity of the severity that the population presented post COVID-19 in the included studies. Therefore, the meta-analysis generated shows greater heterogeneity of the respiratory symptoms described. The possible reasons for this high heterogeneity are given by the different populations studied, with different degrees of severity and evaluated at different times. Unfortunately, there was also no uniformity in the description of the time after discharge, since some authors reported the time after the onset of symptoms.
Conclusion
Fatigue, dyspnoea, chest pain, and cough were the most prevalent respiratory symptoms found in 52%, 37%, 16% and 14% in survivors of hospital admission after COVID-19 infection, respectively.
In future studies, the researchers must consider reporting their data in a similar way (validated instruments by each symptom, including discharge time and severity of patients) to facilitate the comparison across studies.
Supplemental material
Supplemental Material, sj-docx-1-crd-10.1177_14799731211002240 - Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis
Supplemental Material, sj-docx-1-crd-10.1177_14799731211002240 for Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis by Kevin Cares-Marambio, Yessenia Montenegro-Jiménez, Rodrigo Torres-Castro, Roberto Vera-Uribe, Yolanda Torralba, Xavier Alsina-Restoy, Luis Vasconcello-Castillo and Jordi Vilaró in Chronic Respiratory Disease
Footnotes
Abbreviations
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.