
Abstract
Patients with chronic obstructive pulmonary disease (COPD) usually complain of symptoms such as cough, sputum, wheezing, and dyspnea. Little is known about clinical symptoms in individuals with restrictive ventilatory impairment. The aim of this study was to compare the prevalence and type of respiratory symptoms in patients with COPD to those reported by individuals with restrictive ventilatory impairment in the Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar study. Between 2002 and 2004, individuals ≥40 years of age from five cities in Latin America performed pre and post-bronchodilator spirometry and had their respiratory symptoms recorded in a standardized questionnaire. Among the 5315 individuals evaluated, 260 (5.1%) had a restrictive spirometric diagnosis (forced vital capacity (FVC) < lower limit of normal (LLN) with forced expiratory volume in the first second to forced vital capacity ratio (FEV1/FVC) ≥ LLN; American Thoracic Society (ATS)/European Respiratory Society (ERS) 2005) and 610 (11.9%) were diagnosed with an obstructive pattern (FEV1/FVC < LLN; ATS/ERS 2005). Patients with mild restriction wheezed more ((30.8%) vs. (17.8%); p < 0.028). No difference was seen in dyspnea, cough, and sputum between the two groups after adjusting for severity stage. The health status scores for the short form 12 questionnaire were similar in restricted and obstructed patients for both physical (48.4 ± 9.4 vs. 48.3 ± 9.8) and mental (50.8 ± 10.6 vs. 50.0 ± 11.5) domains. Overall, respiratory symptoms are not frequently reported by patients with restricted and obstructed patterns as defined by spirometry. Wheezing was more frequent in patients with restricted pattern compared with those with obstructive ventilatory defect. However, the prevalence of cough, sputum production, and dyspnea are not different between the two groups when adjusted by the same severity stage.
Introduction
Restrictive ventilatory impairment and chronic obstructive pulmonary disease (COPD) are important causes of morbidity and mortality. 1 Mannino et al. 2 demonstrated that both obstructive and restrictive impairments are associated with an increased risk of mortality when adjusted for age, gender, race, and smoking status.
In a recent study from Spain (EPI-SCAN) Study, Soriano et al. 3 showed that restrictive ventilatory impairment is more prevalent (12.7%) than chronic airflow limitation with a highly variable geographical distribution. Mannino et al. 4 showed that restrictive ventilatory impairment was a common finding in the Burden of Lung Disease study (11.7%) and that the prevalence increased to close to 15% in people above 70 years of age. In addition, both studies used the forced expiratory volume in the first second to forced vital capacity ratio (FEV1/FVC) over 0.70 and FVC less than 80% as the surrogate variables to diagnose the restrictive ventilatory impairment. Although a true restrictive impairment can only be diagnosed by the demonstration of a reduced total lung capacity (TLC) < lower limit of normal (LLN), a reduced FVC has been associated with reduced TLC, and has been accepted as a surrogate marker for restriction in epidemiological studies. 3 However, the use of the fixed ratio method for the diagnosis of restrictive ventilatory impairment as well as for the diagnosis of obstructive ventilatory impairment may lead to misdiagnosis. 5,6 A more rigid method for the diagnosis of a restrictive ventilatory defect using the FEV1/FVC ratio higher than the LLN and the FVC lower than the LLN decreases the possibility of misdiagnosis. 6,7
Cough, sputum, dyspnea, and wheezing are the most common respiratory symptoms in the Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar (PLATINO) population study. 8 However, little is known about the frequency of the respiratory symptoms among persons with spirometric evidence of restrictive ventilatory impairment. Indeed, in that study a high prevalence of respiratory symptoms was reported (and state the prevalence) among individuals with spirometric restrictive physiology but the relationship between symptoms and the different stages of impairment was not explored. Also, to our knowledge, no study has ever compared the occurrence of respiratory symptoms in persons with restrictive ventilatory impairment as compared to persons with COPD, stratifying it by severity of disease in a population-based cohort.
Our objectives were to determine the prevalence of restrictive ventilatory impairment in the PLATINO study and to compare the occurrence of respiratory symptoms in persons with spirometric evidence of restrictive ventilatory impairment with those occurring among patients with fixed airflow obstruction (COPD), adjusting for spirometric disease severity.
Methods
The PLATINO study 9 was a population-based epidemiologic study conducted in five major Latin American cities: São Paulo (Brazil), Santiago (Chile), Mexico City (Mexico), Montevideo (Uruguay), and Caracas (Venezuela). Complete details of the PLATINO methodology have been published. 10 A two-stage cluster sampling method was used at each site in order to obtain a random sample of households. All adults ≥40 years old living in selected households were invited to participate. The sample studied was selected in several stages. The metropolitan area was first stratified into the main city and surrounding municipalities. These two subsets were further stratified by socioeconomic status. We selected 68 census tracts at each site, taking stratification into account and using a probability of selection proportional to the number of households in each tract. Within each tract, we counted the number of people in each household and every count was updated from the most recent census. We chose an average of 15 households using systematic sampling within each tract. All adults aged 40 years or more living in the selected households were invited to participate and were submitted to the evaluations in their own homes after signing an informed consent form to participate in the study. Sample size calculations suggested that 800 people would be needed in each area to estimate a prevalence of up to 30% with a margin of error of less than 4% points. We aimed to locate about 1020 eligible participants per site, with a predicted 20% refusal rate. Eligible individuals, in this study, were males and females ≥40 years of age with individuals with restrictive ventilatory impairment and COPD according to American Thoracic Society (ATS)/European Respiratory Society (ERS) 2005 guideline. The local ethical committee of each institution involved in the study approved the protocol, and all subjects gave their written informed consent. The PLATINO study was primarily delineated to collect information on factors that potentially could be associated with COPD, including age, gender, ethnicity (self-reported), smoking habits, years of formal education, employment, respiratory symptoms, and prior spirometric testing. Copies of the questionnaires used at each site are available at the PLATINO Web site (http://www.platino-alat.org). Some questions regarding respiratory symptoms are listed: Do you usually have cough in the absence of a cold? Yes/No; Do you cough most of the days, at least three times per week, each year? Yes/No; Do you have sputum most of the days, at least three times per week, each year? Yes/No; Did you have chest wheezing in the past 12 months only when you had a cold? Yes/No; Do you have shortness of breath when walking faster on flat ground or on a slight slope? Yes/No; Do you have to walk slower than others your age on flat ground due to shortness of breath? Yes/No. All questions were completed personally.
A portable, battery-operated, ultrasound transit-time-based spirometer (EasyOne; NDD Medical Technologies, Chelmsford, Massachusetts, USA) was used to perform pulmonary function testing among eligible subjects. Each day, the calibration was checked with a 3-L syringe. Subjects performed up to 15 forced expiratory maneuvers (average, 5–6 maneuvers) to obtain three acceptable maneuvers according to the ATS, with FVC and FEV1 reproducible within 150 mL. Salbutamol (400 μg) was then administered by inhalation using a 500 mL spacer, and the test was repeated 15 minutes later (average, 4–5 maneuvers). The spirometric tests were done with the subject seated, using a nose clip and a disposable mouthpiece. Health-related quality of life (HRQL) was evaluated with the short form 12 (SF-12) questionnaire.
Reference values for spirometry
The PLATINO equation developed by Pérez-Padilla and colleagues was used for healthy individuals. 11 The percent of predicted values and LLN (5th percentile) were estimated based on this equation by subtracting 1.645 times the mean standard deviation of the variables mentioned above. The ATS/ERS 2005 criterion was considered to characterize restrictive ventilatory impairment (FVC < LLN and FEV1/FVC > LLN) and airflow obstruction (FEV1/FVC < LLN).
Statistical analysis
Continuous variables are reported as mean ± SD. Categorical variables are expressed in absolute numbers and percentage of the total. The Student’s t-test for independent samples was used to compare two continuous variables. For additional analyses, Levene’s test was used. Levene’s test is a test of the equality of variances, used with the independent t-test. Pearson χ 2 test was used for categorical variables for equality of variances and to compare the proportion in independent groups. Statistical significance was set at p < 0.05. The analysis was conducted using SPSS software version 16. Thus far, there is no study with an epidemiological design to analyze the prevalence of restrictive impairment. Consequently, since we used the PLATINO study data, which have been designed to study the prevalence of COPD, we calculated the power of the analysis for respiratory symptoms in individuals with restrictive ventilatory impairment and obtained a value of at least 85%. This way, the sample size was calculated based on degrees of freedom (n − 1; respiratory symptoms versus restrictive ventilatory impairment). The level of significance was set at p < 0.05 and a sample size of 870 with a power greater than 85%. 12
Results
Detailed descriptions of participation rates and the patient sample characteristics in the study, both for total and individual countries, have been published previously. 9 In summary, from a total of 6711 eligible individuals, complete interviews were achieved in 5571 subjects and spirometry was performed in 5315 subjects. According to the ATS/ERS 2005 criteria, 260 (5.1) of individuals had spirometric evidence of restrictive ventilatory impairment and 610 (11.9) had spirometric evidence of airflow obstruction. Prevalence of restrictive ventilatory impairment in the PLATINO study and individual distribution by city are presented in Figure 1.

Prevalence of restrictive ventilatory impairment in the PLATINO study and individual distribution by city. PLATINO: Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar.
The characteristics of the subjects included are presented in Table 1. The obstructed group was older and had more men than the restrictive ventilatory impairment group; the restrictive ventilatory impairment group had more women, with higher body mass index (BMI) and a higher proportion of overweight patients. The variables pack/years and HRQL (SF-12) were not different between the two groups.
Baseline characteristics of individuals with restrictive ventilatory impairment and COPD according to ATS/ERS 2005 guideline (PLATINO study).a
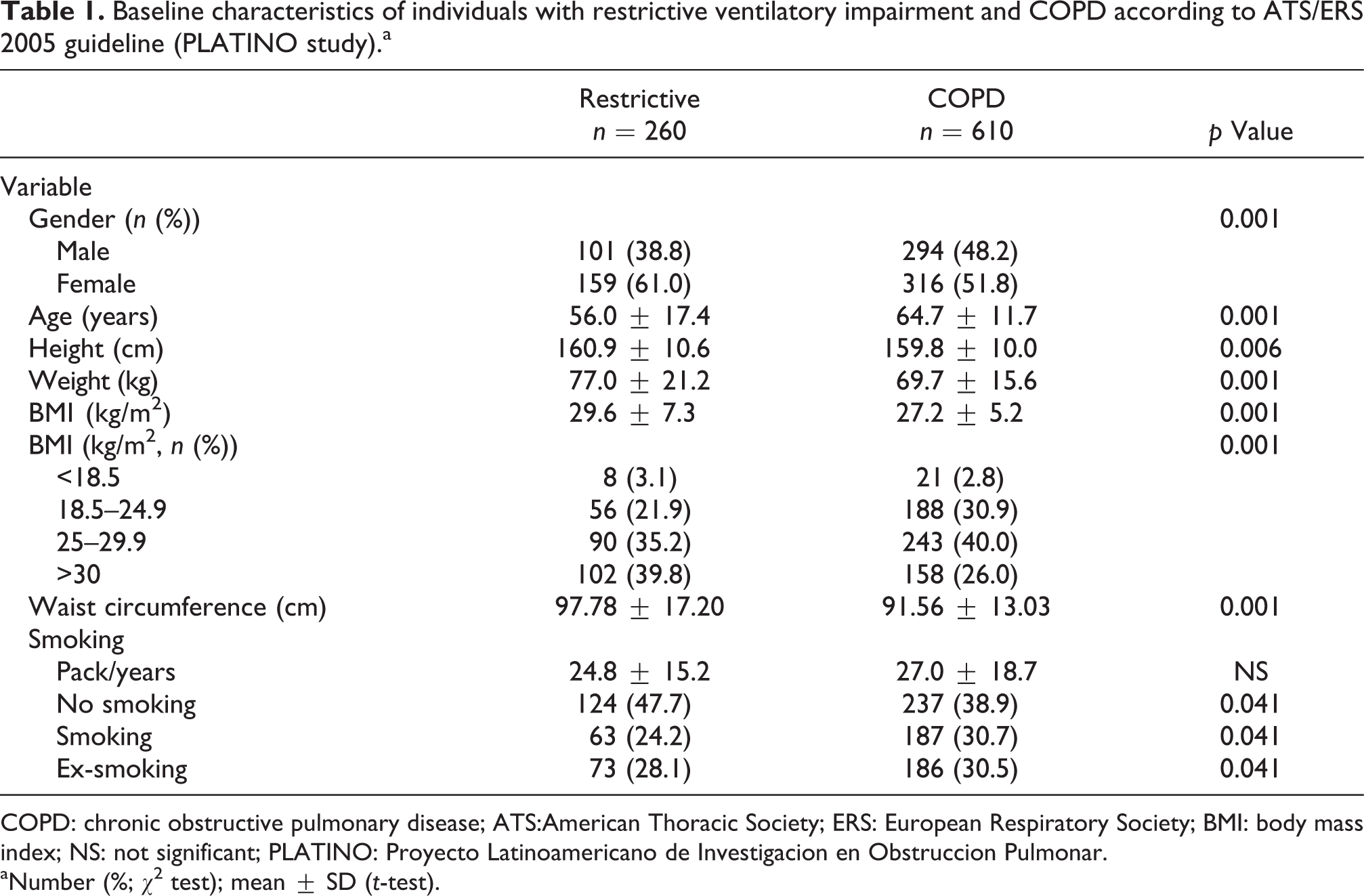
COPD: chronic obstructive pulmonary disease; ATS:American Thoracic Society; ERS: European Respiratory Society; BMI: body mass index; NS: not significant; PLATINO: Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar.
aNumber (%; χ2 test); mean ± SD (t-test).
The FVC (L), FVC (% predicted) and FEV1 (% predicted), and pre- and post-bronchodilator (BD) test were lower in the restrictive ventilatory impairment group (p < 0.001; Table 2). According to the staging classification based on FEV1, the restrictive ventilatory impairment group had a higher number of moderate patients (42.3%) than the COPD group (21.8%; p < 0.001), while the COPD group showed higher number of mild (59.8%) and very severe patients (18.4%, p < 0.001; Table 3). The comparison of respiratory symptoms by severity in both restrictive and COPD groups are shown in Table 4.
Lung function characteristics of individuals with restrictive ventilatory impairment and COPD according to ATS/ERS 2005 Guideline (PLATINO study).

ATS:American Thoracic Society; ERS: European Respiratory Society; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; COPD: chronic obstructive pulmonary disease; BD: bronchodilator test; NS: not significant; PLATINO: Proyecto Latinoamericano de Investigacion en Obstruccion Pulmonar.
aMean ± SD (t-test).
Severity staging distribution for restrictive and COPD groups according to ATS/ERS 2005 criteria.a

COPD: chronic obstructive pulmonary disease; ATS:American Thoracic Society; ERS: European Respiratory Society.
aNumber (%; χ2 test).
Frequency of respiratory symptoms in both restrictive and COPD groups according to 2005 ATS/ERS severity staging.
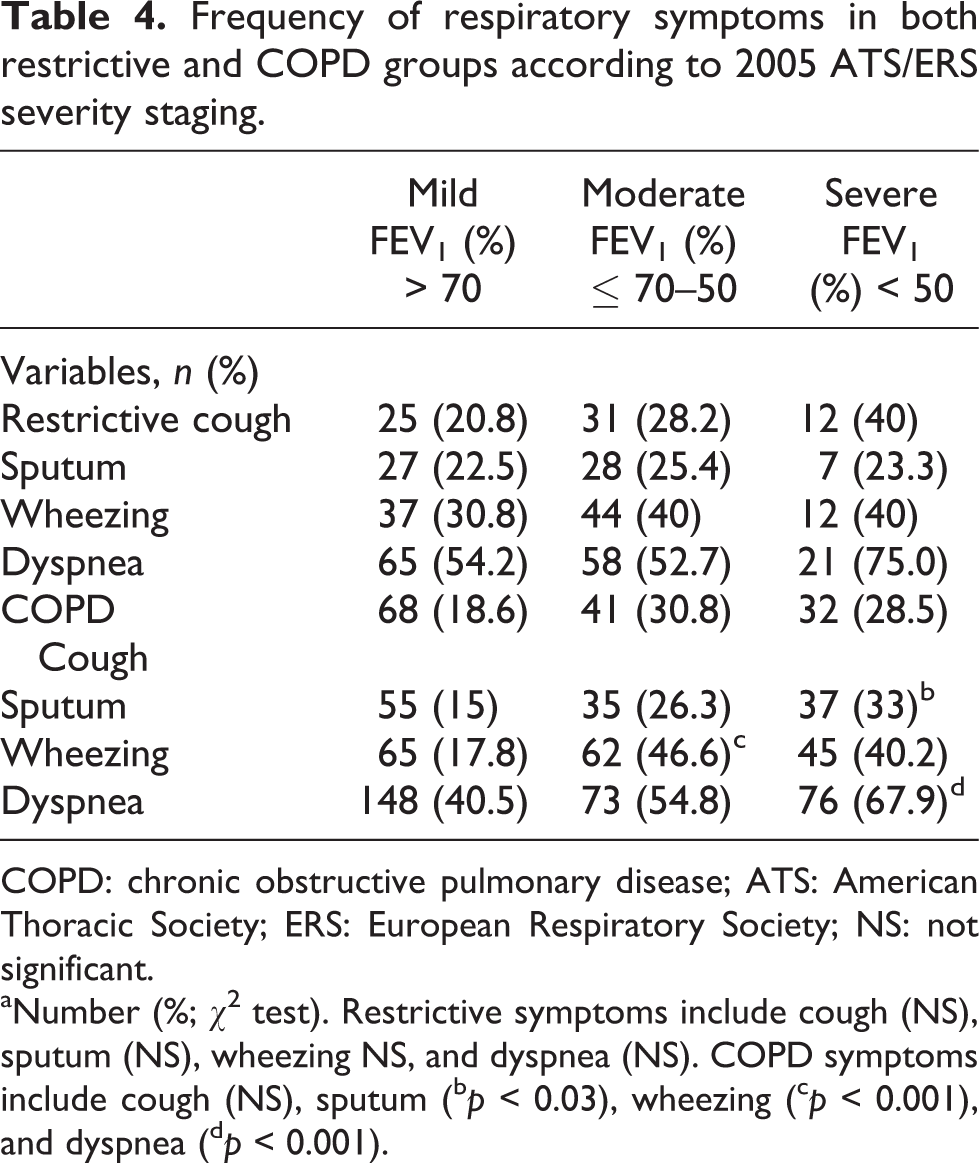
COPD: chronic obstructive pulmonary disease; ATS: American Thoracic Society; ERS: European Respiratory Society; NS: not significant.
aNumber (%; χ2 test). Restrictive symptoms include cough (NS), sputum (NS), wheezing NS, and dyspnea (NS). COPD symptoms include cough (NS), sputum (b p < 0.03), wheezing (c p < 0.001), and dyspnea (d p < 0.001).
There was no difference in the occurrence of symptoms between the restrictive ventilatory impairment and COPD groups, except for wheezing, which was more prevalent in the mild restrictive group (Figure 2).

Frequency of symptoms in the restrictive and COPD  groups according to ATS/ERS 2005 criteria: mild (FEV1 > 70%), moderate (FEV1 ≤ 70–50%), and severe (FEV1 < 50%). There was no difference within each staging group between persons with restrictive impairment compared with COPD, except for wheezing, which showed a difference in the mild stage (*p < 0.028). This same picture shows that the most frequent symptom among groups was dyspnea. COPD: chronic obstructive pulmonary disease; ATS:American Thoracic Society; ERS: European Respiratory Society; FEV1: forced expiratory volume in the first second.
groups according to ATS/ERS 2005 criteria: mild (FEV1 > 70%), moderate (FEV1 ≤ 70–50%), and severe (FEV1 < 50%). There was no difference within each staging group between persons with restrictive impairment compared with COPD, except for wheezing, which showed a difference in the mild stage (*p < 0.028). This same picture shows that the most frequent symptom among groups was dyspnea. COPD: chronic obstructive pulmonary disease; ATS:American Thoracic Society; ERS: European Respiratory Society; FEV1: forced expiratory volume in the first second.
Dyspnea was the most frequent symptom in both groups (Figure 2), occurring in 177 (68%) persons with restrictive physiology and 458 (75%) persons with airflow obstruction. There was no difference in the distribution of the number of symptoms between persons with restrictive physiology as compared to those with obstruction; approximately 60% of individuals in each of the two groups showed none or only one respiratory symptom (Figure 3). There was a high proportion of patients with severe impairment with just one symptom (Figure 4).

Frequency of number of respiratory symptoms among individuals with restrictive ventilatory impairment and COPD according to ATS/ERS 2005 criteria. COPD: chronic obstructive pulmonary disease; ATS:American Thoracic Society; ERS: European Respiratory Society.

Frequency of number of respiratory symptoms in individuals with restrictive ventilatory impairment and COPD according to severity. (Dotted line separates the proportion of individuals with 0 and 1 respiratory symptom among other respiratory symptom.) When looking at the number of respiratory symptoms in the group with restrictive ventilatory impairment and COPD, we observe that majority of individuals do not present respiratory symptoms or have only one symptom. A great proportion of severe patients present only one respiratory symptom. However, as the proportion of patients decrease, the number of symptoms increases to two, three or four respiratory symptoms. *p < 0.05: significance in the comparison between disease severity and number of symptoms.
There was no difference in the physical and mental domains of the HRQL in individuals with restrictive impairment or COPD. Dyspnea showed a correlation with both physical and mental domains of the questionnaire r = −0.33 and r = −0.23 (p < 0.001), respectively.
Discussion
This analysis of the PLATINO population study had three main findings. First, patients with restrictive pattern on spirometry have a similar prevalence of the respiratory symptoms (cough, dyspnea, and sputum production) to patients with obstructive pattern. They also had similar scores on the SF-12 health status questionnaire. Second, the total number of symptoms experienced by both groups was low. The prevalence of respiratory symptoms was relatively low in both groups of subjects. The most common respiratory symptoms in respiratory diseases are cough, sputum production, dyspnea, and wheezing. Patients with respiratory diseases usually underestimate mild symptoms and attribute them to other factors, such as tobacco smoking and aging. 13 Also, some patients with airflow obstruction may chronically adapt to the increased airway resistance and report decreased perception of bronchial tone. 14 Consequently, they tend not to seek medical care until they develop worsening of symptoms or significant functional limitations. 15 Patients should be requested about respiratory symptoms and, if risk factors are present, pulmonary function evaluation should be requested. 16 Respiratory symptoms are known to occur in patients with obstruction; we are not aware of other studies associating the frequency of respiratory symptoms with the presence of restrictive ventilatory impairment.
In our study, the total number of symptoms in subjects with restrictive ventilatory impairment and COPD was low. Approximately one-third of the patients did not have symptoms and another third had only one symptom reported. The consideration here is that in general the cohort as a whole had mild to moderate degrees of impairment (post-BD FEV1% for restrictive group is 73.2% and for the obstructive group is 93%, and post-BD FEV1/FVC for the restrictive group is 0.79 and for the obstructive group is 0.67). The prevalence of reported symptoms may have appeared somewhat different in a patient population more skewed towards persons with more severe lung function impairment. A previous Spanish study showed that 84.1% of severe COPD patients presented one respiratory symptom. 17 In addition, our findings also showed that, as the number of respiratory symptoms increased, the proportion of patients decreased. Only 4% of patients had all four symptoms.
The most frequent symptoms reported by our subjects in both patient groups was dyspnea, followed by wheezing. Montes de Oca et al. 18 reported that in the general PLATINO study population, dyspnea, and wheezing were strongly associated with pulmonary exacerbations. Nascimento et al. 18 published results from the PLATINO study population from São Paulo indicating that dyspnea and wheezing were more frequent in diagnosed COPD than in undiagnosed subjects. In this study, the frequency of dyspnea was similar in persons with restrictive and obstructive spirometric impairments. However, the mechanisms underlying dyspnea in these patient groups likely differ. 19,20 The dyspnea in restrictive ventilatory impairment to decreased lung and/or chest wall compliance and increased elastic work of breathing rather than just to increased elastic recoil. 21,22
There was no statistical difference between frequency of respiratory symptoms in subjects with restrictive ventilatory impairment and COPD, with the exception of wheezing, which was more frequent only in mild restrictive impairment. It is difficult to explain the presence of wheezing in this population and why it was more prevalent only in those with mild restrictive impairment. While wheezing may have been referable to rhonchi or obstruction in the upper airways, it is not possible to draw firm conclusions regarding the wheezing in this patient group as this symptom was assessed by a questionnaire. However, in keeping with our results, Soriano et al. 3 recently also reported that wheezing was more frequent in individuals with restrictive ventilatory impairment than in COPD. Another study showed that wheezing was the second most prevalent symptom following dyspnea among patients with lung nodules 23 ; the authors did not discuss the mechanisms for this finding in the study. Although individuals with restrictive ventilatory impairment could be asthmatics and have wheezing, in our study, individuals with restrictive ventilatory impairment did not respond to BD, effectively ruling out asthma as a cause of the restriction. Notably, cough, sputum production, and dyspnea were present in both groups, and there were no statistical differences between them. This is somewhat surprising since some healthcare workers may not associate restrictive disease with cough and phlegm production.
Both groups in our study showed similar deterioration in quality of life, which was evaluated by physical and mental domains of SF-12 questionnaire. In general, patients with restrictive ventilatory impairment and COPD have similar physical limitation with decreased HRQL. 24,25
The overall prevalence of restrictive ventilatory impairment according to the LLN classification was 5.1%. Recently, Mannino et al. 4 reported a prevalence of restrictive disorder of 11.7% in males and 16.4% in females, although with high variability among countries participating in the Burden of Obstructive Lung Disease (BOLD) study. The EPI-SCAN study from Spain showed 12.7% of restrictive ventilatory impairment, with higher prevalence in Seville (19.4%) and the lower in Oviedo (5.2%). The BOLD and EPI-SCAN studies used a fixed ratio to diagnose restrictive ventilatory impairment, which could have underestimated its prevalence.
Obesity is associated with decreased pulmonary expansion and depending on the amount and distribution of body fat can lead to restrictive ventilatory impairments of varying degrees of severity. On the other hand, the abdominal circumference reflects the localized fat tissue and could better indicate its influence in lung function. 26 –29 Although the group of patients with restrictive impairment had a higher BMI than obstructed patients, the magnitude of the difference is not large enough to account for the differences observed. The obesity could have accounted for the restrictive ventilatory impairment on spirometry in at least some of the patients. The group of patients with restrictive impairment with higher BMI would probably present more symptoms compared with patients with restrictive impairment with normal BMI, however this would be a subject that merits further study, as this comparison was not part of our objectives.
Our results are relevant in that the presence of these symptoms and identification of a restrictive pattern by spirometry could help improve the medical approach for these individuals as was reported by Mannino et al., who showed that a restrictive ventilatory impairment has a higher association with diabetes, hypertension, and cardiovascular disease than individuals with normal lung function. This way, having a better knowledge of restrictive ventilatory impairment symptoms and its associations with other diseases, the patient’s clinical and pharmacological treatment could be optimized. An important limitation of our study was it did not identify the specific diseases related to restrictive ventilatory impairment, since the PLATINO study was not designed to evaluate possible etiologies of this condition. As such, it is not possible to determine the prevalence, type or patterns of symptoms among those whose restrictive ventilatory defect related to restrictive parenchymal lung disease versus restrictive chest wall disease versus obesity. This is an area that merits further study. Another limitation is the sole use of spirometry for the diagnosis of restrictive ventilatory impairment. We could not specify which were the diseases involved in the etiology of the restrictive ventilatory impairment since this was not part of the PLATINO study’s objectives. However, the fact that dyspnea was the most frequent symptom in this group allows us to infer that restrictive ventilatory impairment could be the cause for frequent respiratory discomfort and subject’s limitation during activities.
But PLATINO was a population-based epidemiological study and the spirometries were performed in the homes of the participants. But a reduced FVC has been associated with a reduced TLC, and it has been accepted as a surrogate marker for restriction in epidemiological studies. 3 Concerning the use of FEV1 to classify the restrictive impairment, the ATS/ERS 2005 document 6 suggests that FEV1 should be used in order to classify all ventilatory disturbances. In restrictive impairment the FVC/FEV1 ratio is normal or higher and there is good correlation between FVC and FEV1. 5 In this case, a moderate restrictive ventilatory disturbance is equivalent to a moderate obstructive disturbance. Another limitation of our study was the lack of available comparisons between our two patient groups and a healthy control group, however this was not an aim of this study. We do not consider it a significant limitation that individuals could attempt to reach technically adequate spirometry maneuvers up to 15 times. The technicians were highly trained to monitor any evidence of patient fatigue and were trained to take all the time necessary to reach the best performance from the individuals. This strategy has been published previously by Tálamo et al. 30 On the other hand our study has several strengths. First, we adopted the ATS/ERS 2005 criteria for the diagnosis of restrictive ventilatory impairment and airflow obstruction that takes into consideration the LLN. 6 The use of the fixed ratio FEV1/FVC does not take into consideration the influence of age, height, and gender in lung function, and values under 0.70 may be normal in elderly persons due to a decrease in elastic recoil. 5 According to Vaz Fragoso et al., 31 LLN had better association with risk of death and respiratory symptoms in patients with COPD than the fixed ratio criteria. The same association was shown for patients with restrictive ventilatory impairment. 32 Secondly, the design of the study limits selection bias and does provide information about the impact in the general population.
We conclude that the frequency of respiratory symptoms is similar among individuals with restrictive ventilatory impairment and COPD, which reinforces the importance of spirometry to differentiate these groups. Surprisingly, the prevalence of wheezing was higher in subjects with mild restrictive spirometrics pattern than in those with obstruction. The health status was equally affected in both groups. This study shows the need of future investigations evaluating the causes of restrictive ventilatory impairment.
Footnotes
Acknowledgements
Would like to acknowledge the hard work of all investigators and collaborators in each center.
Authors' notes
N.L.N. contributed to protocol design, data collection, analysis, and writing the manuscript. O.A.N., M.M.O., and A.M.B.M. contributed to protocol design and analysis. R.P.P. contributed to data collection and analysis. C.T., G.V., C.L., and M.V.L. contributed to data collection. B.C. contributed to data analysis and reviewed the text. J.R.J contributed to protocol design, analysis, and writing the manuscript.
Conflict of interest
We declare that none of the authors have any conflict of interest related to the topic of the article. In addition the authors do not have any association with the tobacco industry.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.