
Abstract
Objectives:
Pharmacologically mediated bronchodilation is important in the management of asthma, and is primarily achieved with β2-agonists. Novel compounds should preferably have a longer duration of action and a better systemic side effect profile than established alternatives at comparable peak bronchodilation. This single-dose crossover study was conducted to investigate and compare with formoterol the bronchodilatory and systemic effects, tolerability and safety of AZD3199, a novel ultra-long-acting β2-agonist (uLABA).
Methods:
Patients with asthma (n = 37) were randomized to receive AZD3199 (120, 480, 1920 µg), formoterol (9, 36 µg) or placebo inhaled via a Turbuhaler™. Bronchodilation was evaluated by maximum (Emax) and average 22–26 h (E22–26) forced expiratory volume in 1 second (FEV1). Serum potassium was evaluated by minimum (Emin) and 0–4 h average (Eav) determined from serial measurements. AZD3199 and formoterol were compared on the basis of relative dose potency. Adverse events, clinical laboratory tests and physical examinations were markers for safety and tolerability, with plasma AZD3199 as the indicator of drug exposure.
Results:
All active treatments dose-dependently increased Emax and AZD3199 (480 and 1920 µg) and formoterol (36 µg) significantly increased E22–26 versus placebo. Relative dose potency between AZD3199 and formoterol was 50-fold on the microgram scale with respect to Emax and 11-fold with respect to E22–26. Small, dose-dependent effects on potassium, heart rate and QTc were seen after administration of AZD3199 compared with placebo. These well-known dose-related class effects of β2-agonists were mild. Notably, serum potassium suppression was less pronounced after AZD3199 compared with formoterol at similar bronchodilation. Overall, AZD3199 was well tolerated.
Conclusions:
AZD3199 480 µg and 1920 µg produced 24-hour bronchodilation. At comparable peak bronchodilator effect, AZD3199 was associated with a lower level of systemic side effects than formoterol. AZD3199 was well tolerated, with no safety concerns identified to preclude further investigation.
ClinicalTrials.gov study identifier:
NCT00736489
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are characterized by airway obstruction and airflow limitation. Pharmacologically mediated bronchodilation is an important component of the management of these conditions and in asthma this is primarily achieved using β2-adrenoceptor agonists [Bateman, 2010]. Inhaled β2-agonists provide a faster onset of action and an improved therapeutic index, as compared with oral formulations [Lofdahl and Svedmyr, 1989]. In order to maintain a sustained therapeutic effect, however, inhaled β2-agonists should have a high affinity for airway tissue, or undergo slow release and absorption from the airway lumen, to allow retention of the drug in the lungs.
Formoterol and salmeterol are widely used β2-agonists and a high affinity for airway tissues is believed to be responsible for their bronchodilating effects, which last at least 12 hours [Anderson et al. 1994; Palmqvist et al. 1997]. New approaches to the management of asthma and COPD have focused on the development of once-daily, well-tolerated treatments. Novel compounds should have a systemic side-effect profile that is similar to, or better than, that of inhaled formoterol at comparable peak bronchodilating effects.
AZD3199, a benzothiazolone derivative, is a novel, selective, inhaled ultra-long-acting β2-agonist (uLABA), with a rapid onset of action that is not significantly different from that of formoterol, but is significantly faster than that of salmeterol, and has a significantly longer duration of action than both formoterol and salmeterol (see further review by Cazzola and colleagues [Cazzola et al. 2012]), characteristics that could potentially improve the pharmacological treatment of obstructive pulmonary diseases. AZD3199 has been investigated as a once-daily bronchodilator in COPD [Kuna et al. 2013]. The aim of the present study was to examine the bronchodilatory and systemic effects, tolerability and safety of AZD3199 in comparison with formoterol, both inhaled via Turbuhaler™, in patients with mild-to-moderate persistent asthma.
Materials and methods
Treatments and study design
This trial was a double-blind, placebo-controlled, randomized, six-way crossover single-dose study performed in patients with mild-to-moderate asthma at three centres in Sweden and one in Denmark.
Patients were randomized to receive AZD3199 (120, 480, 1920 µg), formoterol (9, 36 µg) or placebo, administered via a Turbuhaler™ (AstraZeneca) on six separate occasions. The Turbuhaler™ delivered doses of AZD3199 120 μg (2 × 60 μg per puff), 480 μg (2 × 240 μg per puff) and 1920 µg (8 × 240 μg per puff) were estimated to equate to 48, 192 and 768 µg lung deposited doses, based on the analysis of fine particles generated in vitro, using a computational model for extra-thoracic deposition from dry powder inhalers [DeHaan and Finlay, 2004] i.e. 40% of delivered doses. If required, Bricanyl® Turbuhaler™ (0.25 mg/inhalation) could be used as rescue medication during the clinic visits.
Objectives
The primary objective of the study was to investigate the pharmacodynamics of inhaled AZD3199 in comparison with formoterol and placebo, with assessments of forced expiratory volume in 1 second (FEV1) and serum potassium levels.
Serial FEV1 measurements were performed in duplicates at −30 and −15 minutes predose and then at 5, 15, 30 and 60 minutes and 2, 4, 6, 8, 10, 12, 14, 18, 22, 24 and 26 hours postdose. The magnitude of bronchodilatation, assessed as maximum FEV1 (Emax) and duration of action, assessed as the residual effect on FEV1 at 22–26 hours postdose (E22–26) constituted the primary basis for evaluation of efficacy. In addition, average effects on FEV1 over 24 hours (Eav), over the first 12 hours (E0–12) and from 12–24 hours were examined, with FEV1 at 5 minutes (E5 min) as a measure of the onset of action.
Blood sampling for serum potassium was performed predose and then at 15, 30, 60 minutes, 2, 4, 8, 12 and 24 hours postdose. Magnitude of serum potassium suppression, assessed as minimum serum (Emin) and 0–4 hours postdose average (Eav) constituted the primary basis for evaluation of systemically mediated effect. Heart rate, QTcB, pulse, blood pressure, tremor and palpitations were similarly assessed as secondary variables for systemically mediated effects.
The safety and tolerability of AZD3199 were assessed on the basis of incidence and nature of adverse events, clinical laboratory assessments and physical examination, as a secondary objective of the study.
Drug exposure of AZD3199 was investigated by assessment of drug concentration in plasma and calculated pharmacokinetic (PK) parameters.
Inclusion and exclusion criteria
Patients were male or postmenopausal females aged ≥18 years with a minimum 6-month history of asthma. Those taking inhaled steroids prior to enrolment were allowed to continue taking them during the study period, provided that the dose was maintained at a constant level. Use of inhaled short-acting bronchodilators was permitted, except for the period prior to inhalation of study drug (≤8 h for β2-agonist and ≤ 12 h for anticholinergic). Long-acting β2-agonist bronchodilators were not allowed from 72 h prior to first spirometry and throughout the study period and long-acting muscarinic antagonist bronchodilators were not allowed from 48 h prior to first spirometry and throughout the study period. Patients were to be nonsmokers or exsmokers, with a prebronchodilator FEV1 ≥60% predicted normal and ≥1.5 l. A small number of users of tobacco snuff were included in the study. Airway obstruction with a confirmed stepwise reversibility to salbutamol was also required for study inclusion. For the stepwise reversibility test, patients received 100 µg salbutamol, followed by an FEV1 recording after 15–30 minutes. Patients then received an additional dose of 900 µg salbutamol, with FEV1 again recorded after 15–30 minutes. An increase in FEV1 ≥5% between the first and second dose of salbutamol and a total increase of ≥15% relative to baseline after the two doses of salbutamol was required for a patient to fulfil the inclusion criteria.
Patients with any clinically significant disease or disorder were excluded from the study. A history of ischaemic heart disease or failure, a QTcF interval >450 ms, a QT interval >500 ms or any other ECG abnormalities were other reasons for exclusion. Patients who had received systemic glucocorticoid treatment within the 30 days prior to the study, or who had donated blood or plasma within 3 months or 14 days respectively prior to the first study visit, were also excluded from study participation.
Statistical analysis
Bronchodilator and systemic effects were compared between treatments using analysis of variance models, with fixed factors for treatment, period and patient, using the predose value of FEV1 (mean of the two predose values) as a covariate. Pairwise treatment contrasts were constructed between doses of AZD3199, formoterol and placebo. A closed testing procedure, starting at the top dose, was used when testing for efficacy versus placebo. The relative dose potency between the two treatments was estimated assuming parallel lines for lung function and shifted sigmoidal curves for systemic effects. Onset times were compared using a Cox proportional hazards model with treatment as factor and stratified by patient.
Ethics
The clinical study was approved by the Independent Ethics Committee in each participating country. The study was performed in accordance with the ethical principles that have their origin in the Declaration of Helsinki and that are consistent with International Conference on Harmonization (ICH)/Good Clinical Practice (GCP) and applicable regulatory requirements and the AstraZeneca policy on Bioethics. Informed consent was obtained from all subjects prior to initiation of any study specific procedures.
Results
Of the 73 patients enrolled in the study, 37 were randomized to treatment. The demographic and baseline characteristics of patients are outlined in Table 1. The average patient age was 40.3 years (range 22–68); 32/37 were male and 35/37 were white. Only four patients (11%) were current users of tobacco snuff and none had smoked in the 6 months prior to enrolment or had a smoking history of more than 15 pack-years. Patients had a median time since asthma diagnosis of 25.2 years (range 2–58). Mean prebronchodilator FEV1 at entry to the study was 3.1 l, corresponding to 77% predicted normal. Mean stepwise reversibility in FEV1 in response to salbutamol was 24%.
Summary of demographic and disease-related data at entry.
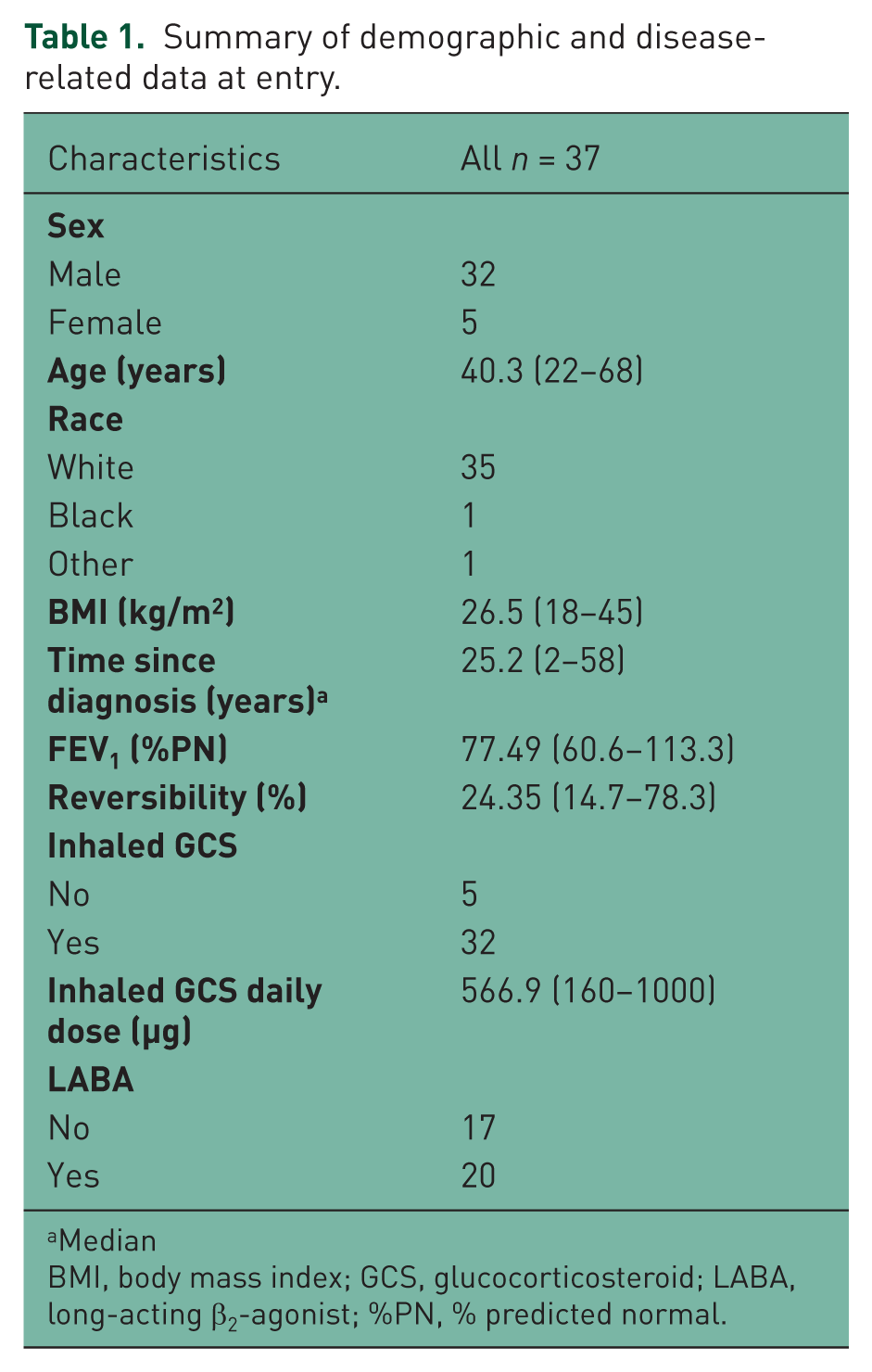
Median
BMI, body mass index; GCS, glucocorticosteroid; LABA, long-acting β2-agonist; %PN, % predicted normal.
Bronchodilation and rescue medication
A dose-dependent and statistically significant effect on peak FEV1 was observed with all active treatments in comparison with placebo (all p < 0.01; see Figure 1 and Table 2). Statistically significant effects were also observed on Eav, E0–12, E12–24 and E5min for all doses of AZD3199 and formoterol versus placebo (all p < 0.05; see Table 2). The estimated relative dose potency for peak bronchodilation between treatments was 50-fold on the microgram scale.

Mean changes in forced expiratory volume in 1 second (FEV1) following administration of AZD3199 (120, 480, 1920 µg), formoterol (9, 36 µg) or placebo in patients with mild-to-moderate persistent asthma.
Treatment estimates and pairwise contrasts for FEV1: Emax, Eav, E0–12, E12–14, E5min and E22–26.

CI, confidence interval; FEV1, forced expiratory volume in 1 second.
Dose-dependent and statistically significant effects on E22–26 (all p < 0.001; see Table 2), were observed after AZD3199 (480 and 1920 µg) and formoterol (36 µg), but not after the lowest dose of each active compound. The estimated relative dose potency for E22–26 was 11-fold on the microgram scale, approximately 5 times smaller than based on peak bronchodilation.
An early statistically significant effect on FEV1 (E5min) was seen after AZD3199 and formoterol. However, in contrast to the effect of formoterol, that of AZD3199 was not dose dependent. Therefore, no firm conclusion could be drawn regarding the relative onset properties.
The most frequent use of rescue medication was reported in patients receiving placebo treatment (10 patients, 41 doses), with the least frequent use of rescue medication following treatment with AZD3199 480 µg (four patients, seven doses) and AZD3199 1920 µg (four patients, nine doses).
Systemic effects
Statistically significant systemic effects were only seen after formoterol 36 μg and AZD3199 1920 μg. On serum potassium and tremor formoterol gave the largest effects, whereas on heart rate and QTcB effects were of similar magnitude (Figure 2 and Tables 3 and 4). Overall, at comparable peak effects on FEV1, AZD3199 was shown to have a more favourable profile than formoterol with regard to systemic effects.

Mean change in serum potassium during the first 4 hours after drug administration.
Treatment estimates and pairwise contrasts for average (Eav) effects on serum potassium, heart rate, QTcB, pulse, blood pressure, tremor and palpitations.

CI, confidence interval.
Treatment estimates and pairwise contrasts for maximum (Emax) effects on heart rate, QTcB, pulse, tremor and palpitations, and minimum (Emin) effects on potassium and blood pressure.

CI, confidence interval.
Safety
AZD3199 was well tolerated, with no deaths, serious adverse events, discontinuations due to adverse events or other significant adverse events. The most frequently reported adverse events were headache and nasopharyngitis. Adverse events were more frequently reported following AZD3199 1920 µg, with four patients reporting throat irritation at this dose only.
Discussion
The aim of the present study was to investigate the pharmacodynamics of AZD3199, in comparison with formoterol, to aid the selection of appropriate doses of AZD3199 for further phase II studies. The dose range was selected on the basis of the results of a single-ascending dose (SAD) study. A fourfold difference between doses was aimed for, to optimize the possibility of seeing dose-dependent effects. The minimum inhaled dose of 120 µg was selected to be on the lower limit of an effective dose, whereas the intermediate dose of 480 µg was expected to give a 24-hour duration of bronchodilatory effect. The maximum dose of 1920 µg was selected to provide a margin below the mean maximum exposure observed in the SAD study. Patients with asthma were selected for the study population as they are considered to be the most sensitive group of patients to β2-agonist treatment, and because dose–response to a β2-agonist can be assessed following temporary withdrawal of bronchodilator therapy in these patients.
All doses of AZD3199 and formoterol significantly and dose-dependently increased peak FEV1 relative to placebo. AZD3199 480 and 1920 µg and formoterol 36 µg maintained bronchodilation for 24 hours, with a significant difference in comparison with placebo for E22–26. The estimated relative dose potency between AZD3199 and formoterol on the microgram scale was 50-fold with respect to maximal bronchodilation, suggesting equal potency between AZD3199 480 µg and formoterol 9 µg. With respect to residual bronchodilation at 22–26 hours postdose, the relative dose potency between AZD3199 and formoterol was 11-fold on the microgram scale, indicating a prolonged duration of bronchodilation with AZD3199. This is supported by the less frequent use of rescue medication following AZD3199 480 and 1920 µg treatment in comparison with formoterol. All active substances produced a statistically significant effect at 5 minutes postdose, but the early response of AZD3199 was not dose-dependent, in contrast to formoterol. As such, no firm conclusions can be drawn regarding the relative onset properties between AZD3199 and formoterol.
Statistically significant systemic effects were observed only following treatment with formoterol 36 µg and AZD3199 1920 µg. Formoterol had a greater effect on serum potassium levels and tremor scores, whereas AZD3199 and formoterol had comparable effects on heart rate and QTcB. Overall, at doses with comparable effects on peak FEV1, AZD3199 was associated with a lower level of systemically mediated effects in comparison with formoterol, suggesting a more favourable therapeutic index.
AZD3199 was demonstrated to be well tolerated in these patients with asthma at the studied dose range. Adverse events were more frequently reported following treatment with AZD3199 1920 µg, with throat irritation reported only at this highest dose. This reaction started soon after dosing and may, therefore, be related to the large quantity of drug administered at this dose level. No serious adverse events or discontinuations due to adverse events were reported, and no safety concerns were identified for AZD3199.
Conclusions
AZD3199 produced effective bronchodilation over 24 hours at doses of 480 and 1920 µg. The data suggest that AZD3199 can achieve a peak bronchodilatory effect that is comparable with formoterol, but with a longer duration and a lower level of systemic side effects. No safety concerns were identified that could preclude AZD3199 entering further clinical trials.
Footnotes
Acknowledgements
The authors thank Dr Kim Krogsgaard for participating in the conduct of this study. The authors thank David Candlish and Natasha Hausman of inScience Communications, Springer Healthcare, for medical writing assistance funded by AstraZeneca. Turbuhaler™ is a trademark of the AstraZeneca group of companies. Turbuhaler™ is a registered trademark in Sweden and Denmark where the studies were performed.
Funding
This study was supported by AstraZeneca.
Conflict of interest statement
LB has received honoraria for speaking and consulting and/or financial support for attending meetings from Almirall, AstraZeneca, Airsonett, Andre Pharma, Boehringer, GlaxoSmithKline, Merck, Mundipharma, Nigard, Novartis, Nycomed/Takeda and Orion Pharma. JR is an employee of AstraZeneca plc and holds shares in the company. TB was an employee of AstraZeneca at the time this study was carried out and holds shares in the company. JL has received honoraria for speaking and consulting and/or financial support for research from AstraZeneca, Airsonett, GlaxoSmithKline, Merck/MSD and Novartis.