
Abstract
Objectives:
Physical activity, sedentary and sleep behaviours have strong associations with health. This systematic review aimed to identify how clinical practice guidelines (CPGs) for the management of chronic obstructive pulmonary disease (COPD) report specific recommendations and strategies for these movement behaviours.
Methods:
A systematic search of databases (Medline, Scopus, CiNAHL, EMbase, Clinical Guideline), reference lists and websites identified current versions of CPGs published since 2005. Specific recommendations and strategies concerning physical activity, sedentary behaviour and sleep were extracted verbatim. The proportions of CPGs providing specific recommendations and strategies were reported.
Results:
From 2370 citations identified, 35 CPGs were eligible for inclusion. Of these, 21 (60%) provided specific recommendations for physical activity, while none provided specific recommendations for sedentary behaviour or sleep. The most commonly suggested strategies to improve movement behaviours were encouragement from a healthcare provider (physical activity n = 20; sedentary behaviour n = 2) and referral for a diagnostic sleep study (sleep n = 4).
Conclusion:
Since optimal physical activity, sedentary behaviour and sleep durations and patterns are likely to be associated with mitigating the effects of COPD, as well as with general health and well-being, there is a need for further COPD-specific research, consensus and incorporation of recommendations and strategies into CPGs.
Keywords
Background
Throughout the day, people engage in a range of activities: sleep, leisure, occupational, transport, self-care or household chores. 1 Activities can be categorized into different movement behaviours according to their energy requirement in metabolic equivalents (METs). While the energy requirement of sleeping is around 0.9 METs, the energy requirement of waking activities ranges from 1.0 MET for quiet sitting to >20 METs for athletic activities. Waking activities that are on the lower end of the energy expenditure spectrum (1.0–1.5 METs) and maintain a seated or reclined posture are considered sedentary behaviours. 1,2 In contrast, physical activities are bodily movements produced by skeletal muscles that result in energy expenditure and can be of light- (1.6–2.9 METs), moderate- (3–5.9 METs) or vigorous-intensity (≥6 METs). 1,3
Different movement behaviours have significant associations with either positive or negative health outcomes. 4 –6 Public health guidelines have been developed to provide the general population with specific recommendations for movement behaviours and strategies to facilitate changes in movement behaviours, to improve and maintain health. 7 –9
For the general population, 150 minutes of at least moderate intensity (≥3 METs) physical activity per week is recommended for significant health benefits; 8 however, for people with chronic obstructive pulmonary disease (COPD), replacing time spent in sedentary behaviour with light intensity physical activities may be a more feasible goal. 10 Reducing time spent in sedentary behaviour has demonstrated positive associations with waist circumference and glucose level, 11 while participation in regular physical activity has shown associations with reduced risk of all cause and respiratory mortality and acute COPD exacerbation. 12 Spending more time in active pursuits may also help to improve sleep quality. 13 Sleep quality has shown to be a predictor of mortality, COPD-hospitalization, health-related quality of life and severity of day time symptoms. 14 –16
Public health guidelines developed for the general population recommend people who have chronic conditions seek advice from health care providers to adequately manage their condition. 8 To assist with the management of chronic conditions such as COPD, clinical practice guidelines (CPGs) have been developed. 17,18 This systematic review posed two primary questions:
In CPGs for the management of COPD: What specific recommendations are provided for physical activity, sedentary behaviour and sleep? What strategies are provided to achieve optimal amounts of physical activity, sedentary behaviour and sleep?
Secondary questions concerned how specific recommendations and strategies for movement behaviours were presented within CPGs.
Methods
The protocol for this systematic review was developed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA-P 2015) guidelines. 19
Eligibility
CPGs were included in this review if they were the most recent version for the broader management of COPD developed by an authoritative body and published since 2005. No limitations were set for language of publication. References were excluded if they were experimental or observational designs, systematic or narrative reviews, conference abstracts, opinion pieces or focused specifically on pharmacological management, management of acute exacerbations, pulmonary rehabilitation or domiciliary oxygen.
Information sources and search strategy
A range of electronic databases were searched: OVID Medline, EMbase, CiNAHL and Scopus. Search terms were collated for the population of interest (COPD) and the publication type (clinical practice guideline). The first group of search terms included COPD, pulmonary emphysema and pulmonary disease chronic obstructive. The second group of search terms included guideline, consensus, position statement, guidance and standard. All items within a group were separated by the Boolean term ‘OR’ and groups were separated by the Boolean word ‘AND’. The complete search strategy conducted in OVID Medline is presented in Table S1 of the online supplementary materials. Clinical guideline databases were also searched for eligible guidelines and included: The National Institute for Health and Care Excellence, Clinical Practice Guidelines Portal, National Guideline Clearing House, International Guideline Network, Scottish Intercollegiate Guidelines Network and the International Primary Care Respiratory Group. To identify any additional guidelines, the reference lists of systematic reviews identified from the search and websites of the medical and scientific bodies listed as participating at the European Respiratory Society International Congress for 2016 were screened. An expert in the field was consulted to ensure that no known CPGs were missed in the search process.
Document selection
The complete lists of titles retained from the searches were screened (HL). Where eligibility was unclear from the title or abstract, the full text was reviewed by two independent reviewers and assessed against eligibility criteria (HL, MTW). For all titles and/or abstracts that were not published in English, the full texts were obtained. A single reviewer (HL) assisted a fluent speaker of the language to assess non-English texts against eligibility criteria.
Data collection
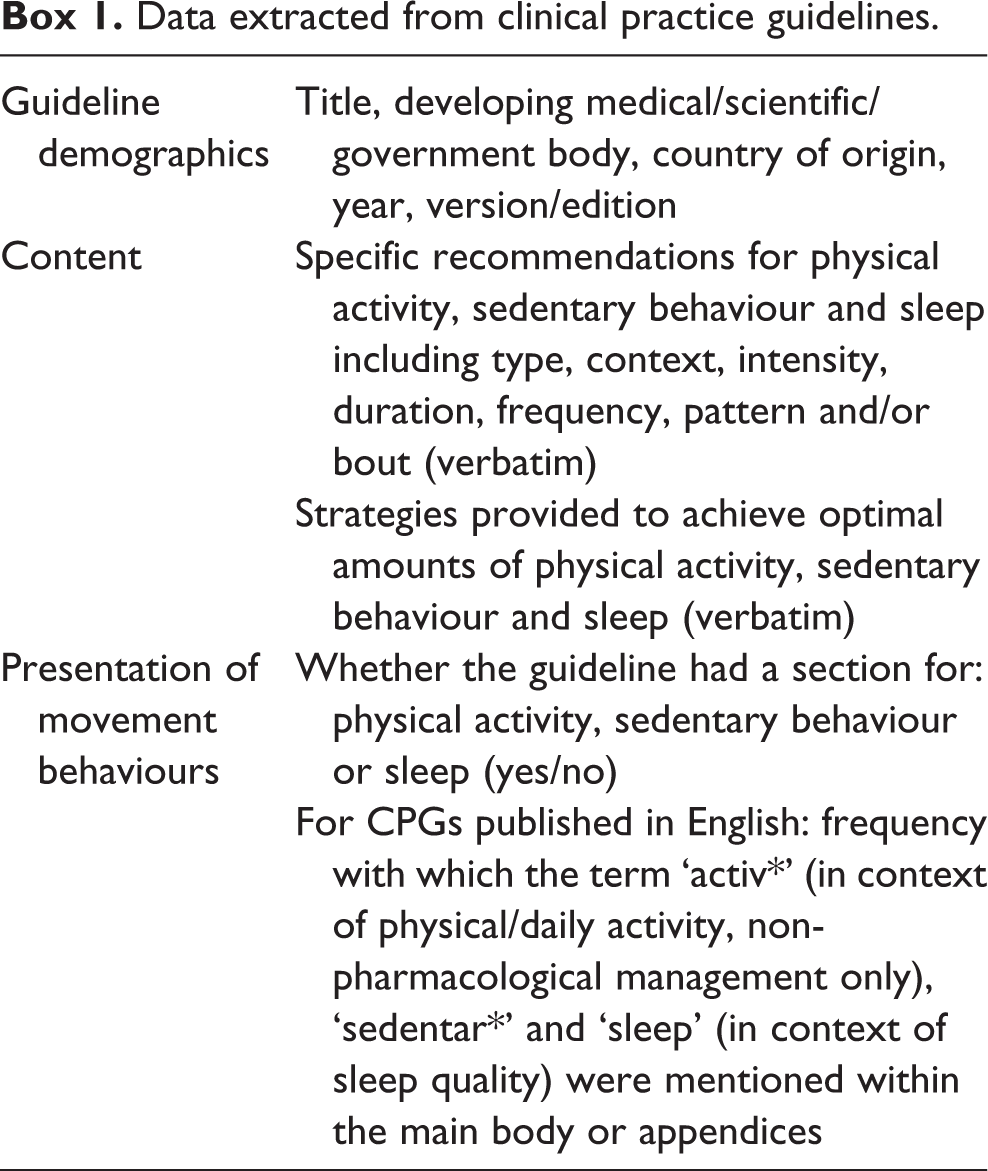
A data extraction template was developed a priori. For eligible CPGs published in English, three reviewers (HL, MTW and TWE) extracted data independently; data were then compared and discussed until consensus was met. For eligible CPGs not published in English, a single reviewer (HL) assisted a fluent speaker of the language to extract data. Data extracted from CPGs are described in Box 1. Where data were extracted regarding specific recommendations and strategies, the following definitions were applied:
Specific recommendation: Where a target type, context, intensity, frequency, duration, pattern and/or bout of a movement behaviour was reported/stated.
Data extracted from clinical practice guidelines.
Specific recommendations for physical activity within COPD CPGs.

COPD: chronic obstructive pulmonary disease; CPGs: clinical practice guidelines; 6MWT: six minute walk test; VO2 max: maximal oxygen uptake. For explanation of CPG abbreviation see Table S2 of the online supplementary materials.
Strategy: Where a method, intervention or process was reported/stated as a means of changing a movement behaviour.
Data analysis
All data extracted were collated and summarized descriptively for specific recommendations or strategies according to movement behaviour type. The proportion of CPGs providing specific recommendations and strategies for each movement behaviour was reported. Specific recommendations and strategies around movement behaviours were compared for commonalities across guidelines. How movement behaviours were presented within CPGs was reported descriptively.
Results
The initial search of four electronic databases obtained 2370 citations, 17 of which were eligible for inclusion. A further 22 citations were identified through supplemental search approaches. No additional guidelines were identified or removed following consultation with the content expert. Despite meeting eligibility criteria for inclusion, one CPG was excluded as the full text was unable to be translated from Ukrainian, 20 and three were excluded as the full texts were unable to be obtained (not being available for purchase outside of the United States of America 21 and Japan 22 and prohibitive costs 23 ). Therefore, 35 CPGs were included in this review (Figure 1).

Outcome of search strategy leading to clinical practice guidelines for the management of COPD eligible for this review. COPD: chronic obstructive pulmonary disease
Physical activity
There were 21 (60%) CPGs included in this review, which provided specific recommendations for physical activity (target: type n = 7, 20%; context n = 4, 11%; intensity n = 6, 17%; duration n = 6, 17%; frequency n = 19, 54%; Table 1). Walking was the most commonly recommended type of physical activity (n = 4, 11%), followed by cycling (n = 3, 9%), strength training (n = 3, 9%) and non-specific aerobic training (n = 3, 9%). Four (11%) guidelines recommended a context for which physical activity is to be performed; as part of the person’s lifestyle and social life, 46 in a group 47 or in recreational clubs, 48 at home 49 or independently. 48 Four of the six guidelines, which provided specific recommendations for intensity of physical activity, recommended people with COPD to be active as per their capacity or until breathless. 48,50 –52 The six guidelines including a target duration of physical activity, recommended durations ranging from 20 minutes to 45 minutes per day. One guideline provided a specific target duration for people with more severe COPD, recommending short intervals rather than continuous activity. 53 Specific recommendations for a target frequency ranged from once a week (n = 1, 3%) to daily (n = 6, 17%) or regularly (n = 8, 23%; Table 1). Three guidelines recommended regular supervision. 47,48,54
There were 28 (80%) CPGs that provided strategies to achieve improvements in physical activity. Encouragement from a health care provider was the most commonly suggested strategy (n = 20, 57%) followed by education (n = 11, 31%), long-term management (n = 6, 17%) and referral to an exercise training program (n = 6, 17%) (Table 2).
Non-pharmacological strategies to achieve optimal amounts of physical activity for people with COPD included in CPGs.

COPD: chronic obstructive pulmonary disease; CPGs: clinical practice guidelines; EP: exercise physiologist; mgmt:– management; OT: occupational therapy; PR: pulmonary rehabilitation
aOxygen recommended on exertion for those patients who meet specific recommendations for hypoxia. For explanation of CPG abbreviation see Table S2 of the online supplementary materials.
Note: Shading indicates that the corresponding strategy was provided in the CPG.
Non-pharmacological strategies to achieve optimal amounts of sedentary and sleep behaviours for people with COPD within CPGs.

COPD: chronic obstructive pulmonary disease; CPGs: clinical practice guidelines; NIV: non-invasive ventilation; COPD-X: Australian and New Zealand online management guidelines for Chronic Obstructive Pulmonary Disease; AIMAR: Interdisciplinary Association for Research in Lung Disease; SEPAR: Spanish Society of Pneumology and Thoracic Surgery; VA/DoD: Department of Veterans Affairs/Department of Defense; STS: Specialized Technical Services; SGP: Swiss Respiratory Society; CPFS: Czech Pneumological and Phthisiological Society; ICS/NCCP: The Indian Chest Society/National College of Chest Physicians; ATS/ERS: American Thoracic Society/European Respiratory Society; SATS: South African Theological Seminary; NICE: National Institute for Health and Care Excellence; MOH: Ministry of Health; IPCRG: The International Primary Care Respiratory Group
aNocturnal oxygen is recommended for those patients who meet specific guidelines for long-term domiciliary oxygen therapy
Guidelines were similar in reporting specific recommendations and strategies for physical activity whether published in English (specific recommendations n = 10, 50%; strategies n = 17, 85%) or a language other than English (specific recommendations n = 11, 73%; strategies n = 12, 80%).
Three guidelines (9%) had a dedicated section for physical activity (Table 4). Of the guidelines published in English, the term ‘activ*’ was most frequently mentioned in the guidelines from Australia and New Zealand (n = 29), GOLD (n = 24) and Spain (n = 21). The terms pertaining to physical activity were mentioned more frequently in the CPGs published in 2014 or later.
Sedentary behaviour
No CPG provided specific recommendations for sedentary behaviour.
Three (9%) CPGs provided strategies to reduce time spent in sedentary behaviour. Encouragement from a health care provider was suggested by two guidelines, and inclusion of practicing sit-to-stand transitions in exercise training was suggested by a single guideline (Table 3). Of the 15 non-English guidelines included in this review, only one provided strategies to reduce time spent in sedentary behaviour, 69 which differed from those provided in English guidelines.
Format and frequency of recommendations and strategies for physical activity, sedentary behaviour and sleep within English CPGs.

CPGs: clinical practice guidelines; GOLD: Global Initiative for Chronic Obstructive Lung Disease; COPD-X: Australian and New Zealand online management guidelines for Chronic Obstructive Pulmonary Disease; AIMAR: Interdisciplinary Association for Research in Lung Disease; SEPAR: Spanish Society of Pneumology and Thoracic Surgery; VA/DoD: Department of Veterans Affairs/Department of Defense; STS: Specialized Technical Services; SGP: Swiss Respiratory Society; CPFS: Czech Pneumological and Phthisiological Society; ICS/NCCP: The Indian Chest Society/National College of Chest Physicians; ATS/ERS: American Thoracic Society/European Respiratory Society; SATS: South African Theological Seminary; NICE: National Institute for Health and Care Excellence; MOH: Ministry of Health; IPCRG: The International Primary Care Respiratory Group
aactiv = physical/daily activity in context of non-pharmacological management.
bsedentar = sedentary/sedentarism.
csleep = in context of sleep quality.
No guideline had a dedicated section for sedentary behaviour (Table 4). Of the guidelines published in English, the term ‘sedentar*’ was most frequently mentioned in the guidelines from Australia and New Zealand (n = 4), with the guidelines from Spain and Italy both mentioning the term once each.
Sleep
No CPG provided specific recommendations for sleep.
Five (14%) CPGs provided strategies to improve sleep. Referral for a diagnostic sleep study (n = 4, 11%) or to a sleep specialist (n = 2, 6%) were the most commonly suggested strategies (Table 3). All guidelines providing strategies to improve sleep were published in English.
Three guidelines (9%) had dedicated sections for sleep (Table 4). Of the guidelines published in English, the term ‘sleep’ was most frequent in the guidelines from Australia and New Zealand (n = 16), Saudi Arabia (n = 11), Russia (n = 7) and the Institute for Clinical Systems Improvement (n = 6). The term ‘sleep’ was not mentioned in six guidelines. 52,70 –74
Discussion
CPGs have been developed to inform clinicians and healthcare professionals of best practice based on available evidence. 17,18 For the management of COPD, a number of CPGs have been developed. The majority (n = 28, 80%) of CPGs included in this review, provided strategies to achieve sufficient physical activity; however, few (n = 2, 6%) provided specific recommendations that included a target type, context, intensity, duration and frequency of physical activity. No CPG provided specific recommendations for sedentary behaviour or sleep, and few suggested strategies to achieve improvements in these domains.
Specific recommendations and strategies concerning physical activity, sedentary or sleep behaviours were difficult to find within most CPGs. Only three (9%) guidelines had a dedicated section for physical activity or sleep, and no guideline had a dedicated section for sedentary behaviour.
The limited specific recommendations and strategies around movement behaviours, particularly around sedentary and sleep behaviours, may be a result of two factors: (1) lack of available evidence to support COPD-specific recommendations and strategies and (2) an assumption that improving physical activity will consequently improve sedentary and sleep behaviours.
Lack of available evidence to support COPD-specific recommendations
Since the early 2000s, there have been a number of studies reporting associations between the level of physical activity and important COPD-specific health outcomes, including risk of mortality and acute COPD exacerbation. 12 Consequently, there has been an emergence of experimental studies exploring the effects of different intervention modalities on increasing physical activity levels in the COPD population; 75 the available evidence supporting efficacious strategies to increase physical activity levels for people with COPD is however inconsistent and of average quality. 12,75
In contrast, there are few studies that explore relationships between volumes, patterns and bouts of sedentary behaviour and COPD-specific health outcomes. 11 A simple search for studies exploring the effects of interventions specifically targeting time spent in sedentary behaviour identified a single protocol. 76 Similarly, while poor sleep quality is commonly reported by people with COPD 15,77 and has demonstrated associations with adverse physiological and psychological health outcomes, 14 –16 few studies have explored therapeutic interventions to improve sleep in people with COPD without a coexisting sleep disorder. 78 –81
In the adult general population, more time spent in light intensity physical activity than sedentary behaviour, 4 –6 breaking up sedentary time more frequently, 82 and sleep durations between 7 hours and 9 hours 7 have demonstrated associations with favourable health outcomes; while prolonged periods of sedentary behaviour have demonstrated associations with deleterious health outcomes. 83 Given that people with COPD spend a large proportion of the waking day in sedentary behaviour and have reduced night-time sleep durations, 84 at a minimum these recommendations could be provided within CPGs for the management of COPD. Due to clinical and functional characteristics (lung hyperinflation, dyspnoea, fatigue, skeletal muscle dysfunction and acute exacerbations), 12,85,86 changing time spent in sedentary and sleep behaviours may be more feasible in the COPD population, as opposed to changing time spent physically active. 10,87
An assumption that improving physical activity will consequently improve sedentary and sleep behaviours
The emergence of research focused on physical activity in the COPD population, may be due to assumptions that improving physical activity will in turn improve sedentary and sleep behaviours. However, evidence for effects of physical activity interventions on time spent in sedentary behaviour in the general population does not support this assumption. 88,89 Recent meta-analyses of interventions to reduce sedentary behaviour in the general population demonstrate that while interventions targeting sedentary behaviour produced clinically significant reductions in total sedentary time, interventions targeting physical activity produced little or no effect in reducing total sedentary time. 88,89 For those people who increase time spent in moderate-to-vigorous intensity physical activity (≥3METs) to meet public health recommendations (≥150 min/week 8 ), this time would still only comprise 2–3% of the 24-hour day. Some confusion has arisen around the term ‘inactivity’, which refers to being insufficiently active (i.e. failing to meet physical activity guidelines). ‘Inactive’ does not refer to levels of sedentary behaviour; one can be active (i.e. meet the physical activity guidelines) but still have undesirably high levels of sedentary behaviour.
Strengths and limitations
One strength of this review is the comprehensive search strategy used. In addition to electronic databases, clinical guideline databases, reference lists of systematic reviews and websites of authoritative bodies within the field were searched.
This review was strengthened by not setting limitations for publication language. The inclusion of non-English CPGs (n = 15, 43%) ensured that differences around specific recommendations and strategies for movement behaviours across countries were captured.
Conclusion
There were a number of CPGs for the management of COPD to provide specific recommendations and strategies around physical activity; however, no guideline provided specific recommendations for sedentary behaviour or sleep, and few provided strategies to achieve improvements in either of these domains. COPD-specific clinical characteristics and comorbidities likely pose additional barriers to achieving general population recommendations for physical activity for people with COPD. However, so far, there is no reason to assume that patterns and bouts of sedentary and sleep behaviours recommended for the general population differ to what would be required in the COPD population to improve health. People with COPD spend a large proportion of the day in sedentary behaviours and have reduced night-time sleep durations. Therefore, at a minimum, specific recommendations focused on changing time spent in sedentary and sleep behaviours could be provided within CPG for the management of COPD to achieve significant health benefits. To facilitate integration into clinical practice, recommendations and strategies around movement behaviours should be explicitly stated within CPGs.
Footnotes
Supplemental material
Supplementary material is available for this article online.
Acknowledgements
The authors would like to thank the following people for assisting with the translation of clinical practice guidelines included in this review: Professor Esther May (Division of Health Sciences, University of South Australia), Dr Hanna Tervonen (School of Health Sciences, Division of Health Sciences, University of South Australia), Dr Dorota Zarnowiecki (School of Health Sciences, Division of Health Sciences, University of South Australia), Diana Knudsen (School of Pharmacy and Medical Sciences, Division of Health Sciences, University of South Australia), Bjorn Dueholm (School of Pharmacy and Medical Sciences, Division of Health Sciences, University of South Australia). We would also like to thank academic librarian Sarah McQuillen (Academic Library Services, University Library, University of South Australia) for providing advice on the search strategy and Professor Peter Frith (School of Health Sciences, Division of Health Sciences, University of South Australia) for providing his expertise on the final list of clinical practice guidelines to be included in this review.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HL and TWE have nothing to disclose. MTW reports grants from National Health and Medical Research Council and travel and honorarium from Boehringer Ingelheim and the Australian Physiotherapy Association, outside the submitted work. TO reports grants from Pennington Biomedical Research Center, National Health and Medical Research Council, and Australian Research Council, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.