
Abstract
Pulmonary rehabilitation programs (PRPs) are most commonly provided in hospital settings which present barriers to attendance such as long distances or travel times. Community-based settings have been used in an attempt to alleviate the travel burden. This study evaluated the feasibility and outcomes of a network of community-based PRPs provided in non-healthcare facilities (CPRPs). The CPRPs were established in five venues and comprised two supervised group sessions each week for 8 weeks. Participant inclusion criteria and guidelines for exercise testing and training were developed to reduce the risk of adverse events. Outcome measures included 6-min walk distance (6MWD) and health-related quality of life (chronic respiratory questionnaire (CRQ)). Respiratory-related hospital admission data were collected in the 12 months prior to and following the program. Two hundred and fifty-one participants (79% with chronic obstructive pulmonary disease: mean ± SD FEV1 49 ± 21%predicted) entered a CPRP of which 166 (66%) completed. Improvements were demonstrated in 6MWD (mean difference (95% CI) 44 m (37–52)) and total CRQ score (0.5 points per item (0.4–0.7)). Fewer participants had a respiratory-related hospital admission following the program (12% vs. 37%, p < 0.0001). Pulmonary rehabilitation is safe, feasible and effective when conducted in community-based non-healthcare facilities.
Introduction
Compelling evidence exists for the benefits of pulmonary rehabilitation in people with chronic respiratory disease (CRD) and in particular for those with chronic obstructive pulmonary disease (COPD). 1,2 The benefits include improved symptoms (dyspnoea and fatigue), exercise capacity, health-related quality of life (HRQoL) and mood, and a reduction in healthcare utilization. 1 Despite these benefits some people with COPD who are referred never attend pulmonary rehabilitation programs (PRPs) and rates of 10–32% have been reported for non-completion. 3 A number of factors have been identified that contribute to poor uptake and completion rates including transport and location barriers with patients less likely to complete a PRP if they have a long journey time 4 and/or live a large distance from the centre. 5 Illness and comorbidities are also common reasons for non-completion. 3
Traditionally, PRPs have been provided in hospital outpatient or inpatient settings. However, these programs may have limited availability due to the high costs, or funding and referral restrictions. Further, access to these PRPs can be difficult due to lack of transport for people who live long distances from the hospital and the cost of parking may influence attendance. For a PRP based in a hospital outpatient physiotherapy department, we previously reported program uptake and completion rates of 49% and 73%, respectively, with transport difficulties and medical problems being important barriers to attendance. 6,7
Offering a PRP in a community-based non-healthcare setting may be a strategy to increase availability and alleviate the travel burden, and thereby improve uptake and completion. However, it is unclear whether the benefits gained in hospital-based PRPs are achieved in community-based programs. A subgroup analysis of hospital versus community-based programs in the Cochrane review of pulmonary rehabilitation for COPD 2 identified a treatment effect in favour of hospital-based programs. However, this finding should be interpreted with caution because four of the nine community-based PRPs were provided in the home and the remaining five were conducted mainly in primary care settings with disparities in both program content and exercise intensity.
In contrast to the findings of the Cochrane review, 2 a randomized trial carried out in the United Kingdom reported similar improvements in exercise capacity and HRQoL in patients with COPD who completed an outpatient hospital-based PRP and those randomized to a group-based PRP provided in a non-healthcare facility. 8 In this study, all assessments were conducted within the hospital due to perceived safety concerns associated with carrying out an incremental shuttle walk test in the community. A large audit of PRPs (224 programs) throughout England and Wales found that 53% of programs were provided in non-healthcare facilities, usually with at least two staff members involved in patient supervision and program delivery. 9,10 Overall the audit findings demonstrated improvement in exercise capacity and health status, however, data were not reported separately for the programs conducted in non-healthcare facilities.
To improve availability and overcome some of the barriers to attending PRPs, we set up a network of community-based PRPs (CPRPs). We refer to ‘community’ pulmonary rehabilitation as a program conducted in a non-healthcare facility such as a recreation centre. In contrast to earlier work, all aspects of pulmonary rehabilitation were conducted in these non-healthcare facilities with only one staff member supervising. The aim of the study was to evaluate the feasibility of these CPRPs and determine whether uptake and completion are improved by providing services closer to people’s homes. Further, outcomes comprising exercise capacity, HRQoL and hospitalization were examined to establish whether these programs provide an alternative to hospital-based programs.
Methods
In this prospective observational study, we evaluated data from a network of CPRPs over a 3-year period (2011–2013). All participants provided written consent for their data to be used for reporting purposes. The Sir Charles Gairdner Human Research Ethics Committee deemed the study to be of negligible risk and we were advised that formal approval was not required.
Establishing location of CPRPs
Mapping of existing PRPs in metropolitan Perth (Western Australia) was undertaken to identify areas of high need and poor availability. The area covers 5386 km2 and has a population of 1.65 million. Potential venues in these areas that met facility requirements (Table 1) were identified. The CPRPs were implemented in a phased approach at five venues that were geographically located between existing hospital-based PRPs.
Facility requirement and safety checklist.

6MWT: 6-minute walk test; SpO2: oxygen saturation via pulse oximeter; HR: heart rate, bpm: beats per minute; CPRP: community-based pulmonary rehabilitation program.
Participants
Criteria for suitability to undertake pulmonary rehabilitation in a non-healthcare setting were determined by a group of ‘experts’ including physiotherapists experienced in pulmonary rehabilitation and respiratory physicians (Table 2).
Inclusion and exclusion criteria for CPRP.

Referrals to hospital-based PRPs were examined by the program coordinator (physiotherapist) to determine the individual’s suitability to attend a CPRP. Medical records were viewed and, where deemed necessary, a screening 6-minute walk test (6MWT) was conducted in the hospital facility to ensure that oxygen saturation levels fit the safety checklist (Table 1). Referrals were also accepted directly to the CPRPs from general practitioners and respiratory physicians if the individual met the inclusion criteria.
Staffing and program content
Six physiotherapists were involved in delivering the CPRPs. Each held certification in cardiopulmonary resuscitation and had completed a workshop provided by a specialist PRP team employed at a tertiary hospital.
The programs were continuous and rolling. Participants attended assessment sessions pre- and post-program and two supervised group sessions each week for 8 weeks. They were also prescribed a home exercise program to complete on 2 or 3 additional days.
The exercise training was standardized and based on the training utilized in a hospital-based program that has been shown to be effective. 7 Training comprised lower limb endurance exercise (20–30 min of ground-based walking prescribed at 80% of the average speed achieved on the 6-minute walk test (6MWT)), 11 and a circuit of upper limb endurance exercises and functional lower limb strengthening exercises using hand weights and body weight, respectively. Exercise intensity and duration were progressed according to symptoms. Individuals with a prescription for supplemental oxygen used the portable oxygen equipment provided by their supplier during exercise testing and training. Where necessary, interval training was used to maintain oxygen saturation (SpO2) ≥ 85%.
Informal education sessions with a self-management focus were incorporated into each class. 12 Individuals were encouraged to actively participate and problem solve. Where indicated, participants were referred to other health professionals (e.g. respiratory nurse, dietitian).
To encourage program participation and completion, participants were contacted by the physiotherapist supervising the PRP if they failed to attend two consecutive classes. Strategies to manage the barriers to attending were discussed and where medical problems impacted on attendance the duration of the program was extended.
Following program completion participants were offered a supervised weekly maintenance exercise class 6 or continued independently with their home program.
Safety checklist
A safety checklist was developed to reduce the likelihood of an adverse medical event and to prepare participants for any emergencies (Table 1).
Outcome measures
The 6MWT was used to measure functional exercise capacity and was carried out in accordance with recommended guidelines (see modifications – Table 1). 13,14 Oxygen saturation (Rad-5 pulse oximeter with finger probe, Masimo Corporation, Irvine, USA) and heart rate (Polar a1 heart rate monitor, Polar Electro, New York, USA) were continuously monitored during the test. Two 6MWTs were performed at pre-program assessment unless performance on the first test was limited by musculoskeletal symptoms, or the participant had performed the 6MWT in the previous 6 weeks. 13 The best distance of the two tests was used for exercise prescription and data analysis. At follow-up assessment a single 6MWT was performed. 15
Health-related quality of life was measured using the self-administered version of the chronic respiratory questionnaire (CRQ-SAI) with individualized dyspnoea domain. 16
Respiratory-related hospital admissions and length of stay were recorded using a healthcare utilization questionnaire. Data were collected for the 12 months prior to and following the program and verified by searching hospital databases.
Analysis
Data were analysed using (Statistical Package for Social Sciences (SPSS), version 22.0, IBM corp., Armonk, New York, USA). Data were checked for normality and no transformations were required. The baseline characteristics of those who completed and those who did not complete the program were compared using independent t tests. The proportion of individuals in each GOLD grade who did and did not complete the program was analysed using a χ 2 test. Paired t tests were used to compare 6MWD, CRQ-SAI and hospitalization data pre- and post-program. The proportion of individuals with at least one hospital admission pre- and post-program was compared using McNemars test. Data are expressed as mean ± SD or 95% CI unless otherwise indicated.
Results
Three hundred and ninety-four participants with CRD were referred to the CPRP during the study period. Of these, 251 (64%) attended a pre-program assessment. Reasons (n, %) that individuals were not assessed comprised medical problems (32, 22%), conditions precluding participation in a walking-based program (28, 20%), declined participation (27, 19%), transport/travel difficulties (20, 14%), paid employment (3, 2%) and other reasons including social problems and responsibilities as a carer (33, 23%). Most referrals (78%) were from hospital-based programs. Screening assessments were carried out in the hospital setting in 127 (51%) participants. One hundred and sixty-six people (66% of those assessed, 42% of those referred) completed the CPRP. Non-completion (n = 85) was mostly due to medical problems (47, 55%) and poor attendance due to travel difficulties and social problems (24, 28%).
The baseline characteristics of the 251 participants who entered the program are summarized in Table 3. Most (66%) participants reported at least two comorbidities. Among those with COPD, a greater proportion of non-completers were in GOLD grade IV compared with those who completed the program (25% vs. 8% p < 0.001). Following program completion, 114 (69%) agreed to attend a supervised weekly maintenance exercise class.
Characteristics of all participants assessed for community-based pulmonary rehabilitation programs.a

BMI: body mass index; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease; FEV1: forced expiratory volume in one second; %pred: %predicted; FVC: forced vital capacity; DLCO: diffusing capacity for carbon monoxide; GOLD: Global Initiative for COPD; 6MWD: 6-minute walk distance; mMRC: modified Medical Research Council dyspnoea scale; IQR: interquartile range.
aData are mean ± SD unless otherwise stated.
bDLCO %pred – n = 121.
c p < 0.05 completed vs. did not complete program.
Adverse events
There were no major adverse events during exercise testing or training. Ten individuals (4%) had a persistent irregular HR or rhythm during exercise and were referred to their general medical practitioner for management prior to commencing or continuing the program. Four individuals (1%) demonstrated oxygen desaturation to <85% during the 6MWT that did not recover leading to test termination. These participants were sent back to the referrer for further management.
Functional exercise capacity and HRQoL
The magnitude of increase in 6MWD (44 m (37–52 m), 14% (11–17%)) exceeded the minimum important difference (MID) of 30 m 18 (Table 4). Responses to the CRQ-SAI demonstrated improvements that exceeded the MID of 0.5 points per item 19 in all domains except emotional function (Table 4).
Functional exercise capacity and health-related quality of life pre- and post-CPRP in the 166 participants who completed the program.a
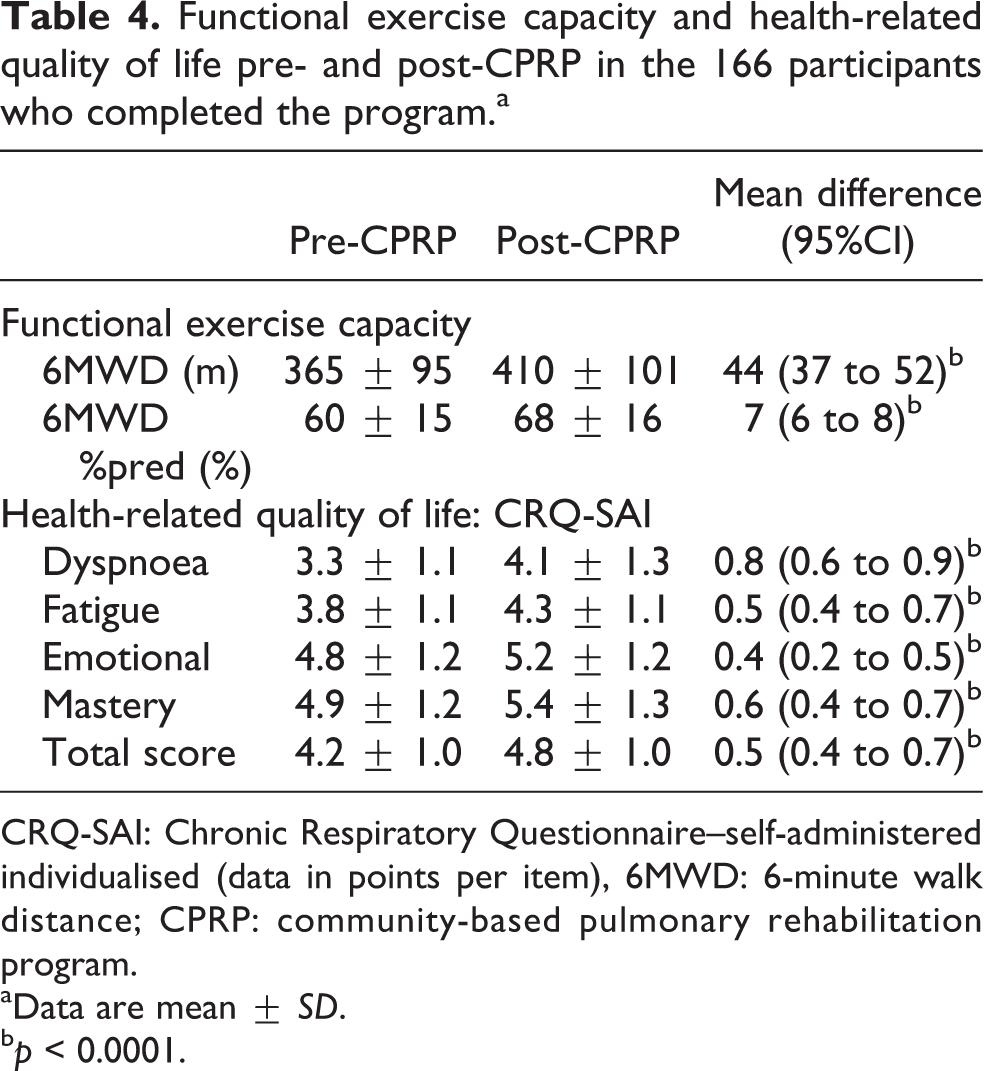
CRQ-SAI: Chronic Respiratory Questionnaire–self-administered individualised (data in points per item), 6MWD: 6-minute walk distance; CPRP: community-based pulmonary rehabilitation program.
aData are mean ± SD.
b p < 0.0001.
Respiratory-related hospitalization
Nine people who completed the program died during the follow-up period and their data were excluded from further analyses. Full data for the 12 months prior to and following the program were available for 136 (87%) of the remaining 157 participants (Table 5). There was a 66% reduction in the number of people who had an admission (50–17), a 67% reduction in the total number of hospital admissions (83–27) and a 72% reduction in total bed days (555–156) following program completion (all p < 0.001).
Respiratory-related hospital admissions for 136 participants (79% COPD) who completed the CPRP.

CPRP:community-based pulmonary rehabilitation program; COPD: chronic obstructive pulmonary disease.
a p < 0.001.
Discussion
This is the first report of outcomes from a large group of individuals with CRD attending a network of CPRPs in Australia. The findings of this study show that PRPs conducted in non-healthcare facilities with strict entry criteria and assessment guidelines are feasible and safe. Further, participants demonstrated improvements in exercise capacity and HRQoL, and had a reduction in respiratory-related hospital admissions in the 12 months following the program.
Uptake (64%) and attrition (34%) from the program were similar to that reported elsewhere. 3 It was anticipated that by offering programs close to people’s homes that had good access to parking and public transport, rates of uptake and completion would be optimized. However, travel difficulties remained a factor influencing program completion and we recommend additional strategies, such as subsidized transport options, are considered for people with limited resources referred to PRPs. Individuals with more severe COPD (GOLD grade 4, lower FEV1, FVC and FEV1/FVC), most likely experienced greater difficulties with transportation and exercise training as a result of severe dyspnoea which contributed to their lower completion rate. Illness was the main reason for non-completion in this study consistent with earlier reports. 3 This was despite the implementation of strategies to facilitate program completion including telephone follow-up after two missed sessions and program extension where indicated. We contend that pulmonary rehabilitation in an outpatient setting is not the most convenient program location for the severely breathless individual and alternatives such as home-based programs may be more feasible.
This study differs from that of Waterhouse et al. 8 in which perceived concerns regarding the implementation of exercise testing in a facility without full resuscitation equipment led these authors to carry out all testing in a hospital. In contrast, we developed inclusion criteria and guidelines to enable exercise testing to be carried out in the non-healthcare facility and report no major adverse events during the 3-year period. Further, our earlier study of 741 patients referred to a hospital-based PRP, only two 6MWTs were interrupted due to cardiac problems with transient oxygen desaturation (SpO2 < 80%) accounting for the remaining adverse events. 20 In the facilities used for the CPRPs, supplemental oxygen was not available, thus modifications to our hospital-based protocol were implemented, for example, exercise testing was contraindicated if resting SpO2 was <91% and a rest imposed if SpO2 fell below 85% during the 6MWT. Individuals on supplemental oxygen were only enrolled in programs if they were independent in the use of their own portable equipment. The continuous measurement of SpO2 and HR is recommended during walking tests. 21 We consider the use of a Polar monitor to assess HR was advantageous by providing a more accurate HR than relying on the pulse rate provided by the oximeter and, on occasions, an abnormal HR was detected via telemetry that required further investigation.
The improvement in 6MWD following program completion exceeded the threshold for clinical importance 18 and is consistent with the findings of a meta-analysis of data from PRPs that utilized minimal equipment for training. 22 Programs that use ground-based walking for lower limb endurance training together with hand weights and body weight for resistance training may be more easily replicated in the home and may better promote exercise adherence and maintenance than programs that rely on expensive equipment.
Following completion of the CPRP improvements in HRQoL exceeded the MID for all domains except emotional function. Our standardized programs supervised by a physiotherapist provided exercise training at an intensity that achieved improvements in dyspnoea and fatigue. While the mastery domain showed improvements exceeding the MID, changes in emotional function did not exceed the MID. We did not test for mood disorders and given the high incidence of depression and anxiety in this population 23 it is possible that we failed to identify individuals who may have benefited from psychological intervention.
The reduction in the number of people who had a respiratory-related hospital admission in the 12 months following completion of the CPRP is consistent with other studies comparing hospitalizations pre- and post-completion of a PRP. 1 The cost benefits of reducing hospitalization are likely to outweigh the cost of implementing the program. 24,25
Strengths and limitations
The strengths of this study are the large number of participants across several programs and the consistent, beneficial outcomes. The training provided to the physiotherapists conducting the CPRPs ensured consistency of program content. One limitation is that that the data were prospectively collected as part of the delivery of the CPRP rather than as a part of a randomized controlled trial (RCT) and therefore it is unknown whether other treatments contributed to the observed effect. However, given the large body of evidence for benefits from pulmonary rehabilitation 2 it is unlikely that further RCTs will be undertaken due to the ethical concerns of denying patients pulmonary rehabilitation when available.
Conclusion
Pulmonary rehabilitation is safe, feasible and effective when conducted with clear guidelines in non-healthcare facilities. Improvements in exercise capacity and HRQoL exceeded the threshold for clinical importance. Further, a significant reduction in hospital admissions occurred following the program. Planning for service delivery should consider community-based pulmonary rehabilitation in non-healthcare facilities to compliment hospital-based service and improve availability for individuals with CRD who are likely to benefit.
Footnotes
Acknowledgement
The authors would like to thank the physiotherapists who conducted the CPRPs: Jo Appelbee, Anita Dinsdale and Jane Stott. Also we thank Jo Cockram for data collection and reviewing the article and Dr Kylie Hill and Jamie Wood for reviewing the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.