
Abstract
The aim of this study was to investigate whether the chronic obstructive pulmonary disease (COPD) assessment test (CAT) reflects the functional status of patients with COPD. Forty-seven patients underwent anthropometric assessment, spirometry, the 6-minute walk test (6MWT), the Glittre-activity of daily living (ADL) test (TGlittre), the London Chest ADL (LCADL) scale, and the CAT. The total score of the CAT correlated with 6MWT distance, TGlittre time spent, and LCADL%total (r = −0.56, 0.52, and 0.78, respectively; p < 0.05 for all). There was significant difference in 6MWT distance (490 ± 85.4 m vs. 387 ± 56.8 m), TGlittre time spent (3.67 ± 1.07 min vs. 5.03 ± 1.32 min), and LCADL%total (24.2 ± 3.02% vs. 44.4 ± 13.3%) between the low and high impacts of COPD on health status (respectively, p < 0.05 for all) as well as in the LCADL%total between medium and high impact of COPD on health status (31.3 ± 7.35% vs. 44.4 ± 13.3%; p = 0.001). In conclusion, the CAT reflects the functional status of patients with COPD.
Introduction
Pulmonary and systemic manifestations of chronic obstructive pulmonary disease (COPD) can trigger dyspnea and fatigue, symptoms that limit activities of daily living (ADLs) 1,2 and gradually reduce the patient’s functional status 3 and health-related quality of life. 4 This functional impairment, in turn, is directly related to the frequency and number of exacerbations and hospitalizations 5 and to mortality rate, 6 with physical activity level being one of the strongest predictors of mortality in patients with COPD. 7 Thus, the decline in functional status impacts the health status of these patients. 8
Among the instruments that measure health status, the COPD assessment test (CAT) is already widely used in clinical practice, despite being a recent test. 9,10 It is a short, simple, and easy-to-understand instrument that provides a broad and comprehensive understanding of the patient’s condition. 11,12 Because of its importance, the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) proposed a new classification of the disease that takes into account the risk of exacerbation and symptoms, which can be measured by the CAT. 1 This instrument has also proved responsive to a pulmonary rehabilitation program 13 –16 and able to assist in the prediction of exacerbations of COPD in patients at high risk, 17 a condition which directly affects functional status. 5
Although the CAT is applied with the aim of encompassing multiple aspects that affect the health status of patients with COPD (i.e. ADL-limiting items and shortness of breath), it is not known whether it can reflect functional status evaluated through specific ADL tests. Therefore, the objectives of this study were firstly to determine whether the CAT is able to reflect the functional status of patients with COPD and secondly to verify if health status can be predicted by three different functional status assessment tests.
Methods
This is a cross-sectional study approved by the Human Research Ethics Committee of Universidade do Estado de Santa Catarina, Florianópolis, SC, Brazil (protocol n°: 222/2011). The study included patients with confirmed diagnosis of COPD referred by pulmonologists to Núcleo de Assistência, Ensino e Pesquisa em Reabilitação Pulmonar (NuReab). The inclusion criteria were as follows: diagnosis of moderate to very severe COPD 1 ; age 40 years or over; previous clinical stability of at least 4 weeks. The exclusion criteria were the following: current smoking; inability to perform any of the evaluations of the proposed protocol; presence of cardiovascular, neurological, musculoskeletal, metabolic, or rheumatologic comorbidities that could influence any of the outcomes assessed; participation in pulmonary rehabilitation program completed in the last 6 months; and episode of exacerbation of clinical symptoms during the period of participation in the study.
Protocol
The protocol consisted of 3 days of evaluation. On the first day, we collected data related to sample characterization: anthropometric measurements using a stadiometer (ISP®, São Paulo, SP, Brazil) and a scale (Filizola®, São Paulo, SP, Brazil) and pulmonary function. On the second day, two Glittre-ADL test (TGlittre) and the London Chest ADL (LCADL) scale were applied, and, on the third day, the subjects answered the CAT followed by two 6-minute walk test (6MWT).
Lung function
Lung function was assessed using the EasyOne spirometer (NDD Medical Technologies®, Zurich, Switzerland), calibrated daily before the evaluation. The methods and the criteria recommended by the American Thoracic Society/European Respiratory Society (ATS/ERS) were applied, 18 following the reference values proposed by Pereira, Sato, and Rodrigues 19 were used. The spirometric measurements were taken before and 15 minutes after inhalation of albuterol (400 mcg) and used for COPD classification according to the GOLD criteria. 1
Health status
COPD assessment test
The CAT is a valid tool for assessing the impact of COPD on health status. 9 It consists of eight items related to cough, phlegm, chest tightness, dyspnea, activities, confidence, sleep, and energy. 9 The score for each item varies from 0 to 5 and the total score varies from 0 to 40, with higher scores representing a greater impact of COPD on the health status of the patient. This impact is classified as low (score 1–10), medium (score 11–20), high (score 21–30), or very high (score > 30). 20 For analysis, we used the total score and the impact categories. The CAT was also used in combination with lung function for the GOLD classification A–B–C–D. 1
Functional status
Six-minute walk test
The 6MWT was used to evaluate functional capacity following ATS/ERS guidelines. 21 Subjects were asked to walk as far as possible along a 20-m corridor in 6 minutes. Every minute, standard phrases of encouragement were used. The following measurements were taken at the beginning, during (second and fourth minute), and at the end of test: blood oxygen saturation (SpO2) using an oximeter (Oxi-Go®, Roslyn, New York, USA), heart rate (HR) using a frequency meter (Polar®, Oulu, Finland), and dyspnea sensation. 22 Blood pressure (BP) was measured at the beginning and once at the end of testing with a sphygmomanometer (Welch Allyn®, Skaneateles Falls, New York, USA) and stethoscope (Littmann®, Saint Paul, Minnesota, USA). Two tests were conducted with a 30-minute interval. The greatest distance was used for the analyses.
Glittre-ADL test
The TGlittre is a multiple-task test that aims to evaluate the functional capacity of patients with COPD. TGlittre is a valid and reliable test for patients with COPD. 23 However, studies that evaluated the TGlittre reproducibility present contradictory learning effects. 23,24 It comprises a 10-m circuit with a chair at one end and a bookcase with two shelves at the other as well as a set of stairs in the middle of the circuit. The subject is instructed to perform the following sequence of daily activities as quickly as possible: rise from the seated position and walk along the flat surface; climb up and down two steps (17 cm high × 27 cm wide) and walk again on the flat surface. At the end of the circuit, the subject must move three objects weighing 1 kg each from the top shelf (shoulder height) to the bottom shelf (waist height) and then to the ground, then return the objects to the bottom shelf and finally to the top shelf. Next, the subject follows the circuit back to the beginning, sits on the chair, and rises immediately to start another lap. The subject must complete the circuit five times, carrying a backpack (2.5 kg for women and 5.0 kg for men). 23
Vital signs were monitored before, during, and after the test, with BP taken at the beginning and immediately after the test. HR, SpO2, and dyspnea sensation according to the modified Borg scale 22 were checked at the beginning of each lap. Two tests were performed. The time to complete the test of best performance was used as an outcome for analysis. The longer the time to complete the test was, the greater the subject’s functional impairment.
London Chest Activity of Daily Living
The LCADL is an instrument that evaluates symptoms of dyspnea in ADLs in patients with COPD. 25,26 It consists of 15 items with scores from 0 to 5, with the total score ranging from 0 to 75 points. The higher the score is, the greater the ADL limitation. 25 The total score (LCADLtotal) and the percentage score (LCADL%total) were used for analysis. 26
Sample size calculation
The sample size was calculated with the aim of achieving a correlation of at least 0.4 between the total CAT score and the outcomes: TGlittre time, 6MWT distance, LCADLtotal, and LCADL%total. With a bidirectional α of 0.05 and β of 0.20, the estimated sample size was 47 subjects. 27
Statistical analysis
Data were stored and analyzed using the Statistical Package for the Social Sciences (version 20.0). Dispersion measures such as mean, standard deviation, and 95% confidence interval were applied to all variables. Data normality was verified by the Shapiro–Wilk test. The Pearson or Spearman correlation coefficients were applied to identify correlations between the total CAT score and the outcomes: TGlittre time, 6MWT distance, LCADLtotal, and LCADL%total. In addition, simple linear regression and stepwise multiple linear regression were applied using the CAT as the dependent variable and 6MWT distance, TGlittre time, LCADLtotal, and LCADL%total as the independent variables. One-way analysis of variance followed by Tukey’s post hoc was used to compare TGlittre and 6MWT performances and LCADLtotal and LCADL%total among the CAT categories. The significance level for the statistical analysis was set at 5% (p < 0.05).
Results
Sixty-seven patients were initially recruited for this study, including 53 potentially eligible subjects. Of these, five were excluded due to exacerbation of COPD during the protocol and one for failure to complete the TGlittre due to limiting sensation of dyspnea. Thus, 47 subjects (36 males) completed the study. The anthropometric data, pulmonary function, and functional status of the sample are shown in Table 1. According to the CAT score, 12 subjects (25.5%) had low impact of COPD on their health status, 16 (34%) had medium impact, 17 (36.2%) had high impact, and 2 (4.3%) had very high impact. Six patients were classified as GOLD II, 23 as GOLD III, and 18 as GOLD IV. Regarding GOLD multidimensional classification, 3 patients were classified as GOLD A, 3 as GOLD B, 3 as GOLD C, and 38 as GOLD D.
Anthropometric characteristics, lung function, functional status, and health status.

kg: kilograms; m: meters; BMI: body mass index; FEV1: forced expiratory volume in 1 s; L: liter; %pred: percentage of predicted; FVC: forced vital capacity; TGlittre: Glittre-ADL test; ADL: activity of daily living; LCADL: London Chest ADL scale; total: total LCADL score; %total: percentage of total LCADL score; min: minutes; 6MWT: 6-minute walk test; CAT: COPD assessment test; COPD: chronic obstructive pulmonary disease.
Correlations between CAT and functional status
The total score obtained in the CAT questionnaire showed strong positive correlation with LCADL%total, moderate negative correlation with 6MWT distance, and moderate positive correlation with TGlittre, LCADLtotal (p < 0.001 for all; Figure 1), and their domains: “self-care” (r = 0.73; p < 0.001), “physical activity” (r = 0.57; p < 0.001), and “leisure” (r = 0.63, p < 0.001). The “domestic activities” domain showed a weak positive correlation with the CAT scores (r = 0.30; p < 0.05).

Correlation between CAT scores and total LCADL score, percentage of total LCADL, TGlittre time, and 6MWT distance. CAT: COPD assessment test; COPD: chronic obstructive pulmonary disease; LCADL: London Chest Activity of Daily Living; TGlittre: Glittre-ADL test; 6MWT: 6-minute walk test.
The variability of the LCADLtotal explained 42% of the variability of the CAT (p < 0.001), and the LCADL%total explained 55% (p < 0.001). The variability of the 6MWT distance explained 32% of the variability of the CAT (p < 0.001), while the TGlittre time explained 28% (p < 0.001). In the multiple linear regression analysis, only the LCADL%total was selected as a predictor of CAT (Table 2).
Simple linear regression between COPD assessment test and functional status and model predictor for COPD assessment test.
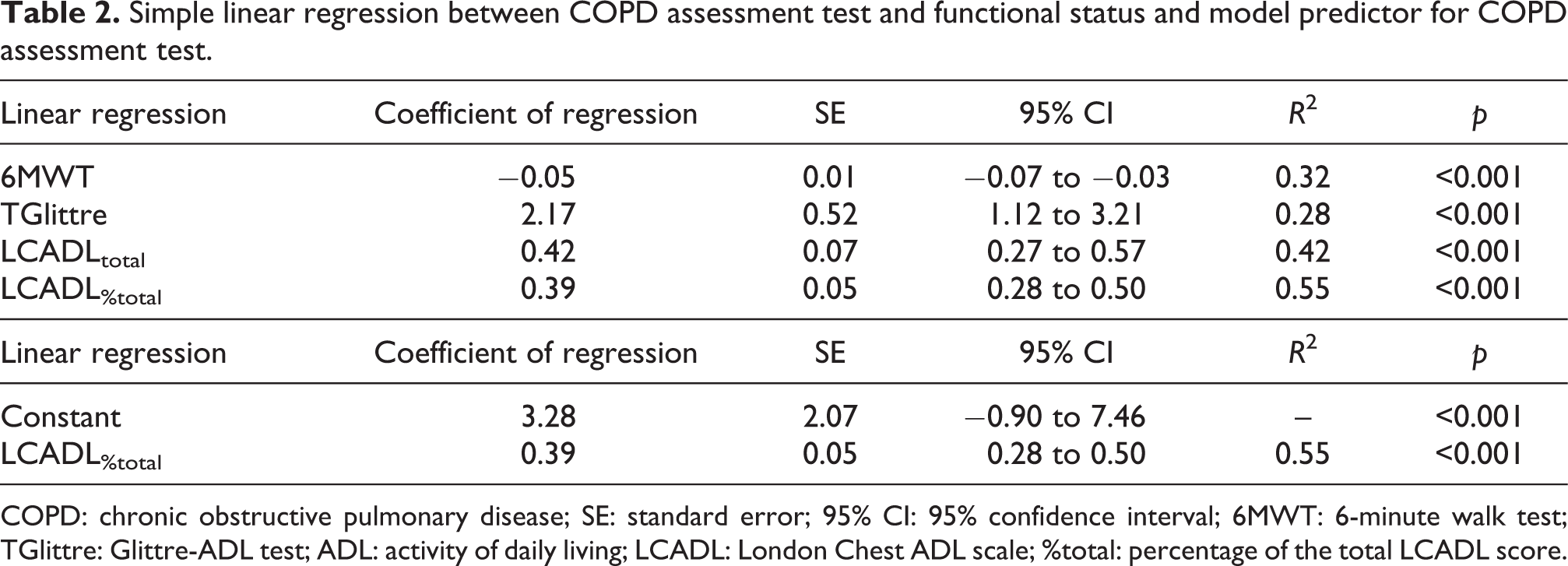
COPD: chronic obstructive pulmonary disease; SE: standard error; 95% CI: 95% confidence interval; 6MWT: 6-minute walk test; TGlittre: Glittre-ADL test; ADL: activity of daily living; LCADL: London Chest ADL scale; %total: percentage of the total LCADL score.
Comparison of functional status among the impact categories of COPD on health status
There was a significant difference between the low and high impacts in 6MWT distance (490 ± 85.4 m for low vs. 387 ± 56.8 m for high; p = 0.002), TGlittre time (3.67 ± 1.07 min for low vs. 5.03 ± 1.32 min for high; p = 0.02), LCADLtotal (15 ± 3.43 for low vs. 29.1 ± 12.9 for high; p < 0.001), and LCADL%total (24.2 ± 3.02% for low vs. 44.4 ± 13.3% for high; p < 0.001). The groups with medium and high impact also differed with respect to LCADLtotal (19.8 ± 6.52 for medium vs. 29.1 ± 12.9 for high; p = 0.01) and LCADL%total (31.3 ± 7.35% for medium vs. 44.4 ± 13.3% for high; p = 0.001) (Figure 2). No significant differences were found between the low- and medium-impact groups.

Comparison of the total LCADL score, percentage of total LCADL score, TGlittre, and 6MWT among low (n = 12), medium (n = 16), high (n = 17), and very high (n = 2) impact of COPD on health status. *p < 0.05. LCADL: London Chest Activity of Daily Living; TGlittre: Glittre-ADL test; 6MWT: 6-minute walk test; COPD: chronic obstructive pulmonary disease.
A significant difference was also found between the low- and high-impact groups for all areas of the LCADL (p < 0.05). The high-impact group showed a significant difference in the areas of self-care and leisure in relation to the medium-impact group (p < 0.05). When comparing the low- and medium-impact groups, physical activity was the only domain that showed a difference between the groups (p < 0.05).
Discussion
The main results of this study were that the health status, assessed by the CAT, correlated with functional status and can be predicted by it when assessed by the 6MWT, the TGlittre, and the LCADL in isolation. However, when analyzed in conjunction in a multiple regression model, only the LCADL%total was able to predict the variability of the CAT score. In addition, it was shown that patients with low impact of COPD on health status have better functional status than those with a high impact.
Functional status is the ability to meet the necessities of life and involves four constructs: functional capacity, functional performance, functional reserve, and use of functional capacity. These constructs are distinct but related and should be considered when choosing tools to assess functional limitation. 28,29 Functional capacity is the maximum potential to carry out activities, while functional performance refers to the daily activities that people actually perform during their routine. 28 Although functional performance is limited by functional capacity, people normally carry out their activities in lower amounts and at lower intensity than their maximum capacity. 30 Thus, even though the instruments for the assessment of functional capacity are highly recommended in clinical practice because they distinguish individuals with impaired functional status and detect changes following interventions, tools that evaluate the actual daily limitations of individuals are also relevant because they reflect the experiences of these individuals. 29 In the present study, the LCADL score was the best predictor of the health status of patients with COPD and it was the instrument that best correlated with the CAT, perhaps because it is the only tool included in the study that evaluates functional performance. As a self-report instrument, the LCADL may better reflect the major limitations perceived by patients in their daily lives and, therefore, the ones that have a greater impact on their health status.
Previous studies have already demonstrated a correlation between the CAT and the 6MWT, with weak correlation (r = −0.24 to −0.37), 8,31 and the LCADL, with moderate correlation (r = 0.63) 32 in patients with COPD. In the present study, the correlations with these instruments were stronger than those seen previously, including a moderate correlation with the TGlittre. This was the first study to find a correlation between the CAT and a specific tool for objective assessment of limitation in ADLs. Recently, it has been suggested that tools involving at least three different tasks be used for the assessment of ADLs. 33 The TGlittre is a multiple-task test developed specifically for patients with COPD 23 that objectively reflects the limitations perceived by these patients in their daily lives. 34
As far as we know, this was the first study to find that the classifications for impact of COPD on health status, according to the CAT score, can differentiate patients with low impact from those with very high impact. Among the other impacts, no significant differences were observed in the assessment tools for functional capacity, while the LCADL showed differences between the medium and high impacts. This finding leads to the hypothesis that instruments that assess the perception of functional limitation better reflect the impact of COPD on health status. The absence of differences between very high impact and other impacts may have been caused by the fact that only two subjects fit this group, compromising statistical power. In the original study for these scores, 35 which was a multicenter study including 1503 patients, the number of patients classified in this condition was also very low (only 11%). It is important to note that the classification of impacts in this study was based only on the scores for the Saint George’s Respiratory Questionnaire 35 and that, since then, very little has been studied about their cutoffs. The results of the present study demonstrate that the classification may be sensitive for identifying the impact on functional status between low- and high-impact groups; however, more studies are needed to evaluate whether all of the classifications are able to identify changes in other important clinical outcomes in COPD.
Because COPD is a systemic disease with multidimensional approach, 1,36 the spirometric GOLD classification is not strongly associated with functional status, 37,38 reinforcing the importance of the inclusion of clinical outcomes in COPD classification other than lung function or the use of the A–B–C–D classification. It should be pointed out that the multidimensional classification does not take functional status into account, only the association between lung function and symptoms. It is important to distinguish patients with greater functional status impairment, given that they are at increased risk of exacerbations, hospitalizations, and mortality. 6,7 In this context, the results of the present study showed that the CAT can be a good instrument to reflect the functional status of patients with COPD in the multidimensional classification.
This study has some limitations that may have reduced the power of one of the analyses: the small number of subjects in the very high COPD impact group. However, some significant differences were observed between these classifications. Furthermore, it is noteworthy that the main objective of this study was to investigate the correlation between the CAT and functional status, thus the number of subjects was in line with the previous sample size calculation, with a power of 95% for the weakest correlation found. 27
In conclusion, the CAT is an instrument that is able to reflect the functional status of patients with COPD. The LCADL was the instrument that best explained the CAT variability and that best differentiated among the impact groups in health status. This shows that perhaps what most influences the patient’s health status is the perception that the patient has over their daily limitations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.