
Abstract
Functional status and quality of life are measures of the chronic obstructive pulmonary disease (COPD) patient’s health status and can demonstrate the impact of the disease on the patient’s ability to perform activities of daily living (ADLs). The Glittre-ADL test was developed to evaluate the functional status of COPD patients and their ability to perform activities of daily life.
The objective of this study was to evaluate the cardiac, respiratory, and metabolic adjustments and reproducibility of the Glittre ADL test performed by COPD patients.
Twenty-two mild to severe COPD patients (forced expiratory volume in 1 second (FEV1): 56.6 ± 19.9% predicted; mean age: 66.3 ± 9.18 years old) were enrolled in this study. Metabolic (oxygen uptake (VO2), carbon dioxide production (VCO2), pulmonary ventilation (VE)/VCO2, and VE/VO2), ventilatory (tidal volume, respiratory rate, and VE), and cardiovascular (pulse oxygen saturation, VO2/heart rate (HR), and HR) variables, lower limbs fatigue, and dyspnea (Borg score) after each lap of two Glittre ADL test were analyzed.
All metabolic, ventilatory, and cardiac variables increased their values up to the third lap and remained stable (plateau) until the end of the test (five laps; multivariate analysis); there was no difference among the time spent to complete each of the five laps in each test and between tests (total time of second test: 4 minutes and 3 seconds); the second test was 17.8 seconds (6.6%) shorter than the first one (NS). All variables were highly reproducible in the two tests (NS). At the end of the test, patients reached 87.7% of the VO2 max, 81% of VE peak, and 88.5% of the HR peak obtained from an incremental maximal test on a treadmill.
The Glittre ADL test is easy for COPD patients to perform and is a highly reproducible test in COPD patients with mild to severe stages of the disease. In addition, our results suggest that it is possible to demonstrate the patient’s functional capacity with a single test of only three laps, making it faster and easier to apply and less stressful for some patients.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable respiratory disease characterized by the presence of chronic airflow limitation, which is not totally reversible. The airflow limitation is progressive and associated with an abnormal inflammatory response of the lungs to the inhalation of noxious gases. 1 Patients diagnosed with COPD usually report fatigue, dyspnea, and activity limitation. Fatigue and dyspnea initially appear after moderate exertion, but as the disease progresses the intensity increases, occurring after minimum physical exertion and limiting the activities of daily living (ADLs). 2 ADLs are defined as tasks of occupational performance that are performed by the patient on a daily basis, such as getting oneself dressed, feeding, or taking a shower. 2,3
Recently, the Glittre activities of daily living test (Glittre ADL test) 4 was developed with the objective of evaluating COPD patient’s functional status and capacity to carry out activities of daily living. The Glittre ADL test was based on the most four relevant questions of the modified version of the pulmonary functional status and dyspnea questionnaire (PFSDQ-M), 5 which evaluates topics related to everyday activities such as walking, climbing stairs, and performing activities using the arms. The outcome of the test is based on the time it takes for the patient to complete all five laps required by the test. 4
However, the original Glittre ADL test study does not mention the patient’s energy expenditure and the cardiac and ventilatory adjustments reached during the test. This information could help understanding the patient’s functional capacity besides identifying whether the patient reaches a plateau during the test, which could express that the critical power was reached as it occurs during the 6-minute walk test (6MWT). 6
Thus, the aim of this study was to evaluate the cardiac, ventilatory, and metabolic adjustments in a group of COPD patients during the performance of two Glittre ADL tests.
Materials and methods
Twenty-two COPD patients from the COPD Outpatients Clinics of the Pulmonary Rehabilitation Center at Federal University of São Paulo (Unifesp) took part in this study. The Ethics and Research Committee of the University approved the research and patients signed an informed consent form.
Inclusion criteria
Males or females with smoking history greater than 10 pack-years, COPD diagnosis according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, 1 age over 40 years old, and had never participated in an exercise rehabilitation program were included in the study.
Exclusion criteria
Patients with any osteoarticular disease that could prevent adequate movements of the upper and lower limbs, obesity (body mass index (BMI) > 30 kg/m2), neoplasia or myocardial infarction within 6 months prior to the test were excluded from the test.
Protocol
Evaluations were completed in two nonconsecutive days. On the first visit, patients performed a spirometry and a maximal incremental test on treadmill. On the second visit, two Glittre ADL tests were performed with a minimum of 30 minutes resting time or the necessary time for all physiologic parameters to go back to the basal values prior to the second test. Exhaled gases, heart rate (HR), pulse oximetry, and ventilatory and metabolic variables were continuously measured during the tests.
Nutritional evaluation
Nutritional evaluation was performed to determine the BMI by dividing the bodyweight in kilograms by the height in square meter. Weight was evaluated in a calibrated scale (Filizola®, Brazil) and stature was measured by means of a stadiometer, with the patients standing with no shoes on. A BMI lower than 22 kg/m2 was considered malnutrition, 22–27 kg/m2 was eutrophic, and above 27 kg/m2 was overweight. 7
Spirometry
It was assessed with a portable ultrasound-based spirometer NDD EasyOne® (Switzerland). Equipment was calibrated daily. Predicted values were calculated according to the Third National Health and Nutrition Examination Survey. 8 Spirometry was carried out with patients in seated position, breathing room air. At least three acceptable maneuvers were obtained according to the American Thoracic Society (ATS) guidelines. 9 Spirometry was repeated 15 minutes after bronchodilator inhalation with a spacer (albuterol 400 μg). 1 No patient showed reversibility.
Gases analysis
Oxygen uptake (VO2), carbon dioxide production (VCO2), pulmonary ventilation (VE), and other variables derived from these measurements were evaluated during the tests on a breath-by-breath mode by a portable device (K4b2Cosmed®, Italy). Patients breathed through a silicon mask firmly adjusted to their face. The K4b2Cosmed is a light and compact device (600 g) with an appropriated design so as not to interfere with the physiological responses during the exercise tests. 10
Glittre ADL test
The Glittre ADL test 4 is a simple test performed in a 10-m long corridor. The test was initiated with the patient seated on a chair, carrying a backpack on the shoulders (2500 g for women and 5000 g for men). Once the patient was instructed to start the test, he/she had to rise from seated position and walk 10 m over an interposed two-step staircase (17 cm high and 27 cm deep each step) up to a wooden rack with two adjustable shelves, one being at the patient’s waist and the other at the shoulder height. Three containers (A, B, and C) of 1 kg each were placed on the shelf located at the shoulder height. The patient had to take container A and place it on the shelf located at waist height and, soon after, on the floor. Then, the patient had to take the same container from the floor and place it on the shelf located at waist height and, thereafter, on the shelf located at shoulder height. The same activity was repeated with containers B and C, sequentially. After placing the last container on the shelf located at shoulder height, the patient walked back toward the chair and sat down. In order to complete the test, the patient was required to perform five laps of this course.
Prior to the test, patients were oriented to perform it the fastest they could without running and no encouragement was given during the test. If necessary, the patients were allowed to rest during the test but were encouraged to resume the test as soon as possible. If the patient stopped to rest, the chronometer went on counting the time. At the beginning and at the end of each lap, respiratory rate (RR), pulse oxygen saturation (SpO2), HR, and Borg score for dyspnea and lower limbs fatigue 11 were measured; blood pressure was assessed before and at the end of the test. The outcome of the test was the total time taken to complete all the five laps. The criteria for interruption were SpO2 (Pulse Oximeter Healthdyne Technologies, Marietta, Georgia, USA; model 920m) below 80%, chest pain, dizziness, nausea, and headache.
Maximal incremental test
Patients were submitted to a maximal incremental test on treadmill according to Harbor protocol 12 (Cybex Q 35 Controlled Impact, Medway, MA, USA). During the first 3 minutes, the patient walked on the treadmill with no inclination. After 3 minute, the treadmill speed was kept stable, and the inclination was increased by 1% at every minute.
The test could be interrupted by the patient in case of dyspnea or fatigue or by the technician if the patient presented any of the following conditions such as reaching maximal HR, precordial pain, dizziness, malaise, frequent ventricular extra systoles, systolic blood pressure drop of more than 20 mmHg below resting level, increase in systolic blood pressure above 260 mm Hg, increase diastolic pressure above 120 mmHg, or a decrease in SpO2 below 80%. Continuous cardiac monitoring (Ecafix Active Model, Brazil) and SpO2 assessment were performed during the test. Dyspnea and lower limbs tiredness were evaluated before and at the end of the test using the modified Borg scale. 11
Statistical analysis
For an α of 0.05 and β of 0.80, a sample size of 17 patients was necessary. 13 Since the sample had a normal distribution, Kolmogorov–Smirnov parametric test was used. The general linear model (GLM) was used to compare physiological data of the Glittre ADL test between the rest and the laps of tests 1 and 2. GLM was also used to compare the differences within each test between a given lap and the previous lap. When any difference was detected, the Bonferroni post hoc analysis was applied. Statistical significance was determined by p < 0.05.
Results
Twenty-five patients were initially evaluated. Three discontinued due to pulmonary exacerbation during the evaluation period. Thus, the final study sample consisted of 22 individuals (20 males and 2 females). All 22 patients were able to finish the Glittre ADL test and maximal incremental test, without any intercurrence or need for supplemental oxygen. The mean values and standard deviation for the anthropometric parameters and pulmonary function for the 22 patients are demonstrated in Table 1.
Demographic characteristics of the 22 patients with COPD.

ADL: activities of daily living; FEV1: forced expiratory volume in 1 second; BD: bronchodilator test; FVC: forced vital capacity.
There were no statistical differences in the mean cardiovascular, ventilatory, and metabolic variables and in the perception of dyspnea and fatigue of lower limbs before both Glittre ADL tests, indicating that the patients started both tests under the same conditions (Tables 2 and 3).
Values obtained at rest and at the end of each lap during the first Glittre ADL test.a

ADL: activities of daily living; VO2: oxygen uptake; VCO2: carbon dioxide production; VE: pulmonary ventilation; VE/VO2: oxygen equivalent; VE/VCO2: carbon dioxide equivalent; HR: heart rate; RR: respitratory rate; SpO2: pulse oxygen saturation.
aValues are expressed as mean ± SD.
bSignificant difference compared to the rest value.
cSignificant difference compared to the previous lap value.
Values obtained at rest and at the end of each lap during the second Glittre ADL test.a
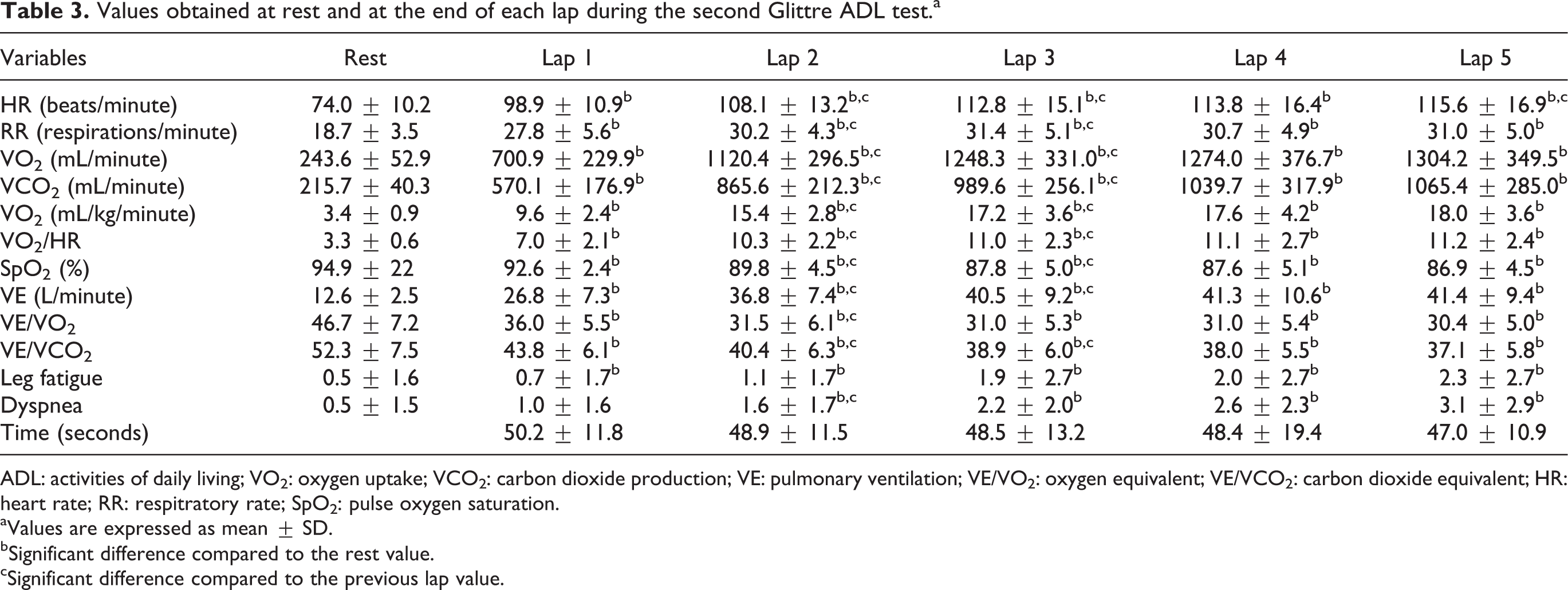
ADL: activities of daily living; VO2: oxygen uptake; VCO2: carbon dioxide production; VE: pulmonary ventilation; VE/VO2: oxygen equivalent; VE/VCO2: carbon dioxide equivalent; HR: heart rate; RR: respitratory rate; SpO2: pulse oxygen saturation.
aValues are expressed as mean ± SD.
bSignificant difference compared to the rest value.
cSignificant difference compared to the previous lap value.
Comparison between the two Glittre ADL test
There was no statistical difference between the duration of the two Glittre ADL tests (first test: 260.8 seconds; second test: 243.2 seconds). Similarly, no differences in the cardiovascular, ventilatory, and metabolic variables were seen between the two tests (Tables 2 and 3).
The multivariate analyses values of VO2, VCO2, and their ventilatory equivalents, cardiac and ventilatory variables, lower limbs fatigue, and dyspnea for the five laps of each Glittre ADL test are shown in Tables 2 and 3. One can observe that there was a progressive increase in all analyzed variables until the third lap. From the third lap onwards, the variables stabilized and did not present statistical difference, plateauing (Figures 1 and 2).
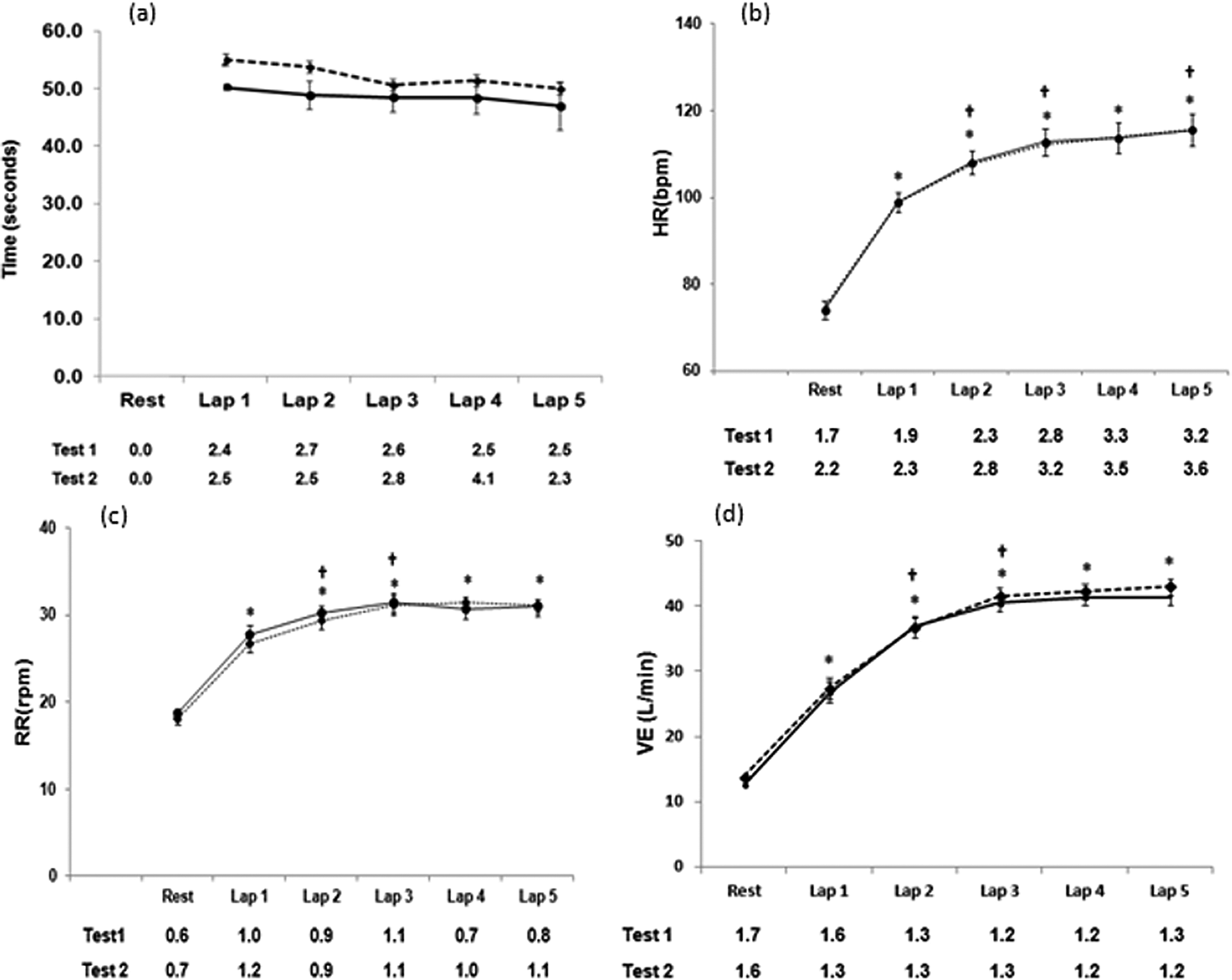
Curves representing the duration (a), heart rate (b), respiratory rate (c), and pulmonary ventilation (d) of Glittre ADL tests 1 (dashed line) and 2 (continuous line) along the five laps. *Compared with the rest values. †Compared with the previous lap values. ADL: activities of daily living.

Curves representing VO2 (a), VCO2 (b), VE/VO2 (c), and VE/VCO2 (d) of Glittre ADL tests 1 (dashed line) and 2 (continuous line) along the five laps. *Compared with the rest values. †Compared with the previous lap values. VO2: oxygen uptake; VCO2: carbon dioxide production; VE: pulmonary ventilation; VE/VO2: oxygen equivalent; VE/VCO2: carbon dioxide equivalent; ADL: activities of daily living.
Table 4 presents the values of HR, VE, and VO2 at the end of the two Glittre ADL tests in relation to their values at the peak of a maximal incremental test on a treadmill.
Oxygen uptake, heart rate, and pulmonary ventilation at the end of the two Glittre ADL tests in relation to their values at the peak of a maximal incremental test on a treadmill.a
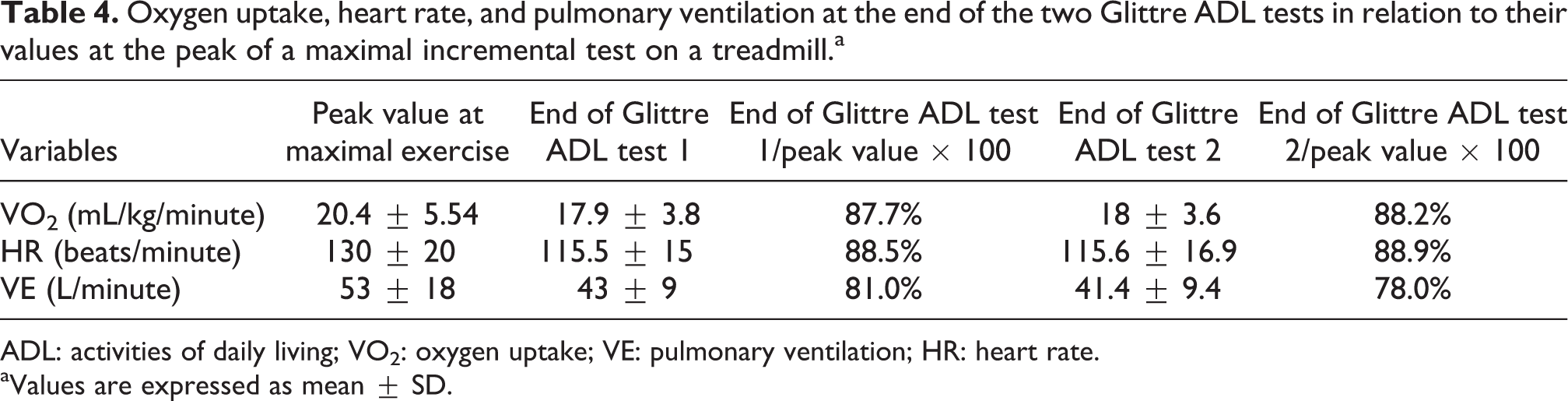
ADL: activities of daily living; VO2: oxygen uptake; VE: pulmonary ventilation; HR: heart rate.
aValues are expressed as mean ± SD.
Discussion
The aim of this study was to analyze the performance of cardiac, ventilatory, and metabolic adjustments during five laps of two Glittre ADL tests. This test was developed to be used as an additional tool for the evaluation of the general capacity of patients with COPD in performing daily living and functional activities. To the best of our knowledge, few studies have evaluated the Glittre ADL test and have shown that the test is easily applicable and that the patients can perform them without any difficulty. 4,14 However, the reproducibility of Glittre ADL test had not yet been studied considering the cardiac, ventilatory, and metabolic adjustments of COPD patients throughout the test.
The main findings of this study were, firstly, there was a great similarity on how patients performed the two Glittre ADL tests according to the analysis of the cardiac, ventilatory, and metabolic variables as well as perception of dyspnea and tiredness of lower limbs. Secondly, there was a progressive increase of the cardiac, ventilatory, and metabolic variables up to the third lap, when thereafter they stabilized and plateaued until the end of the test. These findings show that the Glittre ADL test is highly reproducible and suggest that, in cases where it may be impractical to perform a second test, it is possible to rely on the data found in a single test.
The second Glittre ADL test was completed by the patients in a slightly shorter time (17 seconds or 6.6%). This difference is similar to what was found by Skumlien et al. 4 in their original study (22 seconds or 7%), but the difference showed no statistical difference. The mean total time of the first Glittre ADL test (4 minutes 20 seconds) was also similar to their study (mean of both tests: 4 minutes 40 seconds). However, the variability of our patients was somewhat lower (from 2 minutes 3 seconds to 5 minutes 4 seconds) than Skumlien et al. 4 patients (from 2 minutes 34 seconds to 14 minutes 28 seconds). It is possible that this disparity has occurred due to the different severity of patients. The population studied by Skumlien et al. 4 consisted of mainly moderate to severe disease (GOLD II and III), while most of our sample consisted of moderate patients (GOLD II). This indicates that more severe patients perform the test with greater difficulty and take a longer time to perform it, which is expected.
The study by Skumlien et al. 4 does not describe the duration of each lap. We observed that the individual time spent to perform each of the five laps were very similar, with no statistical difference among them. This demonstrates that, when the patients are adequately instructed, they keep the maximum possible effort to allow them to perform the Glittre ADL test with a very stable effort. We observed a continuous increase of VO2 and VCO2 from resting to the third lap, at approximately 3 minutes. Thereafter, patients maintained a plateau. Usually, a stabilization of VO2 is expected to occur in moderate physical activity after 3–4 minutes. 15 This behavior has also been shown for the 6MWT test and seems to be a typical behavior of submaximal tests. 6,16
When Skumlien et al. 4 first described the Glittre ADL test they only measured time spent and dyspnea in order to characterize their patient’s performance. Considering that the Glittre ADL test should reflect how COPD patients would perform their ADL, we believe that the VO2 evaluation throughout the test may help to better understand how the patients would perform their activities in their real life. We showed that COPD patients when performing the Glittre ADL test present VE and VO2 values close to the peak values measured in the maximal incremental test. Our results are similar to three recent studies on energy expenditure of COPD patients during several ADLs, which also showed high VE/maximal voluntary ventilation (MVV) and VO2/VO2 max ratios. 17–19 The high VE/VE peak of the maximal incremental test (0.81) shows that our patients presented ventilatory limitation. Velloso et al. 20 had already shown that patients with COPD performing four simple activities of daily living for 5 min, such as erasing a whiteboard and sweeping the floor, presented an increase in VE/MVV ratio, which confirms a ventilatory limitation of patients with COPD in performing simple daily activities. Velloso’s et al. 20 finding is in keeping with what we have observed in our study.
There was a progressive increase in HR up to the third lap, which corresponds to approximately 3 minutes of Glittre ADL test, thus maintaining a plateau. At the end of the test, the HR/HRmax ratio reached 0.89, leaving a small cardiac reserve, indicating the patients accomplished a very high degree of effort. The oxygen pulse at the end of the test was two to three times higher than the resting value. The oxygen pulse is a variable that reflects the work done by the heart or, in other words, it may be considered as the effort done by the patient. In a recent study with COPD patients performing ADL during 10 minutes, 17 the oxygen pulse reached 9.23 ± 0.54 ml/heart beat, a value somewhat lower than the one found by us. This may indicate that the Glittre ADL test, even though being described as a test that reflects the ADLs, demands more effort to be performed.
Recently, it has been discussed the importance of critical power in activities that demands effort. 6,21,22 Critical power is defined as the maximum work rate that can be sustained for a long period of time, probably without a substantial contribution of anaerobic source for adenosine triphosphate regeneration. 23 It has been described that the plateau sustained by the patients with COPD after the 3rd minute of the 6MWT indicates that they reached their critical power. 6 Similar to 6MWT, our results show that after the third lap, approximately in the 3-min, the cardiac, ventilatory, and metabolic variables in the Glittre ADL test reached a plateau, suggesting that the patients had reached their critical power. It is possible that the plateau observed by us in the Glittre ADL test may reflect the tolerance and ability of the patients in performing ADLs, such as domestic chores, quick walks, climbing stair, and so on.
ADL evaluation is not a simple task. The ideal evaluation would be the one performed at the patient’s own environment to determine deficiencies or limitations that could be treated or adapted. However, this option is not always feasible, and patients are usually observed at the laboratories or questioned upon their daily activities, which may not quite reflect their limitations. 17 The Glittre ADL test tries to overcome this situation by recreating activities that are very similar to usual ADLs besides being based on the most consistent questions of the PFSDQ-M, 5 a questionnaire specifically developed to evaluate the performance of ADLs by COPD patients. The originality of this study lies in the fact that it is the first one to evaluate the cardiac, ventilatory, and metabolic adjustment in COPD patients during the two tests of Glittre ADL tests and to show their reproducibility. Recently, Karloh et al. 14 showed that the Glittre ADL test can induce slightly higher VO2 than the 6MWT with similar cardiovascular and ventilatory demand and ventilatory efficiency. In keeping view with our results, the physiological variables reached a plateau after the third lap during Glittre ADL test. However, they did not evaluate the reproducibility of Glittre ADL test.
Nevertheless, this study is limited by the fact that most of the patients having mild to severe levels of airflow obstruction were evaluated, not allowing us to generalize the results to more severe patients. Another minor limitation was the fact that 90% of the patients were male, but a large percentage of male over female patients have also been seen in large clinical trial as UPLIFT 24 and TORCH. 25
The cardiac, ventilatory, and metabolic evaluation of COPD patients during the Glittre ADL test allows us to conclude that the test is highly reproducible in mild to moderate COPD patients, it may be completed in a short time, and it is possible that the plateau reached may reflect the patient’s critical power. It is necessary to evaluate patients performing ADL to confirm the significance of these values in a routine use. In addition, although we do not necessarily advise a change in the original test technique, our results suggest that, in cases where it is unfeasible to perform two tests, or five laps as suggested, it is possible that a single test of three laps could reflect the functional capacity of a patient. This way, the test would be faster, easier to apply, and less stressful for some patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.