
Abstract
Patients with chronic obstructive pulmonary disease (COPD) are routinely prescribed one or more inhaled medications. Adherence to inhaler medications and correct inhaler device technique are crucial to successful COPD management. The goals of this study were to estimate adherence and inhaler technique in a cohort of COPD patients. This was an observational study conducted on a sample of 150 COPD patients. Medication adherence was assessed using the Medication Adherence Report Scale (MARS). Inhaler technique was assessed using standardized checklists. Clinical data were collected using a proforma. Of the 150 patients (mean age 70.3 years, 52% male), 58% reported suboptimal adherence (MARS ≤ 24). High adherence to therapy (MARS = 25) was associated with older age (p = 0.001), but not any of the other studied variables. Medication non-adherence was not associated with COPD exacerbations. Errors (≥ 1) in inhaler technique were common across all of the types of inhaler devices reportedly used by patients, with the highest proportion of errors among Turbuhaler users (83%) and the least proportion of errors among Handihaler users (50%). No clinical variables were associated with errors in inhaler technique. Suboptimal adherence and errors in inhaler technique are common among COPD patients. No clinical variables to assist in the prediction of medication non-adherence and poor inhaler technique were identifiable. Consequently, regular assessment of medication adherence and inhaler technique should be incorporated into routine clinical practice to facilitate improved health outcomes among patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) imposes a significant health and economic burden on patients, their families and society as a whole. COPD is currently the fourth leading cause of death worldwide, with a global prevalence rate of 9–10% in adults ≥40 years of age. 1 The morbidity and mortality associated with COPD have risen dramatically over the past 40 years, and it is expected that this trend will continue into the foreseeable future. 2 In 2008, it was estimated that the cost of COPD to the Australian community was AUD $8.8 billion, of which almost AUD $1billion was due to direct health system expenditure. 3
An acute exacerbation of COPD (AECOPD) is defined as:
an event in the natural course of the disease characterized by a change in the patient's baseline dyspnea, cough and/or sputum and beyond normal day-to-day variations, that is acute in onset and may warrant a change in regular medication in patients with underlying COPD.
4
Medications that have been demonstrated to reduce the risk of AECOPD include long-acting bronchodilators (long-acting beta agonist (LABA) or long-acting anti-muscuranic agents), inhaled corticosteroid (ICS), combination of LABA and ICS, dual bronchodilators and prophylactic antibiotic therapy. 6 However, several studies have reported that among COPD patients, non-adherence to inhaled medications is common, ranging from 20% to 60%. 6 –12 This is concerning since Vestbo et al. reported in an observational study nested within a randomized controlled trial that adherence to inhaled medication was associated with a significantly reduced risk of death and admission to hospital due to COPD exacerbations. 9 Retrospective analyses of COPD large patient and medication databases have also identified that increased proportion of days covered with inhaler medications is associated with reduced hospital and emergency presentations for COPD patients. 13,14
Another critical component of inhaler medication use in patients with COPD is correct inhaler technique. It is recognized that incorrect use of inhalers is common among patients both patients with COPD and asthma and is associated with poor disease control. 15 –18 Not surprisingly, COPD guidelines emphasize the importance of demonstration of good inhaler technique to patients and to regularly check that the patient has the correct inhaler technique. 19 To assist in this endeavour, the National Asthma Council Australia (http://www.nationalasthma.org.au/managing-asthma/how-to-videos/using-your-inhaler) and Lung Foundation Australia (http://lungfoundation.com.au/wp-content/uploads/2014/02/08.-Using-your-inhalation-devices.pdf) have developed and promoted a series of video clips and checklists that allow clinicians and patients to assess inhaler technique so that errors in technique can be rectified. However, there have not been any Australian studies that have evaluated inhaler technique in COPD patients.
The aims of this study are to: (1) quantify the frequency of medication non-adherence in a cohort of COPD patients; (2) assess COPD patients’ inhaler technique; and (3) identify clinical variables associated with medication adherence and poor inhaler technique.
Methods
The study was a 12-month observational cross-sectional study performed in the Gold Coast Hospital and Health Service (GCHHS). Study participants were recruited either when they were admitted to the hospital (Gold Coast University Hospital) or were enrolled into a community-based pulmonary rehabilitation programme. Only patients with a clinical diagnosis of COPD that was supported by spirometry results (forced expiratory volume in 1 second/forced vital capacity < 70%) were included in the study. Spirometry was measured at disease stability (in AECOPD patients, it was defined as either within 6 months prior to the exacerbation or 6 weeks after recovery). Patients who had been prescribed inhaler medications for a clinical diagnosis of COPD but did not have supportive spirometry results were excluded from the study. For patients admitted more than once during the study period, only the first admission was included in the analysis. Treatment was not influenced by participation in the study. The GCHHS District Human Research Ethics Committee approved the study (HREC/13/QGC/16).
Patients who consented to participate in the study were interviewed and a proforma was used to capture the data: patient's name, age, sex, education, marital status, smoking habits, co-morbid illness and details about their inhaled and non-inhaled medications. During the interview, patients were asked to complete the Medication Adherence Report Scale (MARS). 20 The MARS tool presents participants with five scenarios of non-adherent behaviour. Participants were presented with a 5-point Likert-type scale (1 = always, 2 = often, 3 = sometimes, 4 = rarely and 5 = never) and asked to indicate which response best represented their feeling towards each statement. The scores were summed with a possible range of 5 to 25. A higher total was suggestive of better adherence than a lower score. A MARS total score of 25 was taken as indicative of optimal adherence. 7 Sample size calculation suggested that at least 120 subjects will need to be recruited to identify a difference in medication adherence of 2 points on the MARS (α = 0.05 and β = 0.80).
The National Asthma Council and Lung Foundation standardized ‘inhaler technique in adults with asthma or COPD’ checklist to assess patients’ medication inhaler technique. Subsequently, the patients were categorized as having either no errors in their inhaler technique or ≥1 error in their inhaler technique. When errors were noted in patients’ inhaler technique, patients were taught the correct technique, thus ensuring optimal delivery of medication. Patients were also asked to report on the number of exacerbations they had experienced over the preceding 12 months. Exacerbations of COPD were defined as any illness episode that required the use of antibiotics and/or corticosteroid medication.
Data analysis
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 20.0 (SPSS, Chicago, Illinois, USA). Normally distributed data were analysed for differences between individual groups using the Student's t-test and presented as mean and standard error. Non-parametric data were analysed for differences between groups using the Mann–Whitney U test, and the results were expressed as median and interquartile range. Statistical significance was indicated by p value of less than 0.05.
Results
During the study period, 162 patients consented to participate in the study. However, 12 patients were excluded from further analysis, as their history and spirometry was not consistent with COPD. The characteristics of the study patients are presented in Table 1. There were more male (52%) than female patients, and the mean age (± standard deviation (SD)) of the study cohort was 70 (±8.9) years. Most patients reported that they had less than high school level of education (65%). Approximately 80% of patients reported they were former smokers, and almost 70% of patients had moderate or severe COPD. Patients reported using on average 2.7 (±0.7) inhaled medications for the management of their COPD. An overwhelming majority (92%) reported other medical co-morbidities for which an average of 5.1 (±3.4) oral medications were prescribed per patient. Salbutamol delivered either via metred dose inhaler (MDI) or nebulizer was the most commonly used reliever (as required) bronchodilator, whilst tiotropium was the most commonly used regular bronchodilator. A salmeterol/fluticasone fixed-dose combination was used by almost three-quarters of the patients, of whom 82% used the MDI delivery device and the remainder used the Accuhaler device.
Patient characteristics and medication adherence.
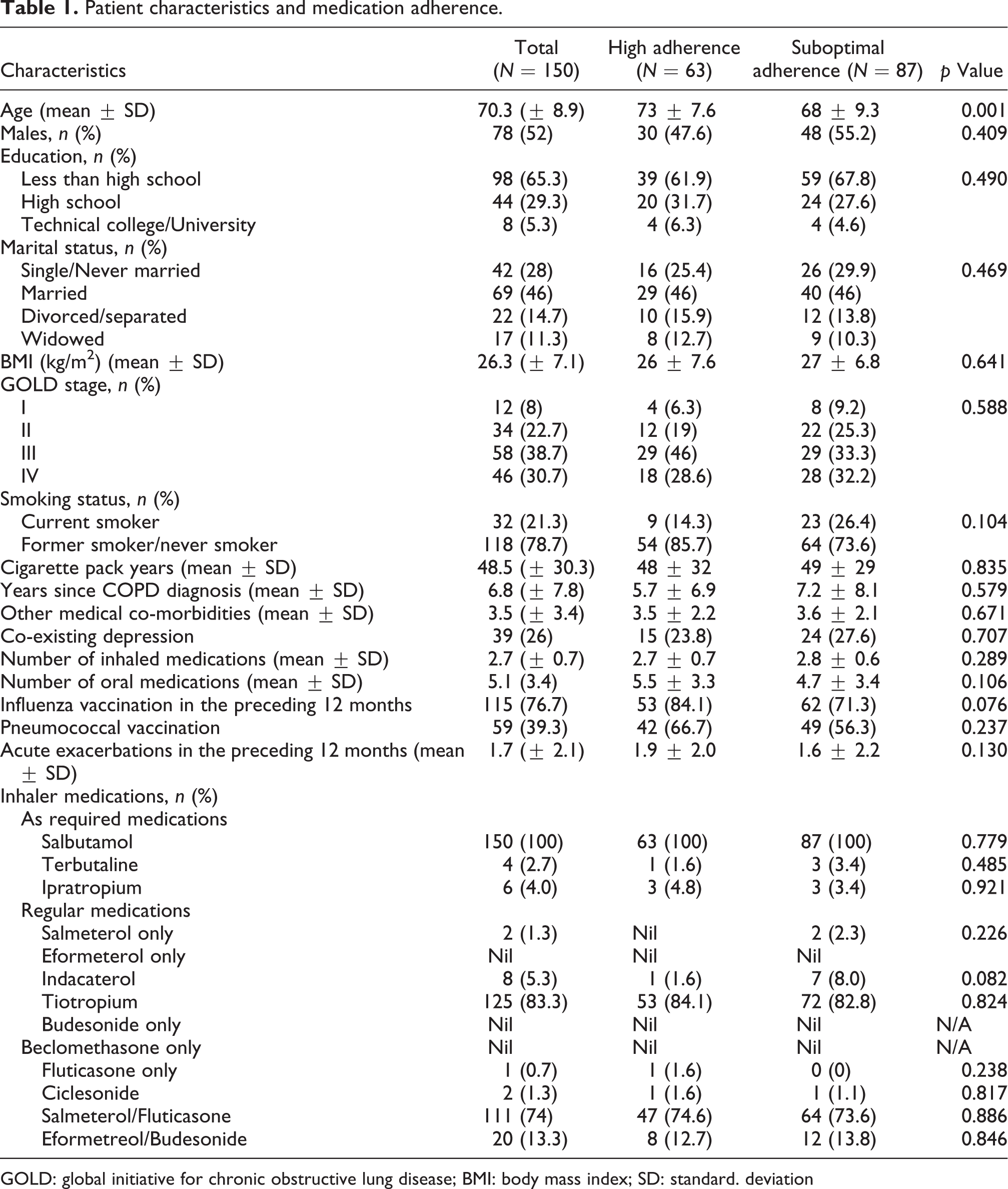
GOLD: global initiative for chronic obstructive lung disease; BMI: body mass index; SD: standard. deviation
The mean score on the MARS in the study population was 23.2 (±2.4). A total of 63 patients (30 men and 33 women) self-reported high adherence on the MARS (score = 25), whilst 87 patients reported suboptimal adherence (MARS ≤ 24). Patients who self-reported high adherence were older than those who reported suboptimal adherence (mean age 73 years vs. 68 years, p < 0.001). No other significant differences were observed between patients who self-reported high adherence and those who reported suboptimal adherence in their demographic and clinical features (Table 1). There was a trend for a higher frequency of acute exacerbations of COPD in the preceding 12 months in the group of patients who reported high adherence compared to the group who reported suboptimal adherence, albeit the difference was not significant (1.9 vs. 1.6, p = 0.13).
Patient characteristics and inhaler device technique are presented in Table 2. It was common for patients to make more than one error in their inhaler technique. The number of subjects using the different inhaler types were as follows: MDI with spacer 128 (85%), Turbuhaler 27 (18%), Handihaler 119 (79%) and Accuhaler 20 (87%). The proportion of patients who had ≥1 error in their inhaler technique was highest for the Turbuhaler (83%), and it was the lowest for patients using a Handihaler (50%). The mean (±SD) of errors among the different inhalers were as follows: 1.52 ± 1.2 for the Turbuhaler device, 2.3 ± 2.7 for the MDI with spacer device, 1.15 ± 1.6 for the Handihaler device and 2.2 ± 2.2 for the Accuhaler device. The most common errors that were noted for each inhaler device are provided in Table 3. The most common errors in inhaler technique for the Turbuhaler were that patients did not check the dose counter and expiry date (63%), MDI with spacer were that patients did not correctly assemble space and check expiry date (40%), Handihaler were that patients did not remove the inhaler from mouth while holding their breath (18%) and ensured that all medication had been inhaled (18%) and Accuhaler were that patients did not check dose counter and expiry date (55%).
Patient characteristics and inhaler device technique.

MDI: metred dose inhaler; SD: standard deviation; GOLD: global initiative for chronic obstructive lung disease; COPD: chronic obstructive pulmonary disease.
Inhaler technique errors among patients.
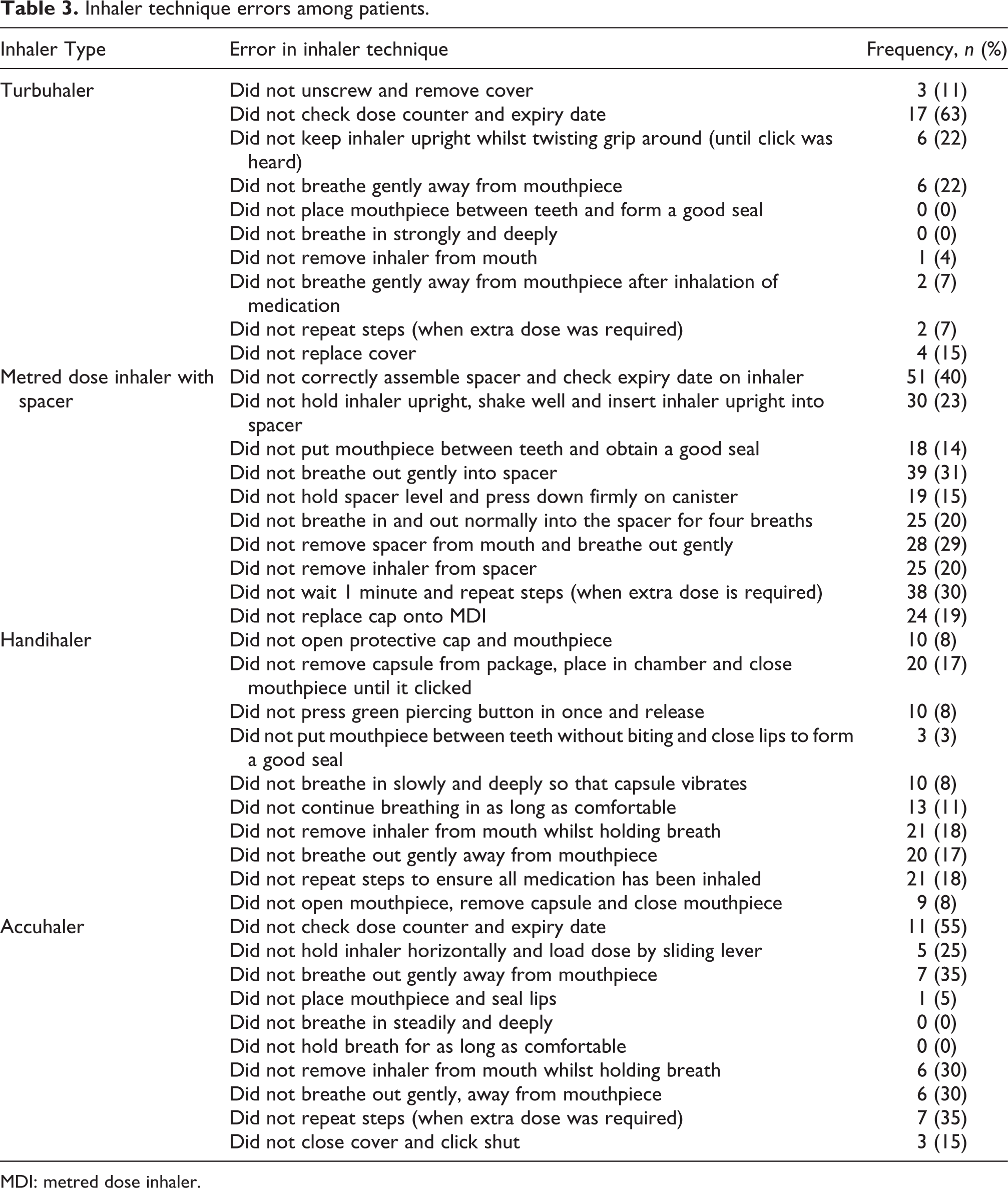
MDI: metred dose inhaler.
There was no observed clinical phenotype differences between the cohort of patients with or without inhaler technique errors for any of the inhalers studied. There was no difference in the frequency of AECOPD between the cohort of patients who did or did not have errors in inhaler technique.
Discussion
It is important to recognize medication non-adherence in COPD patients since it has been reportedly associated with adverse clinical outcomes. In addition to medication non-adherence, poor inhaler technique is often overlooked as a cause of therapeutic failure. In this observational study, we evaluated the adherence and inhaler technique to different inhalation regimens of 150 COPD patients. The majority of patients reported suboptimal adherence to inhaler medications. In addition, at least one or more errors in inhaler technique were identified in the majority of patients, and this was particularly common among patients using Turbuhalers. We did not find any clinical variables that were predictive of either suboptimal medication adherence or errors in inhaler technique. Also there was no association between suboptimal medication adherence, poor inhaler technique and frequency of COPD exacerbations. Nevertheless, our study suggests that clinicians should be vigilant and screen for medication adherence and check inhaler technique of all COPD patients.
In our study, 58% of patients reported suboptimal adherence to their COPD medications, which is consistent with other studies that evaluated self-reported adherence in COPD. 6 –12 Medication adherence to COPD is complex and multifactorial. 21 Previous studies have reported that low self-efficacy, limited knowledge about COPD, poor health beliefs, high perceived barriers to treatment and increased medication concerns are associated with suboptimal adherence, whilst high perception of clinician expertise and effective patient–clinician interaction were associated with high medication adherence. 7,11,12 Other factors that are also thought to play a role in medication adherence include frequency of administration, rapid onset of action and ease of use of inhaler device. 21
We found that patients who reported high adherence were significantly older than the cohort who reported suboptimal adherence (73 vs. 68, p = 0.001), which is consistent with the findings of previous studies. 6,7,22 It has been hypothesized that this may be due to more organized behaviour in old age, which can facilitate better adherence to medications. 7 Conversely, we found that there was no association between self-reported adherence and demographic variables (gender, education, marital status and smoking status), severity of COPD (global initiative for chronic obstructive lung disease (GOLD) stage), duration of illness, co-morbid conditions (including depression) and total number of inhaled and oral medications. This is not surprising, given the association between adherence, and these factors have been inconsistent across studies. 7 Although numerous variables have been identified as affecting adherence with varying degrees of significance, no factor has been shown to be ‘fully predictive’ of whether a patient will demonstrate poor adherence. 23 It is now acknowledged that it is the interplay of a variety of factors rather than individual factors per se that contribute to poor adherence. 24
In our study, the proportion of patients who made at least one error in inhaler technique was high, ranging from 50% to 83% depending on the device used. Recent studies that have evaluated errors in inhaler technique also report similar high proportions of patients with errors in inhaler techniques. 17,18 We did not find any association between the studied social or clinical variables and errors in inhaler techniques. Arora et al. report that older age, low education, lower socio-economic class and increased duration of device usage were associated with increased errors in inhaler technique, whilst patients who were trained by a doctor performed the least number of errors. 17 Similarly, Chorão et al. found that older patients, female patients and dry powder inhalers were associated with increased errors. 18 However, there is a lack of consistency in the identification of clinical variables associated with increased errors in inhaler technique, with other studies not identifying any association between age, 25 gender, 16 socio-economic status 26 and type of inhaler device. 15 The disagreement may be due to methodological differences (assessment of inhaler technique and error scoring systems), devices studied and different patient populations (ethnicity and sample size). One variable that has been reported to be associated with fewer errors in inhaler technique and improved adherence to inhaler medications is repeated instruction by a health professional. 10,17,27 Another reason for the poor inhaler technique may relate to the method of instruction. Bosnic-Anticevich et al. reported that physical demonstration is superior to verbal and written instructions for inhaler technique maintenance. 28
In addition to the overall error rate, the Inhaler Error Steering Committee has identified ‘critical’ errors which are defined as when a patient performs an error, displays imperfect technique or lacks knowledge on usage or maintenance of the inhaler device that is likely to significantly impair the delivery of adequate medication on all occasions. 29 In our study, the leading error that was noted for patients who used a Turbuhaler, MDI with spacer and Accuhaler was that they did not check the dose counter and expiry date. These errors translate to an inability to know when the inhaler device is empty or expired. It is possible that such an error results in a lack of effective medication dose being delivered to the patient, resulting in lack of treatment efficacy resulting in poor disease control both during stable state and during exacerbations. One possible solution to the challenge of inhaler error is for patients to health-care professionals to routinely perform inhaler technique check and provide counselling. Batterink et al. evaluated inhaler technique in hospitalized COPD patients and found that the 43% did not receive any counselling from health-care professionals within the previous 6 months. 30 Whilst we did not specifically evaluate the amount of time taken for inhaler technique assessment, Vanderman et al. recently reported that typically it only takes 2.5 minutes to perform an inhaler technique assessment. 31
Importantly, we also did not find an association between self-reported medication adherence and the frequency of COPD exacerbations. These results are consistent with those of George et al. who evaluated medication adherence in a cohort of 276 Australian COPD patients and reported that there was no association between medication adherence and chest infections or hospital or emergency visits for respiratory complaints in the preceding 12 months. 7 This is not surprising since COPD exacerbations are often seasonal due to virus infections 32 and may not be necessarily preventable with currently available therapeutic regimens. However, the long-term impact of medication non-adherence (e.g. decline in lung function) is not known and was beyond the scope of this study.
Some limitations of this study warrant comment. We used the MARS instrument, which is a self-report questionnaire to measure patient adherence to medications and hence patient responses may have been subject to reporting bias. However, the MARS instrument is a well-recognized medication adherence assessment tool that has been validated against electronic medication adherence measures. 33 Furthermore, there is no universally accepted GOLD standard for measuring medication adherence since all methods have certain limitations. 34 The lack of consistency in the results of studies evaluating clinical variables associated with medication adherence suggests that there are possibly a multitude of factors that are different across study populations which affect the self-reporting of adherence to COPD medications. Another limitation is the utilization of checklists for inhaler technique. A recent review highlights the heterogeneity of checklists for inhaler technique, this limiting the widespread adoption of this approach for inhaler technique assessment. 35
Conclusions
Our study has demonstrated that it is common for COPD patients to have suboptimal adherence to medications and also to use their inhaler devices incorrectly. Health professionals should be more aware of these issues when evaluating and managing COPD patients. Self-report tools and the inhaler technique checklists used in this study are readily available, and we took a pragmatic approach and employed readily available and easily applicable checklists during routine clinical care. These relatively simple tools allow for the identification of patients who may benefit from additional evaluation and education. Future evaluations should explore patients’ health beliefs and perceived barriers to optimal adherence and good inhaler technique. Education will most likely be successful if it is targeted towards addressing patient concerns and deficiencies in knowledge and technique. Future work should explore the duration, frequency and cost-effectiveness of incorporating medication adherence and inhaler checklists in the management of COPD patients.
Footnotes
Acknowledgements
We thank Leanne Chapman, Amber Drysdale, Penny Bishop, Pamela Allen, Samantha Nolan-Neylan, Melanie Harris, Kate Harland, the interns and medical registrars in the Department of Respiratory Medicine (GCUH) for their assistance in recruiting study participants. We are grateful to the patients of the Gold Coast Hospital Health Service, Gold Coast, Australia, for their participation in this study.
Authors’ Note
KBS was involved in study concept and contributed to study design, literature search, patient recruitment, statistical analysis and manuscript preparation and MP contributed to study design, data collation and manuscript review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.