
Abstract
Although recommended by international guidelines, the benefit of inspiratory muscle training (IMT) in addition to rehabilitation remains uncertain. The objective was to demonstrate the effectiveness of IMT on dyspnea using Borg scale and multidimensional dyspnea profile questionnaire at the end of a 6-minute walk test (6MWT) in patients with chronic obstructive pulmonary disease (COPD) with preserved average maximum inspiratory pressure (PImax) of 85 cm H2O (95% of predicted (pred.) value) and admitted for a rehabilitation program in a dedicated center. In a randomized trial, comparing IMT versus no IMT in 32 COPD patients without inspiratory muscle weakness (PImax >60 cm H2O) who were admitted for pulmonary rehabilitation (PR) for 3 weeks, we evaluated the effect of IMT on dyspnea, using both Borg scale and multidimensional dyspnea profile (MDP) at the end of the 6MWT, and on functional parameters included inspiratory muscle function (PImax) and 6MWT. All testings were performed at the start and the end of PR. In unadjusted analysis, IMT was not found to be associated with an improvement of either dyspnea or PImax. After adjustment on confounders (initial Borg score) and variables of interaction (forced expiratory volume in 1 second (FEV1)), we found a trend toward an improvement of “dyspnea sensory intensity”, items from MDP and a significant improvement on the variation in the 2 items of MDP (“tight or constricted” and “breathing a lot”). In the subgroup of patients with FEV1 < 50% pred., 5 items of MDP were significantly improved, whereas no benefit was observed in patients with FEV1 > 50% pred. IMT did not significantly improve dyspnea or functional parameter in COPD patients with PImax > 60 cm H2O. However, in the subgroup of patients with FEV1 < 50% pred., MDP was significantly improved.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major public health problem associated with an important morbidity, quality of life impairment, and mortality. The efficacy of pulmonary rehabilitation (PR) programs on exercise capacity, health-related quality of life, and reduction of hospitalization has been established in patients with COPD, and rehabilitation programs are highly recommended in guidelines for COPD management. 1,2
Inspiratory muscle training (IMT) is efficient when used alone and it has been recommended in patients with inspiratory muscle weakness 1 ; however, its added benefit as an adjunct to whole body training is questionable. 1 IMT would reduce dyspnea by improving the capacity of patients to sustain high level of ventilation and by decreasing hyperinflation. 3 Three meta-analyses of IMT studies in COPD patients have been conducted. 4 –6 Although it has been recently established than the benefits are greater in patients with maximal inspiratory pressure (PImax) lower than 60 cm H2O, 5 some benefits have been also reported in patients with preserved PImax. 5 But to date, the identification of a cutoff of 60 cm H2O was more arbitrary than demonstrated. To our knowledge, there is no randomized trial that included only patients with a PImax > 60 cm H2O. In the randomized study of Beckerman et al., 7 IMT combined with the rehabilitation program in patients with an average PImax greater than 60 cm H2O led to an improvement in dyspnea. In addition, in meta-analyses on IMT, dyspnea was evaluated using classical scales or questionnaire (Borg or visual analog scale, Transition Dyspnea Index, and Chronic Respiratory Questionnaire dyspnea score). However, dyspnea mechanisms are multifactorial, and affective and sensorial components are only taken into account in the multidimensional dyspnea profile (MDP). 8 –10 Moreover, mono-dimensional evaluation of dyspnea such as Borg scale only evaluate the intensity of dyspnea but not the mechanism. 11,12
As IMT is efficient in patients with PImax lower than 60 cm H2O by improving inspiratory muscle strength and endurance, we looked for an effect of IMT on dyspnea using MDP in preserved PImax patients as dyspnea is often the first parameter to improve.
The primary objective of this open randomized trial was to demonstrate the effectiveness of IMT on dyspnea using MDP questionnaire and Borg Scale at the end of a 6-minute walk test (6MWT) in COPD patients with preserved PImax and admitted for a rehabilitation program in a dedicated center. Secondary objectives were to evaluate the effect of IMT on PImax, on 6MWT, on distension indices at rest, such as inspiratory capacity (IC), and at the end of 6MWT, 13 and to identify variables, such COPD severity, that potentially might influence the effect IMT on dyspnea and exercise capacity.
Methods
Study population
Patients routinely admitted in the rehabilitation program unit were eligible for the study if they have COPD diagnosed according to American Thoracic Society/European Respiratory Society criteria 14 and PImax > 60 cm H2O at admission. Non-inclusion criteria were a previous pneumonectomy or lobectomy in the past 6 months, the impossibility to measure IC at the end of the 6MWT, the incapacity to follow the standard rehabilitation program, and the absence of written informed consent. The study was approved by the ethic board on August 2011 (ClinicalTrials.gov identifier: NCT01545011).
Intervention
A computer algorithm, with a randomly determined block size of four or six within each stratum, generated an allocation list in which patients were assigned to follow either a standardized PR program associated with IMT (IMT group) or a standardized PR program without IMT (control group).
The standardized rehabilitation program was conducted during 3 weeks, 5 days per week, and included aerobic exercise on cycle ergometer and on treadmill (30 minutes per day each), 15,16 strengthening of lower and upper limb muscles groups, therapeutic educational program, aerobic gymnastic in groups, smoking cessation program, and sociopsychological and dietary advices.
In the IMT group, all subjects were trained daily in two sessions of 15 minutes each, 5 times a week, during 3 weeks, supervised by a physiotherapist. The patients had to breathe slowly with an increased tidal volume. The IMT was performed using a threshold inspiratory muscle trainer (Threshold IMT®) at a resistance generating a pressure corresponding to 40% of the initial PImax for each session. The intensity was not modified during the program.
Testing and end points
The primary end point was the assessment and the comparison between the two groups of the change of dyspnea using the MDP questionnaire 10,14 and the Borg scales at 3 weeks of the rehabilitation program. Both MDP questionnaire and Borg scale were self-administered and performed at the end of the 6MWT.
The secondary end points were the assessment of the functional changes: PImax measure using a MicroRPM (Micro Medical Limited, UK), 17,18 six-minute walk distance (6MWD), 19,20 and IC at rest and IC at the end of the 6MWT using a portable spirometer (Spirobank II, MIR Medical International Research S.r.l), 21 and all baseline functional measures (i.e. FEV1, FEV1/FVC, TLC, RV, IC, etc.) and two 6MWT were performed in accordance with the international recommendation guidelines. 19,22
Sample size
In both Borg and MDP scales, the standard deviation is about 20% of the mean of the initial dyspnea evaluation. In the study of Koppers et al., evaluating the effect of IMT on Borg scale, the expected rate of scale improvement was 20% of the initial Borg score. 23 For the MDP, we hypothesized that MDP improvement would also be of 20% of the initial score. Based on the previous results in the sensorial component of the MDP scale, 8 we assumed an initial mean of 5, a standard deviation of 1, and a difference of mean of 1. For an α risk of 5% and β risk of 20%, the expected sample size would therefore be of 34 patients.
Data analysis
Continuous variables were expressed in mean (±standard deviation). The effect of IMT on dyspnea and functional parameters were analyzed using the Wilcoxon test for within comparison. The data at baseline and the unadjusted changes observed after training between the two groups were analyzed using a Mann–Whitney U test for between-group comparisons. In the case of heterogeneity between active and control group, changes in dyspnea and functional parameters were compared and adjusted using the analysis of covariance (ANCOVA) procedure. Interactions between variables on the changes in dyspnea and functional parameters were also estimated using an ANCOVA procedure. For comparison tests, a p value of less than 0.05 was considered as statistically significant. All statistical tests were performed using SPSS software 20.0 (version 20.0; SPSS, Inc., Chicago, Illinois, USA).
Results
Between 21 October 2011 and 15 June 2012, 83 COPD patients attended our rehabilitation center. After verification of eligibility criteria, 34 patients were randomized to have IMT (n = 16) or to not have IMT (n = 18), in addition to a standardized PR program (Figure 1). Demographic, clinical and initial spirometric data are reported in the Table 1. Dyspnea measured before the intervention is reported in the Table 2. In both the groups, mean PImax were almost at 95% of the predicted values. There was a trend of a lower mean FEV1 in the IMT group (p = 0.07), whereas dyspnea (Borg) was statistically higher in the control group (p = 0.045). The main analysis has been therefore performed firstly without and secondly with adjustment on these two parameters.
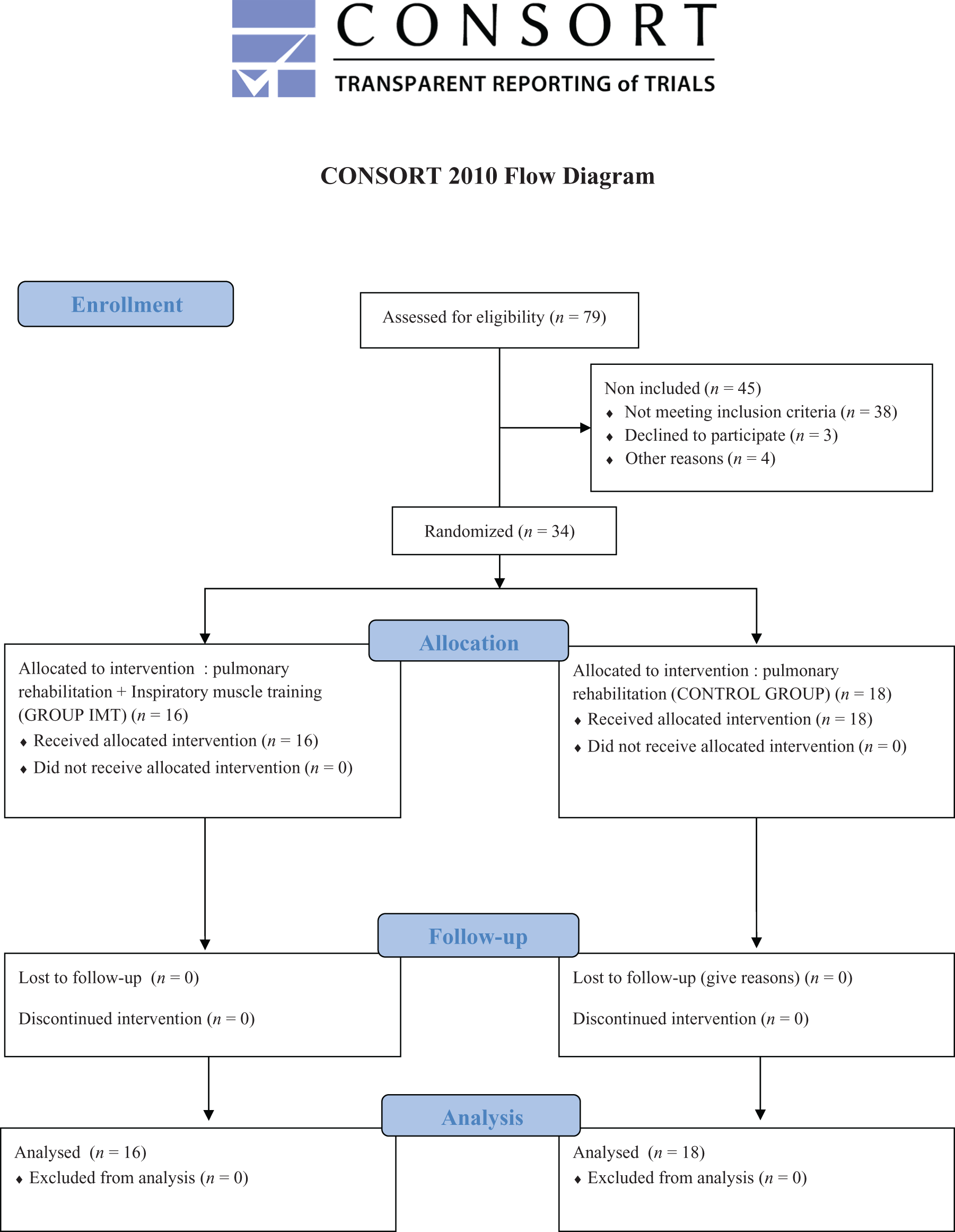
Flowchart of patient’s enrolment.
Baseline patient characteristics and values of the initial tests.a

6MWD: 6-minute walk distance; 6MWT: 6-minute walk test; BMI: body mass index; F: female; FEV1: forced expiratory volume in 1 second; GOLD: Global Organization for Lung Disease; IC: inspiratory capacity; IMT: inspiratory muscle training; M: male; MMRC: Modified Medical Research Council; PImax: maximal inspiratory pressure; pred.: predicted; SpO2: pulse oxygen saturation; RV: residual volume; TLC: total lung capacity; VC: vital capacity.
aValues are expressed as mean ± SD or as median (Q1–Q3) or as number (n).
Baselines characteristics of dyspnea sensation at the end of the 6MWT, according to Borg scale and the MDP questionnaire.a

IMT: inspiratory muscle training; MDP: multidimensional dyspnea profile.
aValues are expressed as mean ± SD or as median (Q1–Q3).
Effect of IMT
In unadjusted analysis, IMT was not found to be associated with significant changes in either primary or secondary end points (Table 3); there was no difference for dyspnea, PImax, 6MWT, and IC between the two groups. Adjustment on initial Borg scale measures and FEV1 did not change the results, except a significant improvement of the variation of the 2 items of MDP scale (‘tight and constricted’ and ‘breathing a lot (rapid, deep, and heavy)’) in the IMT group.
Change in dyspnea sensation and functional parameters at the end of the 6MWT after intervention (MDP and Borg scales) without and with adjustment on initial FEV1 and Borg score.

IMT: inspiratory muscle training; Δ: difference (after minus before intervention); MDP: multidimensional dyspnea profile; 6MWD: 6-minute walk distance; 6MWT: 6-minute walk test; IC: inspiratory capacity; IMT inspiratory muscle training; PI max: maximal inspiratory pressure; pred.: predicted; SpO2: pulse oxygen saturation; FEV1: forced expiratory volume in 1 second; ANCOVA: analysis of covariance.
aValues are expressed as mean ± SD or as median (Q1–Q3).
bMann–Whitney U test.
cAdjustment on initial FEV1 and Borg score (ANCOVA procedure).
IC was increased at the end of the 6MWT in the IMT group even if it was not significantly different between the two groups.
Effect of severity of COPD
On the ANCOVA analysis, we found a significant interaction between FEV1 and IMT on several items of the MDP questionnaire (p = 0.025 for the ‘sensory intensity’, ‘tight and constricted’, and ‘breathing a lot (rapid, deep, and heavy)’). We therefore conducted a separated analysis of the IMT effect on dyspnea scale according to whether FEV1 was higher or lower than 50% of the predicted value (see supplementary appendix).
In patients with severe COPD, the groups with and without IMT were homogenous. At 3 weeks of the rehabilitation program, 5 items of the MDP questionnaire were significantly improved in the IMT group (‘sensory intensity’, ‘mental effort or concentrate’, ‘tight or constricted’, ‘breathing a lot (rapid, deep, and heavy)’, and ‘crush’) compared with the control group and a trend toward an improvement with IMT was found for 2 items (‘muscle work or effort’ and ‘not enough air or smother or air hunger’).
Conversely, baseline characteristics were more heterogeneous in patients with mild COPD. At 3 weeks of the rehabilitation program, no item of the MDP questionnaire was significantly improved in the IMT group, as compared with the control group (see supplementary appendix).
Discussion
In this prospective randomized trial, no benefit of IMT was observed in dyspnea or functional parameters in COPD patients with PImax > 60 cm H2O.
The lower efficiency of IMT as an adjunct of PR than used alone on most parameters including PImax 1,5 and the PImax > 60 cm H2O could explain the absence of benefit in our study. Nevertheless the 60 cm H2O cutoff has been established recently. 1 A previous meta-analysis 5 failed to show that IMT added to general exercise rehabilitation decreased more dyspnea than exercise alone. Indeed, four studies 24 –27 showed PImax improvement despite initial values ranging from 70 cm to 85 cm H2O, but the training protocols were different from ours. Moreover, IMT can increase diaphragmatic velocity by increasing fibers II 28 and reduced inspiratory time 29 and then increase expiratory time, which could allow diminution of hyperinflation (which can be measured with IC at effort) 13,30 ; therefore, IMT may act on dyspnea without any significant Plmax change. 25,26 In our study, IC was not significantly different between the two groups but IC improvement was greater in IMT group than in control group, perhaps by an improvement of diaphragmatic velocity.
IMT program could explain the results of our study. Even if the method (threshold inspiratory training) and the intensity of training (40% of PImax) are in line with recommendations, 5 3 weeks of duration could be too short, the intensity could be too low and, we should increase the intensity during the program. However, Gosselink et al. 5 analyzed studies with duration from 1 month to 4 months and gave no recommendation on program duration.
Despite the randomization, our two groups tended to be heterogeneous in terms of severity: FEV1 was lower in the IMT group whereas baseline Borg scale was unexpectedly higher in the control group. Using ANCOVA analysis, the Borg scale was found to be a confounder and FEV1 a significant variable of interaction. Thus, when adjusting for these two variables, we found significant or trends toward a significant improvement of several items of the MDP questionnaire but no improvement of the Borg scale and of functional parameters. Then, we proposed a subsequently separate analysis according to whether COPD patients had FEV1 higher or lower than 50% of the predicted value (see supplementary appendix). In this group of severe COPD patients, we found a significant improvement in ‘work/effort’, ‘mental concentration’, and breathing a lot ratings. This might indicate that IMT can bring perceptual benefits even though PImax did not increase.
To our knowledge, it is the first study on the effect of rehabilitation program in COPD patients using the MDP questionnaire as an estimator of the effect of an intervention. We found a Borg scale improvement neither in the total analysis nor in the subgroup analysis, but MDP questionnaire appeared to be more sensitive in detecting dyspnea improvement. 8 –10 It has been extensively established that dyspnea is multifactorial 11,12 ; since Borg scale is a one-dimensional approach, the multiple causes of dyspnea might be better explored with this new scale.
Strengths of our study were the randomized design, a well predefined and standardized rehabilitation program that was administered for all entering patients, a predefined and standardized protocol for IMT rehabilitation, the use of predefined objective end points that were performed and measured according to international guidelines 15,17,20 and adjusted analyses taking into account potential confounders or variables of interaction. In addition, if functional tests and data were collected by the physiotherapists who were aware of the group allocation and who conducted the rehabilitation program and tests, the primary end points were self-administered questionnaires that were completed by the patients. The main drawback is the small sample size of the study, which limits the validity of subgroups analyses.
In conclusion, IMT as an adjunct to a 3-week standardized rehabilitation program was not found to be associated with a significant improvement of either dyspnea or functional parameters, in patients with COPD and PImax higher than 60 cm H2O. However, subgroup analysis suggests that IMT might act on dyspnea component of the MDP questionnaire related to effort; this needs to be confirmed in a larger randomized trial in severe COPD patients with and without inspiratory muscle weakness.
Footnotes
Conflict of interest
Dr CMP declares the following conflicts of interest with Pierre Fabre medicaments : member of a board. None of the other authors has a related conflict of interest. I declare that any underlying research materials related to my article (e.g. data, samples, or models) can be accessed.
Funding
Source of funding: EA3878 (G.E.T.B.O.), CIC INSERM 0502, University Hospital of Brest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.