
Abstract
The objective of this study was to investigate whether some activities of daily living (ADLs) usually related to dyspnea sensation in patients with chronic obstructive pulmonary disease (COPD) are associated with dynamic lung hyperinflation (DH) and whether the use of simple energy conservation techniques (ECTs) might reduce this possible hyperinflation. Eighteen patients (mean age: 65.8 ± 9.8 years) with moderate-to-severe COPD performed six ADLs (walking on a treadmill, storing pots, walking 56 meters carrying a 5-kilogram weight, climbing stairs, simulating taking a shower, and putting on shoes) and had their inspiratory capacity (IC) measured before and after each task. The patients were moderately obstructed with forced expiratory volume in 1 second (FEV1): 1.4 ± 0.4 L (50% ± 12.4); FEV1/forced vital capacity: 0.4 ± 8.1; residual volume/total lung capacity: 52.7 ± 10.2, and a reduction in IC was seen after all six activities (p < 0.05): (1) going upstairs, 170 mL; (2) walking 56 meters carrying 5 kilogram weight, 150 mL; (3) walking on a treadmill without and with ECT, respectively, 230 mL and 235 mL; (4) storing pots without and with ECT, respectively, 170 mL and 128 mL; (5) taking a shower without and with ECT, respectively, 172 mL and 118 mL; and (6) putting on shoes without and with ECT, respectively, 210 mL and 78 mL). Patients with moderate to severe COPD develop DH after performing common ADLs involving the upper and lower limbs. Simple ECTs may avoid DH in some of these ADLs.
Introduction
Expiratory airflow limitation, the physiological hallmark of chronic obstructive pulmonary disease (COPD) patients, leads to lung hyperinflation and dyspnea sensation, which may worsen during activities with elevated metabolic demand. 1,2 Reducing dyspnea and improving patients’ exercise tolerance and ability to engage in usual activities, therefore, are important therapy goals in COPD patients.
The mechanisms of dyspnea are not completely known but afferent stimuli originating from the airways, lung parenchyma, rib cage, respiratory muscles, and possibly, cardiovascular receptors, as well as due to lung hyperinflation, may all contribute to the sensation of dyspnea during high ventilation. 3,4 Recently, it was described that awareness of levels of neural respiratory drive is also an important factor for breathlessness. 5,6,7
The negative effects of lung hyperinflation in COPD are already felt in the early stages of the disease and become more intense when the disease has progressed to the moderate and severe stages and the adaptive mechanisms of the respiratory system are no longer as suitable. Efforts during the accomplishment of some activities of daily living (ADLs) might require high minute ventilation that can result in dynamic hyperinflation (DH), air trapping, and dyspnea. 5,6,8,9
It has been shown in COPD patients that an activity such as walking induces hyperinflation, which may be associated with dyspnea. 9 Patients with severe COPD also experience DH and dyspnea in other simple ADLs, such as going up and down a ramp, sweeping and mopping a room, and climbing up and down a set of stairs. 10 Energy conservation techniques (ECTs) such as pursued lip breathing (PLB), among others, have been advocated for use by these patients 11 –14 but their efficacy in preventing hyperinflation has not really been evaluated thus far. Our hypothesis is that the use of ECTs by COPD patients during some ADLs may prevent DH.
Thus the objective of this study was to investigate whether some ADLs usually related to dyspnea sensation in patients with COPD are associated with dynamic lung hyperinflation, and whether the use of simple energy conservation maneuvers can reduce this hyperinflation.
Materials and methods
Participants in this study were selected from a group of COPD patients undergoing initial examinations in order to enter the pulmonary rehabilitation program, according to the criteria outlined by the American Thoracic Society. 12 The protocol was approved by the local ethics committee, and all participants signed an informed consent form.
The inclusion criteria for the COPD patients were as follows: (1) spirometry with moderate-to-very severe COPD; (2) clinically stable, with no pulmonary exacerbations during the previous 4 weeks and no other associated disease (heart, neurological, rheumatic, or orthopedic disease); and (3) no previous engagement in any fitness program. The exclusion criteria were as follows: (1) smoking; (2) use or indication of chronic oxygen therapy; and (3) pulse oxyhemoglobin saturation (SpO2) <80% during ADLs.
Protocol
Patients were made familiar with all procedures prior to beginning the study. All procedures were accomplished in three visits to the pulmonary rehabilitation center. During the first visit, total lung capacity (TLC) and residual volume (RV) by body plethysmography, spirometry with slow vital capacity and forced vital capacity (FVC) maneuvers, maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP; ±150 cm H2O manovacuometer; IMEBRÁS, Brazil), and dyspnea sensation (Borg scale during ADLs) were measured.
Three ADLs were evaluated during the second visit and three other ADLs were evaluated during the third visit. Spirometry, MIP, and MEP were measured at the three visits to check pulmonary function stability. Inspiratory capacity (IC) was measured before and after each ADLs.
Lung function
Measurements were performed according to American Thoracic Society criteria. 12 Spirometry (Koko Systems, The Netherlands) was conducted in triplicate with the patient in a seated position. The largest forced expiratory volume in 1 second (FEV1) and FVC were recorded after examining all the acceptable curves, even if they were not from the same curve. Short-acting theophyllines and long-acting β2 agonists or anticholinergic drugs were withheld for at least 24 hours before spirometry, long-acting theophyllines for at least 48 hours, and short-acting β2 agonists for 8 hours.
IC maneuver
In order to measure IC, the patient breathed quietly through a pneumotach, after after several reproducible tidal volume loops were obtained, the patient was asked to take a maximum inspiration and then was asked to slowly and completely exhale down to RV. IC was calculated as the volume from resting expiratory volume level to TLC. At least three IC maneuvers were performed, two of which had to have a variation of less than 5% to be considered reproducible. IC was measured before and after each ADLs. It was considered as pulmonary hyperinflation loss of IC equal to or greater than 150 mL among the pre and post activity. 2
Body plethysmography
Lung volumes, thoracic gas volume, TLC, and RV were measured using a constant volume variable pressure body plethysmograph according to the methods described by Coates et al. 15
Activities of daily living
The patients were instructed to perform six standardized ADLs as they usually did at home. The activities were performed in a random order, with an interval of at least 30 minutes between them to allow the cardiovascular (heart rate (HR) and arterial blood pressure) and respiratory (respiratory rate (RR), IC, Borg scale, and SpO2) parameters to return to basal values. Continuous HR monitoring and SpO2 were recorded during the following ADLs performance: (1) walking down a corridor (56 meter) carrying a bag weighing 5 kilogram at the patient’s chosen pace, like shopping in a grocery store; (2) going up and down a 10-step staircase once, with each step being 17 centimeter high; (3) walking for 5 minutes on a treadmill with 5% inclination at a speed of 2 miles/hour, simulating walking on an inclined street; (4) putting shoes on and taking them off, bending the thorax over the abdomen, while seated on a chair; (5) lifting pots (1, 2, and 3 kilogram), one at a time in increasing order, from a table (1 meter high) to the highest position over the patient’s head, using both arms and then bringing the pots back to the table; the exercise sequence was repeated for 5 minutes to simulate housework of storing pots; and (6) simulating taking a shower for 5 minutes while in a standing position. In order for the patients to avoid using PLB, they were required to breathe through a mouthpiece.
Use of ECTs
Four ADLs were chosen to be repeated, this time using ECTs, as follows: (1) walking on the inclined treadmill using PLB; (2) putting shoes on and off with the patient seated, without bending the thorax over the abdomen and patients had to lift up the shoe with one of their feet, cross that leg over the opposite thigh, and then put it on (or take it off) with their hands; (3) storing pots using PLB; (4) simulating showering but in a seated position and without bending the thorax over the abdomen, and for the patients to avoid PLB, they were required to breathe through a mouthpiece.
Statistical analysis
A sample size of 18 patients would have 80% power to detect a 150 mL difference in the IC from baseline to exercise 2 assuming an α error of 5%. A paired t-test was used to compare ICs before and after each ADLs task. Values are expressed as mean ± standard deviation. Pearson’s correlation coefficients were used to estimate the correlation between the ▵IC and body mass index, FEV1, RV, RV/TLC, and dyspnea. Numeric graphic displays were constructed using Graphpad program (GraphPad Software, San Diego, California, USA).
Results
Demographic and lung function parameters
Twenty-seven consecutive COPD patients were initially recruited for the study, of which nine were excluded for the following reasons: one patient due to uncontrolled arterial hypertension, one due to cardiac arrhythmia, two due to low SpO2 during the tests, one due to exacerbation during the study, one due to an orthopedic disease, one could not stabilize the tidal volume to obtain reproducible IC maneuvers, and two did not have a good understanding of how to perform the vital capacity maneuver. Thus, 18 patients (mean age: 65.8 ± 9.8 years) completed the study. Ten patients (55.5%) were classified as GOLD stage II, 7 (38.8%) as GOLD stage III, and 1 (5.6%) as GOLD stage IV. Demographic and lung data of the 18 COPD patients are shown in Table 1.
Demographic and lung function data of the 18 COPD patients.

COPD: chronic obstructive pulmonary disease; BMI: body mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLC: total lung capacity; RV: residual volume; IC: inspiratory capacity; PaO2: arterial pressure of oxygen; PaCO2: arterial pressure of carbon dioxide.
The patients had altered health status, as seen by the high St George’s Respiratory Questionnaire and Airway Questionnaire 20 total scores (45.2 ± 18.4% and 50.8 ± 21.2%, respectively). The mean dyspnea sensation (Basal Dyspnea Index; BDI score) was 7.9 ± 4.3. Eleven patients were eutrophic (61.1%), six were overweight (33.5%), and one was underweight (5.6%). Weakness of the respiratory muscles was not observed (data not shown).
IC evaluation during six ADLs
All six standardized ADLs without PLB or ECT induced DH, with a mean increase of more than 150 mL (Table 2).
Initial versus final IC after accomplishment of six ADLs by 18 COPD patients.a

IC: inspiratory capacity; COPD: chronic obstructive pulmonary disease; ADLs: activities of daily living.
aValues are expressed as mean ± SD.
Energy conservation techniques
Results of the use of ECTs for ADLs are presented in Figure 1. The use of ECT did not prevent patients from experiencing hyperinflation while walking on a treadmill for 2 minutes with 5% of inclination. Hyperinflation during movements when simulating taking a shower, lifting pots, and when putting on shoes associated to ECT was prevented with reduction in confidence interval (0.08, 0.12, and 0.05 mL, respectively). None of the patients had to interrupt any of the tasks due to respiratory symptoms. We show in Table 3 the proportion of patients that hyperinflated during ADL without and with ECT.

Impact of ECT on IC (ΔIC = without ECT – with ECT, in liter) in COPD patients accomplishing ADLs. ECT: energy conservation technique; IC: inspiratory capacity; COPD: chronic obstructive pulmonary disease; ADLs: activities of daily living.
Proportion of patients with DH during the ADLs without and with ECT.

DH: dynamic hyperinflation; IC: inspiratory capacity; COPD: chronic obstructive pulmonary disease; ADLs: activities of daily living; ECT: energy conservation technique.
The mean SpO2, HR, RR, and Borg change during ADLs accomplished without and with the use of ECT are shown in Table 4. The matrix correlation between studied variables are listed in Table 5. No significant correlation was found between Borg and dynamic pulmonary hyperinflation for all activities performed.
SpO2, HR, RR, and Borg D change during ADLs accomplished without and with use of ECTs.
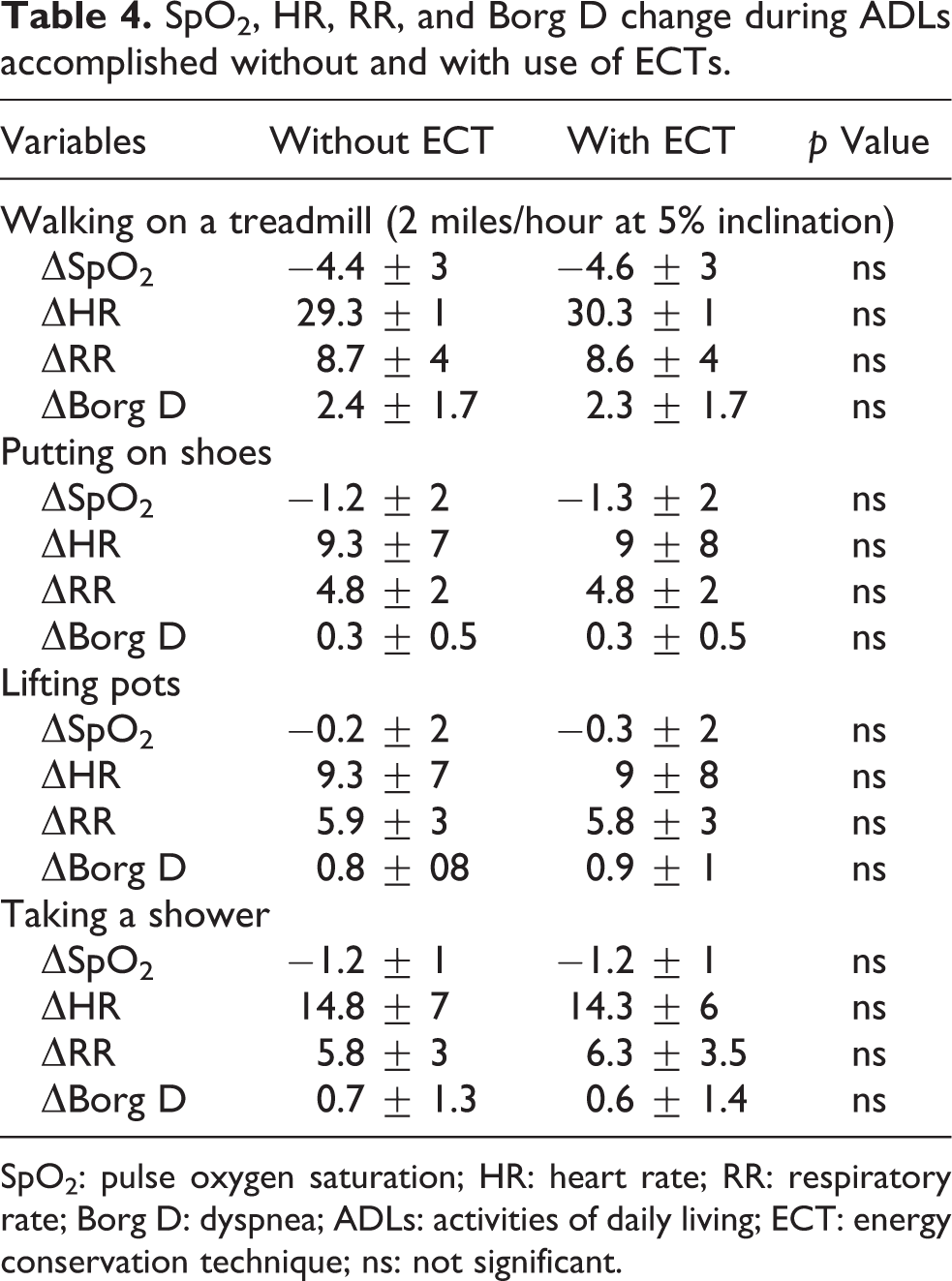
SpO2: pulse oxygen saturation; HR: heart rate; RR: respiratory rate; Borg D: dyspnea; ADLs: activities of daily living; ECT: energy conservation technique; ns: not significant.
Pearson correlation coefficients.
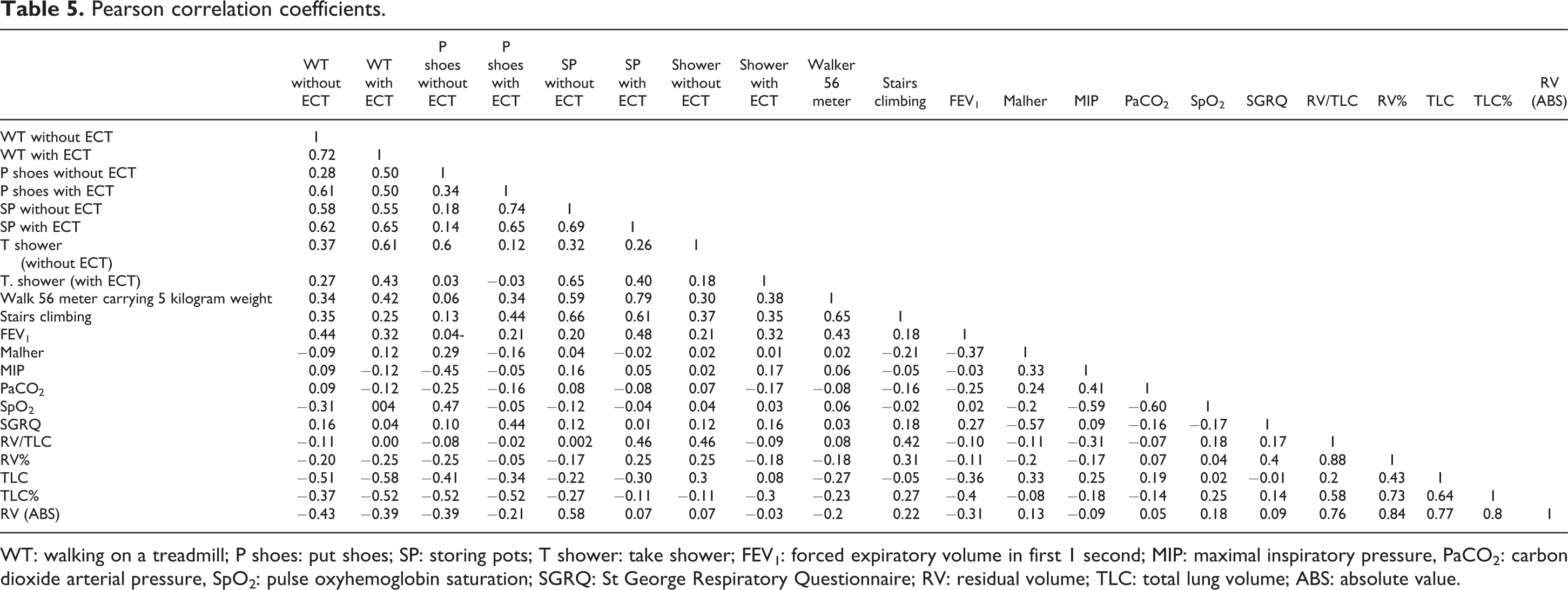
WT: walking on a treadmill; P shoes: put shoes; SP: storing pots; T shower: take shower; FEV1: forced expiratory volume in first 1 second; MIP: maximal inspiratory pressure, PaCO2: carbon dioxide arterial pressure, SpO2: pulse oxyhemoglobin saturation; SGRQ: St George Respiratory Questionnaire; RV: residual volume; TLC: total lung volume; ABS: absolute value.
Discussion
This study evaluated the induction of DH in moderate-to-very severe COPD patients while performing six standardized ADLs. In four of them we tested the use of PLB and other ECT as a possibility to prevent the induction of DH in the ADLs. The main results observed were that all six ADLs induced DH. However, the use of ECT prevented the generation of DH in three of the four ADLs tested (i.e. lifting pots, taking a shower, and putting on shoes) but with no reduction in dyspnea.
The six chosen ADLs were based on the ones commonly performed on a daily basis, which included both upper and lower limb movements and usually lead to dyspnea sensation. It has been shown that routine tasks performed by COPD patients demand high ventilatory and metabolic costs 9 and induce dyspnea. 12,14 The method used in this study to detect DH (variation in static IC) has been described in other COPD patient studies. 2 The 150 mL absolute change in IC adopted in this study is considered a clinically significant change. 2 Yan et al. 16 demonstrated that this method for measuring IC is simple and reproducible and reflects changes in functional residual capacity during exercise. 9
We observed that all six ADLs performed in this study induced DH. The highest level of DH occurred when the patients walked on a treadmill with 5% inclination at 2 miles/hour. It is known that activities that involve the lower limbs have a higher metabolic demand than activities involving only the upper limbs. 17,18 The association of lactic acidosis produced by the lower limbs oxidative metabolism and the occurrence of peripheral reflexes stimulate hyperventilation, and it is known that high ventilation has been implicated in the pathophysiological mechanism of DH induction. 19,20 Despite minute ventilation was not measured in our patients, we believe that this pathophysiological phenomenon accounted for the reduction in IC.
Pot-lifting task also induced a significant reduction in IC. Previous studies have shown that unsupported upper limbs activities are not well tolerated by COPD patients. This study shows that the limitation COPD patients present for this kind of task may be due to the occurrence of static and dynamic lung hyperinflation. 7,17 The recruitment of accessory muscles and the consequent thoracoabdominal dysynchrony may explain the dyspnea 11 these patients feel when accomplishing tasks with the upper limbs.
In a previous study, we showed that four routine ADLs involving upper limbs effort resulted in high metabolic and ventilatory demand. While normal subjects spent less than 20% of their oxygen consumption (VO2) peak to accomplish these activities, the COPD patients reached 50–60% of their VO2 peak. 9,21 Upper limbs activities in normal subjects induce an increase in sympathetic adrenergic tonus, resulting in vasoconstriction and contributing to a reduction in the regional blood flow to the upper limb and scapular muscles, what may lead to the development of lactic acidosis. We postulate that academia may contribute to the increase in ventilation and consequent DH in COPD patients. 22
Putting on shoes and performing movements simulating taking a shower also induced DH in our COPD patients. In both activities, patients had to bend the thorax over the abdomen. Bending the thorax leads to diaphragm compression, increases inspiratory muscle recruitment, and enhances minute ventilation, thereby contributing to DH. This mechanism has been reported previously in the literature. 9 Recruitment of the accessory muscles is expected to reduce the possibility of diaphragm fatigue. 19,22,23 While muscle fatigue might be a contributing factor in the pathophysiological DH phenomenon, no change in respiratory muscle strength was observed in our study.
Interestingly although ECT prevented the development of HD, they did not reduce the sensation of dyspnea. It is not clear why there was a lack of association of reduction of dynamic hyperinflation and dyspnea. Perhaps the subjectivity of the instrument used to measure dyspnea associated with a low understanding of the Borg scale by patients may have contributed to the occurrence of this result. 20,24
One of the novel findings of our study was that the use of simple ECT, such as not bending the thorax over the abdomen, prevented the development of DH in ADLs in tasks like taking a shower and changing shoes. While the use of ECT has been widely recommended for a long time, 24 to the best of our knowledge, this is one of few studies to show that ECT use might decrease pulmonary hyperinflation. However, the use of PLB, probably one of the most frequently recommended maneuvers by physiotherapists, did not change our COPD patients’ hyperinflation values when they walked on a treadmill. Although it is known that PLB breathing can modify the breathing pattern and lower the respiratory rate, 25 it is possible that in activities with a high metabolic demand, such as walking or carrying a weight, 23 PLB is not sufficient to prevent DH, as shown in our results.
We did not observe any correlation between IC change and HR, dyspnea sensation, or SpO2. However, we should point out that our study had no power to demonstrate these associations due to our sample size. These associations were not considered main objectives of this study.
The main clinical implication of this study is the suggestion that patients with COPD in more severe stage of the disease should always be instructed to use ECT during the performance of their ADLs, as they may contribute to prevent DH. Despite we have not observed less dyspnea during the use of ECT, other authors have shown this association. 25 Thus it is our belief that professionals involved in the rehabilitation process of COPD patients should promote the teaching of ECT as an obligatory part of treatment.
The main limitation of this study is not having had an unblended evaluation of the patients but the methods used for evaluation are somewhat objective and have proved to be valid and reliable which is what makes us believe it does not invalidate our data. Another possible limiting factor is the fact that we have not measured ventilatory and metabolic variables but the literature has studies showing the changes that ventilatory and metabolic variables undergo during exercise 17 or during the accomplishment of ADLs. 23
In a study by our group with COPD patients, with characteristics similar to the ones in this study, when performing activities that involved the upper limbs (sweeping the floor, erasing a blackboard, lifting pots, and changing light bulbs) presented an increase in the RR and in the use of the ventilatory reserve, justifying the genesis of dyspnea reported by them. 5 In another study with also COPD patients with similar characteristics, we observed that simple exercises with the arms developed dynamic hyperinflation and the likely mechanism for the DH showed increase in pulmonary ventilation, RR, inspiratory time over total breathing cycle ratio, and tidal volume over inspiratory time and reduction in expiratory time. 26
From this study with moderate-to-very severe COPD patients, it can be concluded that simple ADLs induces DH, which could play a role in the exercise limitation and dyspnea sensation felt by these patients. ECTs use might somewhat prevent the occurrence of DH and their use by COPD patients should be encouraged. In addition, further studies should examine the actual efficacy of those maneuvers in a wider range of ADLs and how they could decrease dyspnea in COPD patients and increase their performance during ADLs.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.