
Abstract
Oxygen is one of the commonest health-care interventions worldwide. This might suggest that health-care professionals (HCPs) would be knowledgeable and familiar with its uses and limitations. Yet it is apparent, through clinical audit, that oxygen is probably misunderstood by many HCPs. The aim of this critical interpretive synthesis (CIS) is to explore qualitative and quantitative literature in relation to HCPs beliefs and perceptions of oxygen therapy. A systematic search in Medline, Cinahl, Embase, British Nursing Index and PsychInfo using search terms, such as, oxygen therapy, chronic respiratory disease, HCPs and perceptions yielded 1514 studies of which 12 contained data relevant to the review question. Two reviewers independently screened the articles for eligibility against inclusion and exclusion criteria, and data were selected and synthesized with an integrative and interpretive approach using CIS. This allowed diverse empirical evidence to be synthesized to develop existing and new interpretations of data.Three synthetic constructs were interpreted from the available literature, namely, oxygen for symptom relief, levels of knowledge and understanding and oxygen as a therapy for HCPs. The literature alludes to deep-seated beliefs that exist. In order to enhance practice, these beliefs and cultures need to be challenged. Further research is needed to explore HCPs’ perceptions of oxygen therapy in order to inform the seemingly resistant adoption of evidence based practice in relation to oxygen.
Introduction
Oxygen is one of the most prolific health-care therapies used in the developed world. Its abundance might suggest that health-care professionals (HCPs) would be knowledgeable and familiar with its uses and limitations. Yet it is apparent, through poor prescribing and administration practices, that oxygen is probably misunderstood by many HCPs. This has been demonstrated in acute care, where despite reported prevalence of 24% use in all inpatients, 1 and in emergency settings where 34% usage 2 has been observed, suboptimal quality of care has been recorded. 1 –4
Similarly, a report produced by the Royal College of Physicians 5 in response to spiralling costs of domiciliary oxygen therapy uncovered poor prescribing practices and follow-up of patients, which led to major changes in prescription and provision of home oxygen services in England and Wales. 6 Yet despite these changes, poor practice and variations in practice persist. 7,8 The reasons for failure to alter practice in accordance with emerging evidence remain an enigma.
The British Thoracic Society (BTS) suggest that a high proportion of medical oxygen is possibly administered because most clinicians believe that oxygen can alleviate breathlessness, 6 but there is no evidence supporting this claim. Indeed the evidence base for oxygen therapy per se is lacking, with most criteria and guidelines for oxygen therapy is supported by evidence that has evolved based on individual cases and consensus opinion rather than sound experimental research. This has often led to the adoption of a priori knowledge with the need for robust controlled clinical trials overlooked.
It is further suggested, possibly as a consequence of a lack of empirical evidence, that a major problem contributing to poor prescribing practices is that HCPs often receive conflicting information and advice about oxygen therapy during their training and clinical careers. There appears to be confusion about the entire area of oxygen prescription and use, 6 but again there is no supporting evidence. The problem appears to become self-perpetuating as anecdotal evidence suggests that the same erroneous beliefs are exposed to individuals receiving oxygen therapy, their carers and the general public. Subsequently, this may lead to unrealistic expectations and poor adherence to prescribed oxygen therapy.
Despite growing acknowledgement of this issue, it is not clear from the literature where the roots of these fallacies lie, and indeed, whether this is a result of tradition, lack of knowledge regarding the indications and administration of oxygen therapy, or misunderstanding of basic physiological principles of oxygen per se. In order to address this clinical paradox, there is a need to identify reasons for enduring poor practices. The aim of this critical interpretive synthesis (CIS) therefore is to explore the literature in relation to HCPs’ beliefs and perceptions of oxygen therapy in order to provide a platform for further investigation.
Method
The dearth of literature addressing the review question directly, together with the diversity and complexity of the literature available, directed the review towards an integrative and interpretive approach.
CIS, a variant of meta-ethnography was utilized, 9 allowing explicit integration of qualitative and quantitative evidence through an interpretative process. CIS draws upon conventional systematic review methodology, whilst allowing discretion in study selection to include articles that may contribute to findings whilst not necessarily answering the review question directly. The use of the ‘authorial voice’, in relation to the first author’s experience and knowledge of oxygen in the clinical context, in both selection of literature and interpretation is a further defining feature of CIS. 9
Search strategy
A systematic approach to searching, locating and retrieving relevant literature was adopted. 10 The initial search identified articles relating to both patients’ and HCPs’ perceptions of oxygen therapy. Findings from HCPs’ perceptions are reported here. Findings from patients’ perceptions have been reported separately.
Medline (1950–2014), Cinahl (1981–2014), Embase (1980–2014), British Nursing Index (1985–2014) and PsychInfo (1806–2014) were searched via Evidence Search (www.evidence.nhs.uk) using keywords oxygen therapy, chronic respiratory disease, healthcare professionals and perceptions. Term variants and synonyms were combined and searched using the Boolean ‘OR’ (e.g. oxygen therapy OR O2 therapy). The Boolean ‘AND’ combined different facets. Truncation (*) was utilized to capture plurals and spelling variants (e.g. Oxygen therap*). To improve focus advanced search operators for phrase searching (“”) were used. Studies were restricted to English language only with no date or publication type restrictions applied.
A search of grey literature and the wider Internet was conducted to minimize publication bias. Hand-searching key journals together with key respiratory conference proceedings and ‘citation snowballing’ 11 supplemented database searches, ensuring the inclusion of literature not yet indexed in databases. The search was undertaken on 21 December 2011 and rerun on 12 March 2014 to capture further relevant studies published since the initial search.
Inclusion criteria and study selection
The initial search included articles relating to both HCPs’ and patients’ perceptions of oxygen therapy. This resulted in 1503 articles identified, and titles and abstracts were considered for these articles. From these 1503 articles, 179 articles were selected for further consideration. Two reviewers independently screened the articles for eligibility against inclusion and exclusion criteria (Table 1) and relevance to the research question. The decision deferred the quality appraisal phase in the event of disagreement. Fifty-nine full-text articles were finally selected for quality assessment. The flow chart (Figure 1), adapted from PRISMA (Preferred Reporting Items for Systematic review and Meta-Analysis), 12 provides a summary of the search outcome.

Flowchart of study selection.
Inclusion and exclusion criteria.

HCP: health-care professional.
Quality assessment
Exclusion of studies on the grounds of poor quality is a leading contention in relation to quality appraisal in integrative reviews and in particular CIS. 9,13,14 Qualitative research is regarded as an interpretative act 15 and appraising the quality of articles requires more than a simple scoring system. Dixon-Woods et al. (2006) argue that studies that can potentially add to a review’s findings should therefore be quality appraised on their own merit and within the context of the review question, and that content and relevance of findings is an additional key consideration. The pro forma therefore included the key aspect of implications and usefulness to the review question. As the principal focus of most studies was not directly related to the review question, this was an important aspect.
A hybrid quality appraisal/data extraction sheet was developed based on the criteria for disparate data as suggested by Hawker et al. 16 This allowed identification of various methodological features without excluding studies of poorer quality. 17 Using Hawker et al.’s protocol for assessment a score of 1–4 is assigned to each of 10 criterion resulting in an accumulative score that indicated the overall assessed methodological rigour of each empirical study (ranging from 10 (very poor) to 40 (good)). Second checking by an independent reviewer (DL) allowed differences to be resolved by discussion and consensus. The process of quality appraisal, including relevance, reduced the number of studies from 59 to 51.
At this stage, articles were separated into two categories, namely, patients (42 studies) and HCPs (12 studies), with a total of 51 articles (three articles being eligible for both). Findings from HCPs’ perceptions are reported here. Findings from patients’ perceptions are available in a companion article. 18
Data extraction strategy
Data extraction was facilitated using a pro forma which detailed characteristics and quality appraisal of included studies, including relevance. Data extraction was undertaken by the lead researcher and independently checked by a second reviewer (DL).
Synthesis of the extracted data
The current review adopted criteria for data synthesis set out by Flemming. 14 This involved the article being read and understood in relation to both itself and the research question. Relevant data were extracted and translated, through identification of concepts, themes and metaphors and developed into synthetic constructs. Exploring relationships between constructs allowed explanatory accounts to be suggested in the form of synthesizing arguments. Integration of evidence in this way, from across studies, allowed new interpretations of data, which is demonstrably grounded in existing evidence. 17
Findings
None of the studies addressed the research question directly. Studies were therefore selected on the basis that some aspect of, or reference to, the study’s findings included HCPs’ perceptions of oxygen therapy.
The final selection of 12 articles consisted of varying methodological approaches, quality, countries of origin and professional groups. The number of participants in each study ranged from 12 to 1051. The methodological quality of selected studies varied, but no articles were excluded on the basis of quality as discussed previously. The final selection of articles related to HCPs’ perception is summarized in Table 2. In addition, representation from the literature is detailed in Table 3. This allows assessment of the grounding of constructs in the original literature.
Grid of main points from literature reviewed – study characteristics and HCPs’ perceptions.

RCT: randomized controlled trial; HCP: health-care professional; LTOT: long-term oxygen therapy; COPD: chronic obstructive pulmonary disease.
Grid of themes – HCPs.
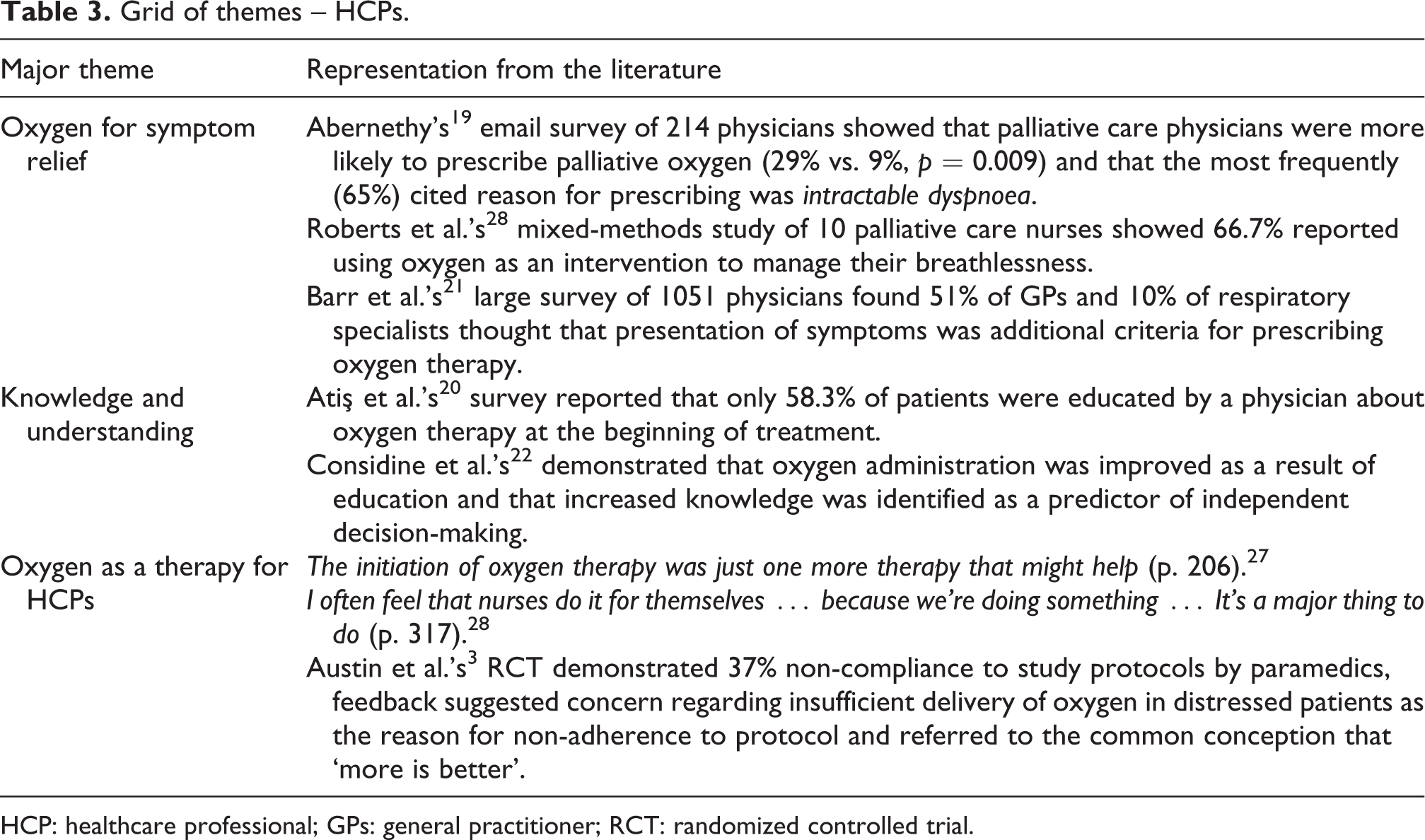
HCP: healthcare professional; GPs: general practitioner; RCT: randomized controlled trial.
Literature pertaining to perceptions from the HCPs’ perspective is very limited. The final selection of studies identified 13 articles of which 4 were excluded at quality appraisal. The reasons for exclusion included the article’s focus was chronic obstructive pulmonary disease (COPD) generally with no specific mention of oxygen, two articles did not relate to perceptions and one was a duplicate publication of the same study. Further details and references of excluded studies are detailed in Table 4. In addition, three articles 25,27,28 selected in the patients’ perception review were also included in the review of HCPs, bringing the total of included studies to 12. Heterogeneity of design and methods was apparent in the studies selected (Table 2).
Reasons and references for exclusion of studies.

HCP: health-care professional; COPD: chronic obstructive pulmonary disease.
Findings were very limited for HCPs due to the paucity of evidence. Three synthetic arguments were constructed from the available literature, namely, oxygen for symptom relief, levels of knowledge and understanding and oxygen as a therapy for HCPs. These constructs, together with the number of articles that contributed to each, are outlined in Tables 3 and 5.
Grid of themes – HCPs.

HCP: health-care professional; COPD: chronic obstructive pulmonary disease.
Oxygen for symptom relief
The notion of HCPs perceiving oxygen to relieve breathlessness was common in the literature and appeared in half of the considered articles. Abernethy 19 published the results of an email survey of 214 physicians (93 palliative care physicians and 121 respiratory physicians). Primarily intended to define the necessary duration of a clinical efficacy study regarding palliative oxygen therapy, the survey captured habits of prescribing oxygen therapy for palliative care including the frequency and indications. The findings showed that palliative care physicians were more likely than respiratory physicians to prescribe palliative oxygen (29% vs. 9%, p = 0.009) and that the most frequently (65%) cited reason for prescribing was ‘intractable dyspnoea’. Despite a low response rate (33%) and crude methodology, the survey demonstrates that the majority of responding clinicians believe that oxygen relieves dyspnoea.
Stringer et al. 29 similarly surveyed physicians’ prescribing practices of palliative oxygen therapy. This telephone survey reported variability in prescribing practices attributed to both a lack of evidence and clear guidelines. Based on hypothetical scenarios, physicians were assessed in response to specified cues. Cluster analysis revealed three patterns of response, namely, those who prescribed in the presence of hypoxia regardless of symptoms, those who prescribed only when both hypoxia and symptoms were present and those prescribing for breathlessness alone. Adding a ‘dummy factor’ on the effect of spousal concern revealed an increasing tendency to prescribe, probably related to expectation from carers and perhaps patients. Ultimately the study, although a small sample of 17, demonstrated that uncertainty and inconsistency exists when physicians are faced with the decision whether to prescribe oxygen to palliative care patients. The article’s authors suggest that this may be a reflection of inadequate understanding of pathophysiology and treatment and that the decision to use oxygen is often based upon individual past experiences and biases.
Roberts et al. 28 studied the experience of dyspnoea in the last year of life. The mixed-methods study of 10 patients with late-stage lung cancer and the nurses providing their care provided data to investigate the phenomenon of dyspnoea, as experienced during the last weeks of life. A triangulated approach included patient self-report survey, chart audits (to record incidence and management of dyspnoea) and patient and HCP interviews. Of the 10 patients interviewed, 7 recalled no suggestions made by the nurse regarding how to manage their breathlessness, although 66.7% of nurses reported using oxygen as an intervention. The study revealed an inconsistent understanding; with reference to oxygen therapy, some nurses reported that it was helpful and that it should be ordered as soon as dyspnoea was apparent, whilst others claimed that although it wasn’t clinically therapeutic they believed it had a symbolic benefit (p. 317). Several nurses were of the opinion that oxygen provided psychological comfort to both patients and their families. Whether this notion can be extended to HCPs themselves will be explored later.
Barr et al. 21 recorded patient and physician perceptions of COPD in a large survey (1050 physicians and 1023 patients) in the United States. Although the main focus of the study was COPD, in relation to oxygen therapy, physicians reported confusion regarding treatment options; 51% of general practitioners and 10% of respiratory specialists thought that presentation of symptoms was additional criteria for prescribing oxygen therapy.
Adding to the synthetic construct of oxygen for symptom relief, a Turkish questionnaire survey aimed at exploring issues of compliance of long-term oxygen therapy (LTOT) by patients, provides some insight into the messages that HCPs provide. 20 Thirty-three percent were told only to use oxygen when they were short of breath and only 28.2% reported that they used oxygen for more than 15 hours per day (the recommended evidence-based duration necessary to obtain long-term clinical benefit). Although limited by the response rate (34.5%) and its geographical specificity (in Turkey patients purchase their own oxygen), this study adds to the elusive, but anecdotally common, belief that oxygen therapy relieves breathlessness.
The limited insight found in the literature relating to how HCPs prescribe and use oxygen provides an inconsistent approach. It does however appear prevalent that it is frequently used for, and HCPs appear to believe it relieves dyspnoea. It has been demonstrated that pressure from carers influences prescription 29 ; a phenomenon that may be linked to expectations of both patients and carers.
Levels of knowledge and understanding of HCPs
Half of the articles considered referred to HCPs’ knowledge and understanding of oxygen therapy. Glaab et al. 24 undertook a national mail survey of 845 physicians (486 generalists and 359 specialists) in Germany to investigate compliance to guidelines when prescribing. Although primarily concerned with generic COPD guidelines, there is some limited reference to oxygen therapy. LTOT was generally regarded as an effective measure for improving the quality of life and symptoms rather than prolonging life expectancy. The knowledge of effect on survival rate was higher in respiratory specialists than generalists (p < 0.0001).
Atiş et al.’s 20 survey reported that 58.3% of patients were educated by a physician about oxygen therapy at the beginning of treatment, whether the rest received any form of education is not clear. Logistical regression identified the likelihood of achieving compliance increased 4.5-fold (confidence interval 2.27–9.13, p < 0.001) when education was provided. This relationship between patient compliance and the level of education supports the findings of an earlier study by Pepin et al. 26 This French survey questionnaire of 219 physicians and 564 patients assessed patient compliance and prescribing practices for LTOT. Although 87% of patients were prescribed over 15 hours per day of oxygen therapy (as reported by the physicians), only 45% reached this target. Again logistical regression showed that patients receiving a follow-up education session increased the likelihood of receiving effective treatment 4.5-fold (CI 2.3–9.1). The study concluded that supplementary education regarding LTOT, given by a nurse or physiotherapist, was an important factor for increasing patient’s compliance to therapy. Clearly then education of the patient is central to understanding the therapy and consequently compliance, but fundamental to that must be the knowledge and understanding of the HCPs themselves.
Considine et al. 22 demonstrated that the use of supplemental oxygen was improved as a result of educating the HCPs in the acute setting and that increased knowledge was identified as a predictor of independent decision-making. The quasi-experimental design sets out to test the assumption that an increase in nurse’s knowledge, though a self-learning package, improved clinical decisions. Pretest scores were comparable (p = 0.091), whilst posttest scores between the experimental and control group showed a statistically significant improvement (19.31 ± 3.56 vs. 13.05 ± 3.76; p = <0.001). Eighty-seven percent of nurses in the study reported making clinical decisions about oxygen therapy on a daily basis (91% of those decisions were autonomous). The calibre of these decisions clearly has the potential to influence patient outcomes and therefore it is important to consider factors that influence the acquisition of knowledge.
A further study by the same Australian group 23 explored specifically the effect of education on clinical decisions regarding emergency oxygen therapy. Utilizing a similar design, this smaller study of 20 emergency department nurses tested nurses’ decision-making skills, rather than knowledge, following completion of the educational intervention. The results from this study were variable with some changes in hypothetical management of patients seen, in particular device selection, but in other aspects (e.g. the parameters used for assessment) no change was demonstrated.
It is apparent from the literature that education of HCPs is important and that education given to patients has the potential to improve compliance and, therefore, hypothetically, clinical effectiveness.
Oxygen as a therapy for HCPs
The synthetic argument of oxygen as a therapy for HCPs is probably the most ambiguous construct derived from the literature. Nonetheless, it is evident in four of the reviewed studies that such a notion exists and seems a familiar explanation for the common prescription of oxygen therapy for non-hypoxic patients. Relating to patients’ fears and restrictions with palliative oxygen, a study by Reinke et al., 27 though very limited in its reference to HCPs, refers to physicians’ recognition of oxygen therapy as a milestone in a patient’s condition; one physician stating, ‘The initiation of oxygen therapy was just one more therapy that might help’ (p. 606). This quote seems to epitomize the often felt frustration from HCPs regarding the management of the intractable symptom of dyspnoea.
Roberts et al.’s 28 mixed-methods study of lung cancer patients’ experience of the last year of life draws on this idea further. With reference to the notion of oxygen providing palliative comfort to keep patients at home and ‘happy’, one nurse wondered whether the psychological benefit of oxygen was as relevant to the patients and families as it was to the nurses. ‘I often feel that nurses do it for themselves … because we’re doing something …’. 28
This rare recording of an anecdotally common perspective gives a potential insight into HCPs’ rationale for prescribing or recommending oxygen therapy. This insight seems to be potentially the most elusive with regard to the variability and inconsistencies of oxygen prescription and would support Considine’s and Botti’s 23 notion that factors other than knowledge and education may influence clinical decision-making.
A further tentative reference to the prospect of oxygen being given to relieve HCPs’ need to help patients manage dyspnoea, and the possibility of an entrenched culture, is alluded to by Austin et al. 3 This well-designed and conducted randomized controlled trial set in Tasmania tested outcomes in relation to high-flow versus titrated oxygen in the pre-hospital care of COPD patients. The main findings from this landmark study demonstrated that titrated oxygen significantly reduces hypercapnia, respiratory acidosis and mortality. The researchers discovered a lower than expected adherence to study protocols. Of the 214 patient records, 37% showed that received treatment did not comply to study protocols (56% in the titrated arm and 21% in the high-flow arm). In the titrated arm, all violations involved administration of high-flow oxygen at some point in the pre-hospital care. The authors muse that this is probably a result of entrenched culture and training in emergency medicine. Chart reviews found no evidence of equipment malfunction, requests from patients, or lack of protocol understanding, but the authors report that feedback from some paramedics indicated concern regarding insufficient delivery of oxygen in distressed patients and referred to the common conception that more is better. This study is potentially important in that it does expose, intangibly, the notion of culture and the need to explore and substantiate the reasons why this exists is manifest. Although fundamentally relating to the efficacy and detrimental effects of oxygen in the acute setting, the existence of persistent beliefs and entrenched practices is apparent.
The literature pertaining to perceptions from HCPs is very limited but from what evidence is available there appears to be a persistent belief that oxygen is useful for management of dyspnoea. There is also some degree of evidence that using oxygen for patients in such a way helps HCPs and has the potential to offset guilt and frustration at not being able to help patients.
Discussion
Inconsistency of reported beliefs, understanding and variations in clinical practice, even with respiratory specialists, dominate this limited sample of empirical evidence. The reasons for inconsistency in the indications and use of oxygen have been cited as a result of a lack of clear guidelines, endorsed through the obscure nature of lucid information and directives.
The relationship between knowledge and clinical practice is clear. Transfer of this knowledge to patients is part of the therapeutic relationship, but it can be contested as beneficial if that knowledge is not grounded in evidence but in misplaced beliefs and misconceptions. It is suggestive that the faith in HCPs 18 that patients have, on occasion, may be poorly placed.
It has been suggested that factors other than knowledge may influence clinical decisions. 23 What these factors are remains obscure and further research is warranted. Attempts have been made previously to uncover perceptions of oxygen therapy and the implications that this may have on clinical decision-making, but contributing factors identified tend be those that affect efficacy of oxygen 30 and patient compliance 20,25,26 rather than culture.
Respiratory specialists appear to have a greater knowledge and understanding regarding oxygen, as may be expected, it can be argued however that with the prevalence of prescriptions and use from non-specialist HCPs that the prescriber should always have the relevant knowledge and understanding to enable safe clinical decision-making.
The overuse and misunderstanding of oxygen therapy by HCPs has been alluded to in other literature, 31 –35 nevertheless there is very little evidence to verify this and a dearth of empirical evidence to substantiate why these misunderstandings appear to be so prevalent among HCPs. It is often cited that a culture exists whereby oxygen is given automatically to patients who present critically ill or dyspnoeic. 36 It appears that this culture may be deep-seated and may in fact be so ingrained that it actually provides relief for HCPs themselves as they feel they are doing ‘something’.
This review overall offers some, albeit limited, insight into the inconsistencies of oxygen prescription and administration, the importance of education and its potential relationship to clinical efficacy and a glimpse at a culture and an innate response that may be obstructive to HCPs practicing evidence-based care.
Summary and recommendations
The literature is not very forthcoming in enlightening beliefs and perceptions of HCPs regarding oxygen therapy. There appear to be clues, but these lack tangibility and verification. It is proposed that this missing perspective may serve to illuminate the problems associated with poor adherence to guidelines and recommended practice concerning oxygen therapy and clearly further research is this area is warranted.
It is interesting to note that overall the methodological qualities of studies pertaining to HCPs are poor, with a seemingly over-reliance on survey as means of data collection. Response rates, especially from non-specialist physicians are recorded as low, despite strategies to increase returns. The rudimentary survey approach to gathering information can overlook some of the more deep-seated roots of beliefs, culture and practice that may inform the seemingly resistant adoption of evidence-based practice in relation to oxygen.
HCPs can be considered to have immense power over patients’ lives in what they prescribe and advocate. With the possibility that perception is shaped by several influences including media, knowledge, cultural, historical, professional and social, these factors appear vague in the literature but should not be disregarded as potential sources of antecedents. The findings presented here highlight possible misconceptions and potential influences regarding oxygen therapy. Further exploration of the perceptions regarding oxygen therapy from both HCPs’ and patients’ perspectives are needed in order to explore these potential influencing factors in order that recommendations to address these can be made.
From the literature it can be deciphered that knowledge affects clinical practice with regard to oxygen therapy, yet practice is not always influenced by education. It appears that it is difficult, even in a controlled experimental situation, to rise above deep-seated beliefs, especially when a patient is struggling to breathe. Yet in order to improve practice, with regard to the safety and efficacy of oxygen therapy, these beliefs and cultures need to be challenged.
Strengths and limitations of the review
By casting a ‘wide net’, the high sensitivity of the initial search could be considered as the strength of the review. The incorporation of representation from the literature is a further strength that demonstrates grounding in the original data and is a characteristic of CIS. 9 The use of the author’s experience in interpretation is a key to the explanation of data and construction of the synthesizing arguments. Whilst drawing upon personal experience and preconceived ideas that can be considered a threat to impartiality, it can alternatively be argued that the insight brought to the review through expertise was true to CIS and the fulcrum to developing the synthetic constructs.
The quality of the reporting of included articles was an inherent weakness with many studies not being well described and methods of analysis not always explained. This issue of poor quality in write-up, as opposed to poor quality of methods, has been identified by other authors. 16 Ultimately, most literature focuses on diverse objectives, such as HCPs understanding of disease and treatments, illness transition and efficacy of interventions rather than actually what HCPs think or believe about oxygen, and this limits the review’s ability to address the research question directly.
The material selected displayed heterogeneity, being based on differing philosophical and scientific assumptions. In particular, most studies utilized a quantitative design with retrospective data and an over-reliance on survey. In the absence of directly relevant studies, the use of CIS enabled the construction of synthetic arguments, which informs and gives some foundation to this elusive phenomenon. The use of reflexivity, as advocated with this interpretative review methodology, 17 facilitated consideration of the review methods and the process of synthesizing both original data and the researchers’ interpretations of these data.
Footnotes
Acknowledgement
I would like to thank Dr Dave Lynes, Edge Hill University, for his guidance with study selection and data extraction.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declared no conflict of interest.